-
7/25/2019 Costos SV Belize
1/11
326 Rev Panam Salud Publica 28(5), 2010
Economic impact of fatal and nonfatalroad traffic injuries in
Belize in 2007
Ricardo Prez-Nez,1 Martha Hjar-Medina,2,3 Ileana
Heredia-Pi,4
Sandra Jones,5 and Eugnia Maria Silveira-Rodrigues6
Objective. To estimate the economic cost of road traffic
injuries in Belize in 2007.Methods. A cross-sectional study was
conducted using secondary cost data, assuming thehealth system and
social perspectives. Epidemiologic information was obtained from
the mor-tality database, the national hospital discharge database,
and administrative records from po-lice and the Ministry of Health.
A health provider survey was carried out in order to estimatethe
postdischarge ambulatory utilization figures. Direct cost was
estimated with the World
Health Organization WHO-CHOICE (CHOosing Interventions that are
Cost Effective) data-base. Prehospital costs were obtained from the
Belize emergency response team. After estimat-ing years of
potential life lost using the Belize life expectancy for 2008 and
methodology pro-posed by the Pan American Health Organization, the
indirect cost associated with prematuredeath was estimated with the
human capital approach. Total estimation of road traffic
injurieseconomic costs used a decision tree model approach.
Multiway sensitivity analysis was usedto incorporate uncertainty in
the estimations.Results. Sixty-one people died due to road traffic
injuries during 2007, 338 were hospital-
ized, and 565 people were estimated to be slightly injured. A
total of 2 501 years of potentiallife were lost in Belize due to
premature death, with a total economic cost of US$11 062 544.This
figure represents 0.9% of the Belize gross domestic product. Direct
cost was estimated atUS$163 503, of which 2.4% was spent on
fatalities, 46.7% on the severely injured, and 50.9%on the slightly
injured.Conclusions. The economic cost estimations make clear the
need to prevent road traffic in-
juries with a strategic and multisectoral approach that focuses
on addressing the main prob-lems identified.
Accidents, traffic; health care costs; costs and cost analysis;
Belize.
ABSTRACT
In recent years, there has been a signif-
icant increase in the number of collisionson major highways and
roads in Belize.
Between 2004 and 2006, the Government
Information System of the Police Depart-ment reported
approximately 6 295 colli-
sions, of which 128 were identified as
fatal, resulting in 143 deaths. Most of thedeaths occurred in
2004, with a slight de-crease in 2005 and 2006. Statistics fromthe
Ministry of Health indicate that in2005, death as a result of road
traffic in-
juries (RTI) was identified as the fourthleading cause of death
in general, regard-less of age and sex (1). The adjusted mor-tality
rate due to RTI in 2006 was 15.4 per100 000 population. The country
has laws
Key words
Investigacin original / Original research
Prez-Nez R, Hjar-Medina M, Heredia-Pi I, Jones S,
Silveira-Rodrigues EM. Economic impact offatal and nonfatal road
traffic injuries in Belize in 2007. Rev Panam Salud Publica.
2010;28(5):32636.
Suggested citation
1 Health Systems Research Center, NationalInstitute of Public
Health, Cuernavaca, Mexico.Send correspondence to: Ricardo
Prez-Nez,[email protected].
2 Population Health Research Center, National Insti-tute of
Public Health, Cuernavaca, Mexico.
3 Pan American Health Organization/World HealthOrganization
Collaborating Centre for Research onInjuries and Violence,
Cuernavaca, Mexico.
4 Survey and Evaluation Research Center, NationalInstitute of
Public Health, Cuernavaca, Mexico.
5 Pan American Health Organization/World HealthOrganization,
Belize Country Office, Belize City,Belize.
6 Pan American Health Organization, SustainableDevelopment and
Environmental Health Area,Washington, DC, United States of
America.
-
7/25/2019 Costos SV Belize
2/11
Rev Panam Salud Publica 28(5), 2010 327
Prez-Nez et al. Economic impact of road traffic injuries in
Belize Original research
that cover speed limits, blood alcoholcontent (0.08%), helmet
use, and seat beltuse (although not all seating positions
arecovered). However, application of theselaws was considered very
weak. There isnot a law for use of child restraints (2).
RTI can have a significant negative im-pact on a country at all
levels, as they
cause a large number of sick days and anelevated amount of
healthy life yearslost. These factors have serious conse-quences on
society as a whole. In Mexico,for example, it has been documented
thatRTI are the second leading cause of or-phaned children, which
has implicationsin terms of poverty perpetuation in low-and
middle-income countries such asMexico (3). Moreover, since RTI
affect theyoung population in its most productiveyears, the
economic cost in terms of med-ical treatment, rehabilitation, and
loss ofproductivity tends to be high, with eco-
nomic repercussions in societies (3, 4).In the United States of
America, the
costs of motor-vehicle-related fatal andnonfatal injuries in
2005 exceeded US$99
billion. Costs associated with motor ve-hicle occupants fatal
and nonfatal in-
juries accounted for 71.0% ($70 billion) ofall
motor-vehicle-related costs (5). InBrazil, the cost of road traffic
accidentson highways amounted to US$10.0 bil-lion per year, which
is equivalent to 1.2%of the Brazilian gross domestic product(GDP).
Among the examined cost ele-ments, loss of production had the
great-
est economic impact, followed by vehicledamage and medical
costs. Fatal acci-dents had the highest mean valueUS$200 000 per
accidentshowing thatthe more severe the accident, the higherthe
cost. The total cost can be evenhigher should the costs of
environmentaldamage and posttraumatic stress disor-der be included
(6).
Not enough data are available to de-termine accurately the cost
of RTI in Be-lize. In order to understand the need foraction, it is
imperative that a comprehen-sive understanding of the cost of RTI
be
developed. For that reason, there is anurgent need to calculate
the economiccost of RTI in Belize and to evaluate theconsequences
that current RTI rates rep-resent for Belize, which will
providevaluable information in terms of injuryprevention and safety
promotion. Thisinformation will serve not only to iden-tify the
economic cost from a publichealth perspective but also to show
the
potential economic benefits from reduc-ing RTI by undertaking
road safety mea-sures such as developing and imple-menting
appropriate interventions (witha multisector approach). The main
objec-tive of this study was to estimate the eco-nomic costs
(direct and indirect) of fataland nonfatal RTI in Belize in 2007
from
health system and social perspectives.
METHODS
Study population
All road traffic injuries in Belize in2007 were included in this
study accord-ing to ICD-10 (7) criteria, which includethe following
ICD-10 codes for fatal andnonfatal RTI: V02V04 (.1, .9), V09 (.2,
.3,.9), V12V14 (.3.9), V19.4V19.6, V20V28 (.3.9), V29V79 (.4.9),
V80.3V80.5,V81.1, V82.1, V83V86 (.0.3), V87.0
V87.8, V89.2, and V89.9. All injuries werecategorized in three
mutually exclusiveseverity categories following previousproposals
(8):
Fatal injury: an injury that causes thedeath of the injured
person in the first30 days after the accident occurred.The 30-day
definition of a road trafficfatality proposed by the World
HealthOrganization (WHO) was used, al-though the official Belize
definition in-cludes all people who die within a yearafter the
collision (9). In order to facili-
tate international comparisons it wasimportant to make this
adjustment.
Nonfatal severely injured: either aperson remains in the
hospital as aninpatient or any one of the followinginjuries is
sustained regardless ofwhether the individual is detained inthe
hospital: fractures, concussions,internal injuries, crushing,
severe cutsand lacerations, and severe generalshock requiring
medical treatment.This category includes deaths thatoccur after 30
days.
Nonfatal slightly injured: a minor in-
jury such as a cut, sprain, or bruise.
Data collection and confirmation ofvariables
A secondary database analysis wasundertaken in order to estimate
epi-demiologic information. Fatal injurieswere obtained from a
mortality databasethat contained all deaths that occurred
during 2007. Serious injuries were ob-tained from the national
hospital dis-charge database, which contained all dis-charges
during 2007. This informationwas used to estimate the total
numberof people hospitalized (assuming theyall had serious
injuries). Administrativerecords from the Belize Police Depart-
ment were used to estimate the numberof slightly injured people
as informationfrom the health sector was not availablefor the
number of slightly injured peoplewho visited the emergency room.
The re-liability of this information is not knownwith certainty,
but it was the best infor-mation available. Finally,
informationabout population figures was obtainedfrom the World Bank
online
database(http://ddp-ext.worldbank.org/ext/DDPQQ/member.do?method=getMembers&userid=1&queryId=135).
Estimation of direct costs included ex-
penditures for medical care and treat-ment such as ambulance and
prehospitalcare services, emergency room use, hos-pital care,
physician services, nursinghome care, drugs and other medicalneeds,
postdischarge ambulatory med-ical consultations, and
rehabilitation.Categories included for each severitylevel group
depended on the availabilityof information.
Unitary cost data were obtained asfollows:
Ambulance and prehospital care ser-
vices: estimates for ambulance andprehospital care services used
sec-ondary data provided by the BelizeEmergency Response Team
(BERT).With a top-down approach, the totalexpenditure figures of
this institutionwere prorated by all services providedin order to
estimate an approximatecost per run. Total figures correspondto the
sum of the following cost cate-gories: salaries, fuel,
maintenance,utilities, medical supplies, insurance,and equipment.
Medical supplies aresubsidized by the Belize Ministry of
Health. In the same way, maintenanceis subsidized by Cisco
Construction(free labor). This cost was assumed foreach of the six
districts that divide thecountry, although BERT services
areprovided only in Belize district.
Hospitalization, emergency room hos-pital-based services, and
ambulatorymedical care costs: secondary data fromthe WHO-CHOICE
(CHOosing Inter-
-
7/25/2019 Costos SV Belize
3/11
328 Rev Panam Salud Publica 28(5), 2010
Original research Prez-Nez et al. Economic impact of road
traffic injuries in Belize
ventions that are Cost Effective) data-base were used to
estimate direct costs(available from http://www.
who.int/choice/country/blz/cost/en/print.html). Information on
specific econo-metric techniques used to estimatecountry-specific
costs is available else-where (10). Cost per bed-day represents
only the hotel component of hospitalcosts, including personnel,
capital, andfood costs but excluding drugs and di-agnostic tests.
Cost per outpatient visit
by hospital level and cost per visit at ahealth center include
depreciated capi-tal items but exclude drugs and diag-nostics (10).
All costs in this study arepresented in US dollars after
convertingthem to 2007 Belize dollars by meansof the national
consumer price index(available from http://www.statistics
belize.org.bz/dms20uc/dynamicdata/docs/20100901211434_2.pdf).
Costs ac-
crued after a year or more were dis-counted at annual rates of
3% and 5%.
Utilization figures were obtained asfollows:
Emergency ambulance services: esti-mated by using a database
containingall emergency ambulance services pro-vided by BERT on RTI
patients during2007. Although this information wasonly for Belize
district, it made it pos-sible to estimate the proportion of
se-verely injured people who received
ambulance and prehospital care ser-vices for the entire
country.
Ambulatory health care services: to es-timate postdischarge
utilization figures,a health provider survey was carriedout.
Experienced medical doctors withdifferent specialties (general
surgery,maxillofacial surgery, neurosurgery,ophthalmology, urology,
orthopedics,and traumatology and rehabilitation)were consulted and
asked to note theproportion of RTI patients who would
be hospitalized based on ICD-10 diag-nosis, which was taken from
the hospi-
tal discharge database. In addition, theywere asked to estimate
the proportionof patients who would potentially useambulatory
health services (includingrehabilitation) and the number of
med-ical consultations for hospitalized andnonhospitalized
patients. When spe-cialists did not fill out the questionnaireto
provide missing information, thosefigures (both the proportion that
useservices and the number of consulta-
tions) were assumed to be the same asthose for a similar injury
(from ananatomic and severity perspective).When that option was not
possible, themedian of the number of ambulatorymedical
consultations (or rehabilita-tion) of all the other injuries was
im-puted. The total number of rehabilita-tion consultations
estimated for eachpatient was included in the total num-
ber of ambulatory medical consulta-tions. This survey also made
it possibleto estimate utilization figures for se-verely injured
nonhospitalized patientsand slightly injured non-emergency-room
users (information presented inTable 1). Table 1 shows mean,
median,and mode of hospital stay (obtainedfrom the hospital
discharge database).
By multiplying the median figures forutilization per unitary
cost, direct costswere estimated for Belize. In this sense,all
emergency room medical consulta-
tions, specialized medical consultations,and rehabilitation were
assumed to betertiary outpatient visits to hospital ser-vices. In
the same way, given that 63.6%of hospital discharges received
attentionat the Karl Heusner Memorial Hospital(KHMH) and as
hospital costs do notconsider drugs and diagnostic tests, itwas
decided to use the cost per bed-dayof a tertiary hospital level.
Finally, hospi-tal stay information was obtained fromthe hospital
discharge database for thosewho died. Both survivors and
casualtieshave median lengths of stay of two days.
Indirect cost estimation was calculatedby using the human
capital approach, inwhich the productivity cost was esti-mated as
the future reduction in grossincome due to mortality and
morbidity.In this study, the Belize average incomefor 2007,
documented by the Belize So-cial Security Board, was used for
indirectcost estimates. Indirect costs associatedwith premature
death take as referencethe Belize life expectancy for 2008
docu-
mented by the Pan American Health Or-ganization (PAHO) (76.1
years) (11). Lifeexpectancy was used instead of age at re-tirement
(55 years) to take into accountcountry preferences on how society
val-ues life at different ages, something im-portant to consider
(12). This decisionwas taken as recommended by the BelizeNational
Road Safety Committee. In thissense, elderly people in low- and
mid-
dle-income countries tend to have a verysmall income or none at
all. This situa-tion does not mean that their time has novalue or
should not be valued. This cir-cumstance is similar to the value of
timefor housewives. Although in real termsthey might not receive a
salary, theirwork and activities are highly valued(and needed) by
societies (11). Calcula-tions were made as follows:
Indirect cost of fatal RTI =
Loss of output (death) = (1)
whereS = salary,r = discount rate, andn = number of years of
potential life
lost due to premature death.
For morbidity figures, indirect costs in-cluded the valuation of
postdischarge av-erage time injured spent at home recov-ering from
injuries (72 days). In addition,the value of productivity losses
due totransitory or permanent disability wasestimated by using the
value of disable-ment pensions awarded to the road traf-
fic injured. This information was pro-vided by the Belize Social
Security Board.
Estimating total RTIeconomic costs
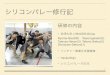
Total estimation of RTI economic costsused a decision tree model
approach aspresented in Figure 1. The decision treeallows one to
disaggregate patients byfatal and nonfatal type of injury. The
lat-
S
r n
n
( )10 +
TABLE 1. Use of health care services by patients with road
traffic injuries, Belize, 2007
Hospitalized Nonhospitalized
Hospital Ambulatory Ambulatorystay medical Rehabilitation
medical Rehabilitation
Variable (days) consultations consultations consultations
consultations
Mean 5 4.87 19.71 4.63 2.11Median 2 3 2 3 2Mode 1 2 0 2 2
-
7/25/2019 Costos SV Belize
4/11
Rev Panam Salud Publica 28(5), 2010 329
FIGURE 1. Decision tree to model economic cost of road traffic
injuries (RTI) in Belize, 2007
Did not receiveattentionatscene
Not used ER
Nonuser
Nonuser
Used ambulatoryservices
Usedrehabilitation
Nonuser
Nonuser
Used ambulatoryservices
Usedrehabilitation
Used ER
Slightly injured
Receivedmedical attention
Not used ER
Nonuser
Nonuser
Used ambulatoryservices
Usedrehabilitation
Nonuser
Nonuser
Used ambulatoryservices
Usedrehabilitation
Used ER
Did not receiveattentionatscene
Did not receiveattentionatscene
Nonhospitalized
Nonuser
Nonuser
Used ambulatoryservices
Usedrehabilitation
Nonuser
Nonuser
Used ambulatoryservices
Usedrehabilitation
Hospitalized
Severely injured
Nonfatal
RTI
Die >30 days
Fatal
Receivedmedical attention
Receivedmedical attention
Nonhospitalized
Nonuser
Nonuser
Used ambulatoryservices
Usedrehabilitation
Nonuser
Nonuser
Used ambulatoryservices
Usedrehabilitation
Hospitalized
Hospitalized
Nonhospitalized
Hospitalized
Nonhospitalized
Prez-Nez et al. Economic impact of road traffic injuries in
Belize Original research
Note:ER: emergency room.
ter category is disaggregated into se-verely injured and
slightly injured. Inaddition, the decision tree follows thenatural
history of disease, starting with
prehospital medical attention at thescene, continuing with
hospital-basedcare (hospitalization versus emergencyroom only),
utilization of ambulatory
health services, and disaggregating am-bulatory services into
rehabilitation ser-vices. Each tree branch has a probabilityof
occurrence and a specific associated
-
7/25/2019 Costos SV Belize
5/11
330 Rev Panam Salud Publica 28(5), 2010
Original research Prez-Nez et al. Economic impact of road
traffic injuries in Belize
cost. In this way, total cost per treebranch corresponds to the
multiplicationof unitary cost per total number of in-
jured estimated for that specific branch.The individual total
cost of RTI for this
study was thus obtained after adding di-rect costs to indirect
costs of those hospi-talized and those who received emer-
gency care only. The economic cost ofRTI in Belize was estimated
in the fol-lowing manner:
(2)
whereTC = total economic cost of RTI,
AECd = average economic cost per RTIdeathf,
AECs = average economic cost of se-
verely injured s,AECsl = average economic cost of
slightly injured sl,D = total number of RTI deaths regis-
tered in 2007,S = estimation of total number of se-
verely injured, andSL = estimation of total number of
slightly injured.
Analysis
A descriptive analysis was performedfor all databases. Central
tendency and
dispersion measures were calculated forthe continuous variable
(mean, median,standard deviation, maximum, and min-imum values) as
well as frequencies andpercentages for the categorical
variablesusing Stata 9.2 (13).
Uncertainty surrounding some of themodels assumptions was
explored witha multiway and probabilistic sensitivityanalysis. The
analysis was performed forvariables such as prevalence and
inci-dence figures (death, hospitalized, at-tended at emergency
room) and for threediscounted rates (0%, 3%, and 5%), al-
though in the text only results using the3% discount rate are
presented. Sensitiv-ity analysis of the number of RTI hospi-talized
considered a literature review tosimulate potential scenarios
consideringthe possibility of hospital underregistra-tion (1421).
This was also the case forslightly injured people. This part of
theanalysis was carried out with software@RISK 5.5 (22). Figures
are presented inUS dollars, using an exchange rate of
US$1.00 = BZ$2.00, which has beenpegged to the US dollar since
1976 (11).
RESULTS
Epidemiology of RTI in Belize
During 2007, 63 people died as a con-
sequence of RTI, of whom 79.4% were
men (Table 2). This figure is equivalentto a total of 61 people
if adjusted byWHOs 30-day definition (total numberof deaths
multiplied by the adjustmentfactor of 0.97). Mean age was 37
years(median = 33) and 68.3% of all injuredwere between 15 and 49
years of age. Itwas not possible to determine the type of
road user most affected, because most
TC Belize AEC D AEC Sdi
n
si
n( )=
+
= =
1 1
+
=AEC SLsli
n
1
TABLE 2. Descriptive analysis of road traffic injury casualties,
Belize, 2007
Variable Frequency %
Individual characteristicsSex
Women 13 20.6Men 50 79.4
Age group (years)014 4 6.31524 13 20.62549 30 47.65074 14
22.2
75 2 3.2Civil statusCommon law 7 11.1Divorced 0 0.0Married 12
19.0Single 43 68.3Unknown 0 0.0Widowed 1 1.6
SchoolingNone 3 4.8Primary 43 68.3Secondary 5 7.9Tertiary 3
4.8Unknown 9 14.3
Activity/occupationWage earner 41 65.1Nonremunerative activity 5
7.9
Unknown 17 27.0Death and medical attention informationPlace of
death
Hospital 32 50.8Road/street 27 42.9Home/farm/workplace 2
3.2Route to hospital 0 0.0Unknown 2 3.2
District of residenceBelize 32 50.8Cayo 8 12.7Corozal 5
7.9Orange Walk 8 12.7Stann Creek 3 4.8Toledo 7 11.1
District of death occurrenceBelize 48 76.2
Cayo 0 0.0Corozal 3 4.8Orange Walk 6 9.5Stann Creek 2 3.2Toledo
4 6.3
Hospital that registered deathBelmopan Hospital 0 0.0Central
Region Belize District 48 76.2Corozal Town Hospital 3 4.8Orange
Walk Hospital 6 9.5Punta Gorda Hospital 4 6.3San Ignacio Town
Hospital 0 0.0Southern Regional Hospital 2 3.2
-
7/25/2019 Costos SV Belize
6/11
Rev Panam Salud Publica 28(5), 2010 331
deaths were coded as other and un-specified. Most deaths took
place in Be-lize district (76.2%) and 50.8% of alldeaths occurred
in a hospital. This valuetranslates to a mortality rate of
20.1deaths per 100 000 population. When an-alyzed with a Poisson
regression model,on average, the relative risk of dying as a
consequence of RTI in Belize decreased7.1% each year during
20012007 (95%confidence interval 3.3% to 10.8%).
During 2007, 338 hospital dischargesdue to RTI were recorded in
all publichospitals in Belize (hospital dischargerate of 117.36
discharges per 100 000population). Of them, 74.9% were men,with a
mean age of 29 years (standarddeviation = 18, median = 26) and
67.5%were between 15 and 49 years of age(Table 3). Most road users
were also clas-sified as other and unspecified. Alarge majority of
hospital discharges
were reported by KHMH, the only ter-tiary level hospital in
Belize. Of all RTIhospitalized, 2.7% died during hospital-ization
(n = 8).
Table 4 presents all emergency ambu-lance services provided by
BERT in Be-lize district in 2007. A total of 222 ambu-lance
services were solicited, although 24of them did not require any
service. Ofthe remainder, 47 (23.7%) were severelyinjured (42.0% of
the total number hospi-talized in Belize district the same
year),73.2% were slightly injured, and 3.0% ofthe injured died.
Most people attended
were men (71.7%) and 74.5% were be-tween 15 and 49 years of age.
Of all in-
jured, 90.4% received treatment andwere transferred to a medical
institution.
No detailed information was availableon patients slightly
injured after a colli-sion. Similarly, no information on emer-gency
room hospital-based medical atten-tion was provided. Using BERT
figures(an estimated 77.5% of the total numberof nonhospitalized
slightly injured in Be-lize district the same year), a total of
565slightly injured was estimated.
Economic cost of RTI
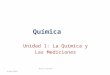
Direct cost. A total of US$163 503 wasestimated for direct costs
during 2007, ofwhich 2.4% was spent on fatalities, 46.7%on severely
injured, and 50.9% on slightlyinjured. Figure 2 shows that most of
thiscost was estimated for prehospital care(36.8%), hospitalization
(21.5%), and am-
bulatory medical consultations (20.3%),while rehabilitation
represented 11.2%.
TABLE 3. Descriptive analysis of hospital discharges due to road
traffic injuries,Belize, 2007
Variable Frequency %
Individual characteristicsSex
Women 85 25.1Men 253 74.9
Age group (years)
014 69 20.41524 86 25.42549 142 42.05074 33 9.8 75 8 2.4
Civil statusCommon law 49 14.5Divorced 0 0.0Married 60
17.8Single 199 58.9Unknown 28 8.3Widowed 2 0.6
SchoolingNone 74 21.9Primary 145 42.9Secondary 53 15.7Tertiary
12 3.6Unknown 54 16.0
Activity/occupationWage earner 128 37.9Nonremunerative activity
119 35.2Unknown 91 26.9
Medical attention and occurrenceAdmittance
Emergency 281 83.1Outpatient 57 16.9
District of residenceBelize 112 33.1Cayo 93 27.5Corozal 35
10.4Orange Walk 20 5.9Stann Creek 44 13.0Toledo 34 10.1
District of dischargeBelize 215 63.6Cayo 53 15.7Corozal 12
3.6Orange Walk 23 6.8Stann Creek 14 4.1Toledo 21 6.2
HospitalBelmopan Hospital 40 11.8 (1.6)a
Corozal Town Hospital 12 3.6 (1.1)a
KHMH Consolidation 215 63.6 (2.5)a
Orange Walk Hospital 23 6.8 (0.9)a
Punta Gorda Hospital 21 6.2 (1.5)a
San Ignacio Town Hospital 13 3.8 (1.0)a
Southern Regional Hospital 14 4.1 (0.5)a
Description of serviceAccident and emergency 1 0.3
General medicine 32 9.5Gynecology 1 0.3In-patient services 64
18.9Pediatric 42 12.4Surgical services 177 52.4
Discharge conditionAlive 302 89.3Dead 8 2.4Self-discharge 9
2.7Transferred 18 5.3Missingvalues 1 0.3
Note:KHMH: Karl Heusner Memorial Hospital.a Numbers in
parentheses indicate road traffic injuries as percent of total.
Prez-Nez et al. Economic impact of road traffic injuries in
Belize Original research
-
7/25/2019 Costos SV Belize
7/11
332 Rev Panam Salud Publica 28(5), 2010
Original research Prez-Nez et al. Economic impact of road
traffic injuries in Belize
From this figure, the potential underesti-mation of
hospitalization costs is evident,as drugs and diagnostics are not
includedin unitary cost estimations used for thisanalysis.
Indirect cost. A total of 2 501 years of po-
tential life were lost in Belize during2007 due to RTI (Table
5). This numbertranslates to a social loss of US$8 116
917attributed to indirect cost due to produc-tivity loss (Table 6).
Table 6 disaggre-gates indirect cost by district for bothmethods
and considers different scenar-ios in terms of discount rates.
Belize dis-trict is where more indirect cost was lost:53.3% of the
total or US$4 328 717. In ad-dition, injured people who were
hospi-
TABLE 4. Emergency ambulance services due to road traffic
injuries, Belize district, 2007
Type of injury
Slight Serious Fatal Total
Variable No. % No. % No. % No. %
SexWomen 41 28.3 8 17.0 0 0.0 49 24.7Men 102 70.3 37 78.7 3 50.0
142 71.7
Missingvalue 2 1.4 2 4.3 3 50.0 7 3.5Age (years)
Mean 29.6 NA 28.4 NA (. . .) (. . .) NA NA014 9 6.2 6 12.8 (. .
.) (. . .) 15 7.81524 45 31.0 12 25.5 (. . .) (. . .) 57 29.72549
66 45.5 20 42.6 (. . .) (. . .) 86 44.85074 12 8.3 3 6.4 (. . .) (.
. .) 15 7.8 75 1 0.7 0 0.0 (. . .) (. . .) 1 0.5Missingvalue 12 8.3
6 12.8 (. . .) (. . .) 18 9.4
DayMonday 10 6.9 3 6.4 1 16.7 14 7.1Tuesday 8 5.5 2 4.3 1 16.7
11 5.6Wednesday 19 13.1 5 10.6 0 0.0 24 12.1Thursday 23 15.9 6 12.8
0 0.0 29 14.6Friday 20 13.8 7 14.9 2 33.3 29 14.6Saturday 32 22.1
17 36.2 2 33.3 51 25.8Sunday 33 22.8 7 14.9 0 0.0 40 20.2
MonthJanuary 6 4.1 4 8.5 1 16.7 11 5.6February 13 9.0 5 10.6 2
33.3 20 10.1March 13 9.0 1 2.1 0 0.0 14 7.1April 7 4.8 7 14.9 0 0.0
14 7.1May 28 19.3 8 17.0 2 33.3 38 19.2June 7 4.8 1 2.1 0 0.0 8
4.0July 24 16.6 5 10.6 0 0.0 29 14.6August 10 6.9 6 12.8 0 0.0 16
8.1September 9 6.2 2 4.3 0 0.0 11 5.6October 9 6.2 4 8.5 0 0.0 13
6.6November 6 4.1 1 2.1 0 0.0 7 3.5December 13 9.0 3 6.4 1 16.7 17
8.6
Type of service providedTreated on site only 8 5.5 0 0.0 0 0.0 8
4.0Treated and transport 135 93.1 44 93.6 0 0.0 179 90.4Air
transportation 1 0.7 0 0.0 0 0.0 1 0.5
No treatment 1 0.7 3 6.4 6 100.0 10 5.1Total 145 73.2 47 23.7 6
3.0 198 89
No service provided NA NA NA NA NA NA 24 11Grand total NA NA NA
NA NA NA 222 100
Source:Belize Emergency Response Team administrative
records.Note:NA: not applicable, (. . .): information not
available.
FIGURE 2. Health system costs estimated for Belize, by type of
service, 2007
Prehospital care 36.8%
Rehabilitation 11.2%
Hospitalization21.5%
Ambulatory medicalconsultations20.3%
Emergency roomservices10.3%
Note:Cost of hospitalization does not include drugs and
diagnostic tests, which could represent a largeproportion of total
hospitalization costs in this type of patient.
-
7/25/2019 Costos SV Belize
8/11
Rev Panam Salud Publica 28(5), 2010 333
talized stayed an average of 5 days in thehospital. This value
represents an aver-age of US$76 of indirect cost per RTI hos-
pitalization and a total of US$25 456 lostfor this cause.
Total economic cost of RTI. Aggregatedfigures are presented in
Table 7. As indi-cated, the base model estimated a totaleconomic
cost of US$9 453 615 due to RTIduring 2007. The great majority of
thecost is due to fatal injuries, specifically in-direct costs
attributed to prematuredeath. When the distribution of total
eco-nomic cost estimated in all 10 000 itera-tions of the simulated
model was ana-lyzed, 90.0% of all estimates fell between
US$10 005 971 and US$12 273 030 (aver-age of US$11 062 544 using
a discountrate of 3%). This estimation represents0.9% of the Belize
GDP during 2007 and2.8% of the total government budget forthe same
year (Table 8). Table 9 shows the
base model results compared with the
sensitivity analysis figures (simulation).According to the
simulation, during 2007the total nonfatal RTI rate was 1 468.7
per
100 000 population. Finally, informationprovided by the Social
Security Boardshowed that at least two people were dis-abled in
2007 as a consequence of RTI (0.7per 100 000 population).
DISCUSSION
The usefulness of cost-of-illness stud-ies for health systems
lies in justifyingthe design and implementation of speci-fied
intervention programs and makingevident the economic loss that the
illnesspresents, with its specific and current
mortality and morbidity rates. In thesame way, these studies
help the re-source allocation process by contributingto
determination of the importance ofeach illness from an economic
perspec-tive and highlighting medical care andspecific research
needs. In addition, they
provide a basis for planning and estab-lishing political and
public health initia-tives for prevention and control and
aneconomic-referenced framework for thenext evaluation of programs
and imple-mented interventions (23).
Information generated in this studywill allow all districts and
national au-
thorities in Belize to have valuable infor-mation for decision
making. In general,this study will aid decision making, jus-tifying
the need for implementing ameaningful road traffic safety
program.It also allows for understanding the realmagnitude of a
problem that so farseems reflected only in causes of mor-tality and
social security payments.Therefore, the economic assessment of
aproblem of this extent will allow visual-ization of the potential
resource savingsthat can be applied to other social andhealth
problems. In this sense, the results
make evident the large problem that RTIcause to the health
system in Belize andsociety as a whole. From the results ofeconomic
cost estimations, there is anurgent need to prevent RTI through
astrategic and multisectoral approachthat focuses on the principal
problemsdetected.
This study faced methodologic chal-lenges due to the lack of
specific infor-mation, such as costs and number ofnonhospitalized
injured people. Al-though secondary cost information usedmight
underestimate the real problem, it
gives a general idea of the magnitude ofthe problem in economic
terms. Futureefforts should consider the use of pri-mary data to
evaluate to what extentthese estimates change. In the same
way,problems in current information systemswere evident. That was
the case in the
TABLE 5. Deaths and years of potential life lost by district,
Belize, 2007
Characteristic District of residence Number
Total deaths Belize (district) 32Cayo 8Corozal 5Orange Walk
8Stann Creek 3Toledo 7
Belize (country) 63Years of potential life losta Belize
(district) 1 380
Cayo 371Corozal 214Orange Walk 238Stann Creek 105Toledo
194Belize (country) 2 501b
a PAHO life expectancy in Belize for 2008age at death for people
with less than life expectancy.b May not sum to total due to
rounding.
TABLE 6. Indirect costs of premature death (US dollars) by
district, Belize, 2007
Indirect cost District of residence Discount rate 0% Discount
rate 3% Discount rate 5%
Minimum wage Belize (district) 4 844 151 2 637 812 1 828 566Cayo
1 301 508 704 967 487 627
Corozal 749 385 403 516 281 063Orange Walk 834 678 570 191 425
693Stann Creek 369 603 231 689 168 315Toledo 679 536 398 073 281
701Belize (country) 8 778 861 4 946 247 3 472 963
Average wage Belize (district) 7 949 376 4 328 717 3 178 414Cayo
2 135 808 1 156 869 846 064Corozal 1 229 760 662 179 489 891Orange
Walk 1 369 728 935 697 744 428Stann Creek 606 528 380 208 293
404Toledo 1 115 136 653 247 496 671Belize (country) 14 406 336 8
116 917 6 048 871
Note:Exchange rate is US$1.00 = BZ$2.00.
Prez-Nez et al. Economic impact of road traffic injuries in
Belize Original research
-
7/25/2019 Costos SV Belize
9/11
334 Rev Panam Salud Publica 28(5), 2010
Original research Prez-Nez et al. Economic impact of road
traffic injuries in Belize
codification of external causes of death,as most deaths and
hospitalizations werecoded as other and unspecified. Thiscoding
problem did not allow estimationof cost per type of road user or
analysisof the medical attention characteristics ofdifferent road
users. Improved codingefforts should be attempted in the future
in order to better appreciate the type ofproblem Belize faces in
terms of roadsafety. This information would be in-valuable for
policy making, as most pre-vention strategies differ depending
onthe type of road user who is most af-fected. In addition, no
information wasavailable on the number of emergencyroom
hospital-based services providedas well as the number of ambulatory
ser-vices provided (including rehabilita-tion). In this sense, it
is important to con-sider that better information systemswould
translate to better estimates of the
economic cost of this important publichealth problem.
The methodology used to estimate in-direct costs could
overestimate actualfigures because it gives more weight todeaths
that occurred at an early stage oflife, according to some
perspectives suchas the investmentproducerconsumermodel
perspective. This conceptualframework, originally proposed
byGardner and Sanborn (24), argues thatduring the investment period
(less than18 years of age), people only receivefrom society
(negative value) while dur-
TABLE 7. Economic impact of road traffic injuries by severity
and cost type,Belize, 2007
Direct cost Indirect costa
Severity (US$) (US$) Total (US$)
Fatal 3 886 8 795 959 8 799 845NonfatalSevere 76 400 488 083 564
483Slight 83 218 6 070 89 288
Total 163 503 9 290 112 9 453 615
a Indirect costs with discount rate of 3% under base model
assumptions.
TABLE 8. Economic cost of road traffic injuries as percentage of
gross domesticproduct and government budget, Belize, 2007
Characteristic Amount
Total GDP (US$) 1 267 000 000Total government budget (US$) 396
657 177Total MOH budget (US$) 43 213 108MOH budget as percentage of
government budget 10.9MOH budget as percentage of GDP 3.4Total cost
of RTI (US$)
0% discount rate 17 995 4153% discount rate 11 062 5445%
discount rate 8 599 470
Cost of RTI as percentage of GDP0% discount rate 1.43% discount
rate 0.95% discount rate 0.7
Cost of RTI as percentage of government budget0% discount rate
4.53% discount rate 2.85% discount rate 2.2
Cost of RTI as percentage of MOH budget0% discount rate 41.63%
discount rate 25.65% discount rate 19.9
Note:US$1.00 = BZ$2.00. GDP: gross domestic product, MOH:
Ministry of Health, RTI: road traffic injuries.
TABLE 9. Economic cost of road traffic injuries estimated for
Belize, 2007
Total cost (USdollars)
Basea Average of simulationa with Total injured
Injury DR 0% DR 3% DR 5% DR 0% DR 3% DR 5% Base Simulation
FatalHospitalized 1 988 122 1 153 106 856 446 2 160 922 1 253
330 930 885 8Not hospitalized 13 190 201 7 646 739 5 677 287 14 336
643 8 311 364 6 170 735 53Total 15 178 323 8 799 845 6 533 733 16
497 565 9 564 694 7 101 620 61 66
NonfatalDied > 30 days 3 970 3 970 3 970 4 320 4 320 4 320
2Hospitalized
Hospitalization 517 685 517 685 812 772 812 772 812 772 338 338
531Ambulatory users 16 003 16 003 25 125 25 125 25 125 261
261Rehabilitation users 8 672 8 672 13 615 13 615 13 615 212
212
ER users 17 161 17 161 117 918 117 918 117 918 471 471 3 239ER
servicesAmbulatory users 14 506 14 506 99 674 99 674 99 674 237
237Rehabilitation users 8 255 8 255 56 719 56 719 56 719 202
202
Total (hospital + ER) 642 908 642 908 1 446 170 1 446 170 1 446
170 854Nonusers of health services NA NA NA NA NA 83
Total (fatal + nonfatal) 15 832 094 9 453 615 7 187 504 17 995
415 11 062 544 8 599 470 998 4 531
Note:Both models (base and simulation) use average income
reported by Social Security Board to estimate indirect costs
(BZ$960, US$480 per month). DR: discount rate, ER: emergencyroom,
NA: not applicable.a Simulation figures consist on average of the
10 000 iterations for different distributions of uncertain
parameters (carried out with @RISK software).
-
7/25/2019 Costos SV Belize
10/11
Rev Panam Salud Publica 28(5), 2010 335
ing the production period they give backto society (positive
value). However, thisframework should also take into accountcountry
preferences on how society val-ues life at different age periods.
In addi-tion, some authors believe there are costshouseholds would
have incurred with-out suffering RTI that could be evaluated
only by using counterfactuals (controlgroup scenario), which was
not consid-ered in this study (25).
WHO estimates that RTI cost repre-sents 1.0% of the GDP in
low-incomecountries, while in medium- and high-income countries the
cost can reach 1.5%and 2.0% of GDP, respectively (19). Thisstudy
documents that the total economiccost of RTI in Belize accounts for
0.9% ofthe GDP in the study year. In this regard,Mohan argued that
the method usedmay influence the final estimation (20).When he
analyzed the differences be-
tween low- and high-income countries,he found that estimates in
high-incomecountries tended to be more detailed andcomprehensive,
since they included will-ingness to pay, quality-adjusted
lifeyears, and healthy life years (20). Ac-cording to this author,
if the willingness-to-pay method had been used in India,the total
cost of RTI would have in-creased from 0.8% to 2.0% of GDP. Healso
highlighted some problems, such aslack of access to health services
and tech-nology, which, together with few workopportunities for
people with disabili-
ties, contributed to underestimation ofthe RTI cost in low- and
medium-incomecountries. Epidemiologic informationfrom countries
with better registersshows how estimates from differentcountries
would also increase to 2.0% ofGDP (20). That might be the case in
theBelize estimates.
CONCLUSIONS
According to this study, it was possi-ble to identify the high
cost that RTI rep-resents to Belize society in general. Dur-
ing 2007, the economic cost of RTI in Be-lize was estimated to
be US$11 062 544(90% confidence interval US$10 005 971to US$12 273
030), from which the greatmajority corresponds to the indirect
costof premature death. This value repre-sents almost 1.0% of the
total GDP of Be-lize for the same year and is equivalent
to 2.8% of the total government and25.6% of the Ministry of
Health budgets.These figures make it possible to visual-ize the
potential financial resources thatcan be used for RTI prevention
and othersocial and health conditions if currentepidemiologic
figures decrease. Thestudy identified that the main victimsare men
and youth; however, there is agap of information about the type
ofroad user injured or dead. Current fatal,nonfatal, and disability
rate figures (20.1,1 468.7, and 0.7 per 100 000
population,respectively) highlight the need to im-
plement effective preventive strategiesin the short term to
alleviate the current
burden of RTI in the country. Informa-tion generated in this
study therefore al-lows for greater understanding of thereal
magnitude of RTI, including eco-nomic impact.
Recommendations
The considerable economic costs ofRTI and deaths in Belize
require specialattention to apply cost-effective strate-gies and
law enforcement in order to
provide road safety for all road users.Improving the health
information sys-tem to capture important data on RTI isessential.
In this regard, unification datafrom different sources (health,
police,and other) are essential to have a betteridea of the
magnitude of the problem.Belize should work on a single RTI
data-
base common for the entire country,with the type of road user
coded prop-erly. Epidemiologic information such asthe number of
injured people attendedin emergency rooms and
hospital-basedfacilities as well as ambulatory follow-
up patients as a result of RTI should beavailable and
quantified. This informa-tion will allow for greater
in-depthanalysis of RTI in the country.
Acknowledgments. Technical and fi-nancial support was provided
by the
WHO/PAHO Country Office. This eco-nomic impact study was
commissioned
by the Belize National Road Safety Com-mittee in support of
activities outlinedin the National Strategic Plan to ReduceRoad
Traffic Injuries in Belize. Thepreparation of this study would not
have
been possible without the collaborationand support of numerous
agencies andindividuals. Special thanks to PeterAllen, chief
executive officer of the Min-istry of Health; Michael Pitts,
director ofhealth services; and the Office of the Di-rector of
Health Services for facilitating
and providing support throughout thedata collection process and
finalizationof the study. Special thanks to the PAHOCountry Office
for technical and ad-ministrative support in making thisstudy a
reality. Thanks also go to themembers of the National Road
SafetyCommittee. The following people wereexceptional in
facilitating the processand contributed significantly to the
col-lection of data to support the research:Yvette Burks (BERT),
Jorge Polanco(Ministry of Health), Aisha Andrewin(Ministry of
Health), assistant superin-
tendent of police Francis Williams (Traf-fic Department,
Police), assistant su-perintendent of police Simeon Avila(Traffic
Department, Police), deputycommissioner of police James Magde-lano
(Traffic Department, Police), Vladi-mir Romero (Traffic Department,
Po-lice), and Bruce Flowers (Belize SocialSecurity Board). In
addition, the authorsacknowledge the time of personnel ofKHMH from
the Records Departmentand the medical doctors who respondedto the
health provider survey in order toestimate ambulatory care.
1. Ministry of Health. Belize basic indicators 2005,1st ed.
Belmopan, Belize: MOH; 2006. P. 12.
2. Organizacin Panamericana de la Salud. In-forme sobre el
estado de la seguridad vial enla regin de las Amricas. Washington,
DC:OPS; 2009.
3. Hijar M, Vazquez-Vela E, Arreola-Risa C.Pedestrian traffic
injuries in Mexico: a country
update. Inj Control Saf Promot. 2003;10(12):3743.
4. Hjar-Medina M, Vazquez-Vela E. Foro na-cional sobre
accidentes de trnsito en Mxico.Enfrentando los retos a travs de una
visinintersectorial, 1st ed. Cuernavaca, Morelos,Mxico: Instituto
Nacional de Salud Pblica;2003.
5. Naumann RB, Dellinger AM, Zaloshnja E,Lawrence BA, Miller TR.
Incidence and to-tal lifetime costs of motor vehicle-relatedfatal
and nonfatal injury by road user type,United States, 2005. Traffic
Inj Prev. 2010;11(4):35360.
6. Impactos sociais e econmicos dos accidentesde trnsito nas
rodovias brasileiras-relatrio
REFERENCES
Prez-Nez et al. Economic impact of road traffic injuries in
Belize Original research
-
7/25/2019 Costos SV Belize
11/11
336 Rev Panam Salud Publica 28(5), 2010
Original research Prez-Nez et al. Economic impact of road
traffic injuries in Belize
executivo. Brasilia: IPEA/DENATRAN/ANTP;2006.
7. Organizacin Panamericana de la Salud.Clasificacin estadstica
internacional de en-fermedades y problemas relacionados con
lasalud, 10th ed. Washington, DC: OPS; 1995.
8. Transport Research Laboratory. Guidelinesfor estimating the
cost of road crashes in de-veloping countries. Project R7780.
London:Department for International Development;
2003.9. World Health Organization. Global status re-
port on road safety: time for action. Geneva:WHO; 2009.
10. Adam T, Evans DB, Murray CJ. Econometricestimation of
country-specific hospital costs.Cost Eff Resour Alloc.
2003;1(1):3.
11. Organizacin Panamericana de la Salud. In-formacin de la
salud y anlisis: situacin desalud en las Amricas: indicadores
bsicos2008. Washington, DC: OPS; 2008.
12. Organizacin Panamericana de la Salud. Tc-nicas para la
medicin del impacto de la mor-
talidad: aos potenciales de vida perdidos.Bol Epidemiol.
2003;24(2):14.
13. Stata Corporation. Stata 9.2. College Station,TX: Stata
Press; 2003.
14. Albert T, Eden C. The economic burden of un-intentional
injury in Alberta. Edmonton, Al-
berta, Canada: Alberta Centre for Injury Con-trol and Research;
2002.
15. Al-Masaeid HR, Al-Mashakbeh AA, QudahAM. Economic costs of
traffic accidents in Jor-
dan. Accid Anal Prev. 1999;31(4):34757.16. National Institute of
Mental Health and
Neuro Sciences. Road traffic injury (factsheet). Bengaluru,
India: National Institute ofMental Health and Neuro Sciences;
2008.
17. Institute for Road Safety Research. Road crashcost.
Leidschendam, Netherlands: Institutefor Road Safety Research;
2007.
18. Ministry of Transport. The social cost of roadcrashes and
injuries. Wellington, New Zea-land: Ministry of Transport;
2006.
19. Peden MM. World report on road traffic in-jury prevention.
Geneva: WHO; 2004.
20. Mohan D. Social cost of road traffic crashes inIndia. New
Delhi: Indian Institute of Technol-ogy; 2002.
21. National Safety Council. Injury facts. Itasca,IL: National
Safety Council; 2007.
22. Palisade C. @RISK, version 5.0. Ithaca, NY:Palisade;
2009.
23. Rice DP. Cost of illness studies: what is goodabout them?
Inj Prev. 2000;6(3):1779.
24. Gardner JW, Sanborn JS. Years of potential
life lost (YPLL)what does it measure?Epidemiology.
1990;1(4):3229.
25. World Health Organization. WHO guide toidentifying the
economic consequences of dis-ease and injury, 1st ed. Geneva: WHO;
2009.
Manuscript received on 12 July 2010. Revised version ac-cepted
for publication on 19 October 2010.
Objetivo. Calcular el costo econmico de los traumatismos por
accidentes de trn-sito registrados en Belice durante el ao
2007.Mtodos. Se realiz un estudio transversal a partir de datos
secundarios sobre loscostos, tanto desde la perspectiva social como
desde la del sistema de salud. La infor-macin epidemiolgica se
obtuvo a partir de la base de datos de mortalidad, la basede datos
nacional de egresos hospitalarios y los expedientes administrativos
de la po-lica y el Ministerio de Salud. Se llev a cabo una encuesta
a los prestadores de servi-cios de salud para calcular las cifras
correspondientes a la atencin ambulatoria pos-terior al egreso.
Para calcular los costos directos, se utiliz la base de datos
delproyecto WHO-CHOICE (eleccin de intervenciones eficaces en
funcin de los costos)de la Organizacin Mundial de la Salud. El
equipo de respuesta a las urgencias m-dicas de Belice aport los
datos sobre los costos prehospitalarios. Despus de calcularlos aos
de vida potencial perdidos tomando como parmetro la esperanza de
vidade Belice correspondiente al ao 2008 y empleando el mtodo
propuesto por la Orga-nizacin Panamericana de la Salud, se calcul
el costo indirecto asociado a la muerteprematura desde el enfoque
del capital humano. Se utiliz un modelo de rbol de de-cisiones para
calcular el costo econmico total derivado de los traumatismos
causadospor el trnsito y se hizo un anlisis de sensibilidad
multivariado y probabilstico paraincorporar los parmetros de
incertidumbre en las estimaciones.Resultados. En Belice, durante el
ao 2007, los traumatismos causados por el trn-sito provocaron la
muerte de 61 personas, la hospitalizacin de 338 y, segn se
cal-cula, lesiones menores a 565. Se perdieron 2 501 aos de vida
potencial a causa de lasmuertes prematuras, lo que se tradujo en un
costo econmico total de US$11 062 544.Esta cifra representa 0,9%
del producto interno bruto de Belice. Se calcul que el costodirecto
fue de US$ 163 503, del cual 2,4% fue ocasionado por las muertes,
46,7% por
la atencin de las personas que sufrieron traumatismos graves y
50,9% por la atencinde quienes presentaron lesiones
menores.Conclusiones. El costo econmico calculado en este estudio
pone de manifiesto lanecesidad de prevenir los traumatismos
causados por el trnsito adoptando un m-todo estratgico y
multisectorial que se centre en abordar los principales
problemasdetectados.
Accidentes de trnsito; costos de la atencin en salud; costos y
anlisis de costo; Belice.
RESUMEN
Repercusiones econmicasde los traumatismos mortalesy no mortales
por accidentesde trnsito en Belice en 2007
Palabras clave