Embed Size (px)
Citation preview

22/01/2010
1
DISFUNCIÓN DISFUNCIÓN ARTICULACIÓN ARTICULACIÓN
TÉMPOROTÉMPORO--MANDIBULAR MANDIBULAR (DTM)(DTM)
HOSPITAL GENERAL UNIVERSITARIO ALICANTE:HOSPITAL GENERAL UNIVERSITARIO ALICANTE:
Fco Javier MondéjarFco Javier MondéjarSandra MuletSandra MuletCarmen RodríguezCarmen RodríguezDiego GómezDiego Gómez
INTRODUCCIÓNINTRODUCCIÓN�� 2020--28 % población (Solo 20% buscan tratamiento)28 % población (Solo 20% buscan tratamiento)
�� Mujeres (15Mujeres (15--40 años)40 años)
�� ClínicaClínica�� DolorDolor�� “Clicks” mandibulares“Clicks” mandibulares�� Limitación apertura mandibular Limitación apertura mandibular �� CefaleasCefaleas
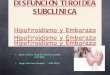
ANATOMÍAANATOMÍA
Disco
Complejo disco-condilar
Fosa glenoidea-
complejo d-cSuperficie articular
superiorSuperficie articular
inferior
Bell’s Orofacial PainsBell’s Orofacial Pains. Jeffrey P.Okeson, DMD. Quintessence Publishing Co, Inc. Carol Stream, Illinois.1999. Jeffrey P.Okeson, DMD. Quintessence Publishing Co, Inc. Carol Stream, Illinois.1999
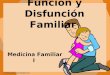
disco
Lig.discal col
medialLig. discal col
lateral
Reborde posterior Z. intermediaReborde anterior
Cóndilo mandibular

22/01/2010
2
Lámina retrodiscal
superior
Tejidos
retrodiscales
Lámina retrodiscal
inferior
Lig. Capsular ant
M. Pterigoideo ext sup
M Pterigoideo ext inf.
Lámina retrodiscal
superior
rotación
traslación
APERTURA BUCAL
DOLOR MASTICATORIODOLOR MASTICATORIO
1) ATM1) ATM
2) DOLORES MIOFASCIALES2) DOLORES MIOFASCIALES
1)1) ATMATMA) Ligamentos discalesA) Ligamentos discalesB) Tejido retrodiscalB) Tejido retrodiscalC) Cápsula articular C) Cápsula articular
D) Artralgia/Artrosis/ArtritisD) Artralgia/Artrosis/Artritis
Bell’s Orofacial PainsBell’s Orofacial Pains. Jeffrey P.Okeson, DMD. Quintessence Publishing Co, . Jeffrey P.Okeson, DMD. Quintessence Publishing Co, Inc. Carol Stream, Inc. Carol Stream, Illinois.1999Illinois.1999
A) A) LIGAMENTOS DISCALESLIGAMENTOS DISCALES
PATOGENIAPATOGENIA�� Grosor reborde posterior disco Grosor reborde posterior disco SE ADELGAZASE ADELGAZA::
�� Disco más anteroDisco más antero--medial medial �� Cóndilo en reborde posterior. Cóndilo en reborde posterior.
Trastornos internos discoTrastornos internos disco//Interferencia del discoInterferencia del disco
Elonga ligamentos/
lámina retrodiscal inferior
Cóndilo
Disco

22/01/2010
3
�� Ligamentos elongadosLigamentos elongados
�� no sensan variaciones propioceptivas (movimiento, no sensan variaciones propioceptivas (movimiento, tracción...)tracción...)
�� disminución dolor podría indicar empeoramientodisminución dolor podría indicar empeoramiento
No dolor
Disco Disco LIGERAMENTE REPLEGADOLIGERAMENTE REPLEGADO sobre el cóndilosobre el cóndilo
movimiento brusco + “movimiento brusco + “click apertura”click apertura”
Pterigoideo externo sup. tira del disco hacia delantePterigoideo externo sup. tira del disco hacia delante
““Click recolocación Click recolocación -- recíprocorecíproco” Estadíos más avanzados” Estadíos más avanzados
Apertura bucal
Cierre bucal
Disco replegado
Click
�� DISLOCACION FUNCIONAL DEL DISCODISLOCACION FUNCIONAL DEL DISCO::
�� MAYOR ADELGAZAMIENTOMAYOR ADELGAZAMIENTO REBORDE POSTERIOR DISCOREBORDE POSTERIOR DISCO
�� Disco completamente antDisco completamente ant--medial medial
�� Traslación /articulación bloqueada 25Traslación /articulación bloqueada 25--30 mm (NR 40)30 mm (NR 40)�� Línea media mandibular: hacia lado afecto (abrir mucho la boca)Línea media mandibular: hacia lado afecto (abrir mucho la boca)
Mayor elongación: lig discales
láminas retrodiscales.
�� DISLOCACION FUNCIONAL DISLOCACION FUNCIONAL CONCON REDUCCIONREDUCCION�� Bloqueo ocasionalBloqueo ocasional�� Resuelve paciente: movilizaciones laterales/abriendo mucho la Resuelve paciente: movilizaciones laterales/abriendo mucho la bocaboca
�� SINSIN REDUCCIÓNREDUCCIÓN�� No recoloca disco No recoloca disco �� Si continúa: cóndilo sobre tejidos retrodiscales :Si continúa: cóndilo sobre tejidos retrodiscales :
�� InflamaciónInflamación�� DolorDolor�� DegeneraciónDegeneración

22/01/2010
4
ETIOLOGIAETIOLOGIA
MACROTRAUMATISMOMACROTRAUMATISMO
�� Mandíbula abiertaMandíbula abierta (caída, tráfico, puñetazo)(caída, tráfico, puñetazo)�� Desplazamiento súbito cóndilo dentro de la fosaDesplazamiento súbito cóndilo dentro de la fosa
�� Iatrógeno Iatrógeno �� IOT (sedados/reducción tono muscular)IOT (sedados/reducción tono muscular)�� Extracciones 3º molarExtracciones 3º molar�� Ttos odontológicos largosTtos odontológicos largos
�� Apertura mandibular muy marcada Apertura mandibular muy marcada �� bostezobostezo
�� Mandíbula cerradaMandíbula cerrada
�� Menor lesiónMenor lesión
�� Oposición desplazamiento articularOposición desplazamiento articular
�� Deportistas/férulas bucales de protección blandas Deportistas/férulas bucales de protección blandas (reducen nº de lesiones).(reducen nº de lesiones).
MICROTRAUMATISMOMICROTRAUMATISMO
1.1. BruxismoBruxismo�� Activación contínua Pterigoideo externo superiorActivación contínua Pterigoideo externo superior
2.2. MasticaciónMasticación�� Múltiples movimientos de traslación/rotación.Múltiples movimientos de traslación/rotación.
elongarían los ligamentos.elongarían los ligamentos.
�� Características dolor ligamentosoCaracterísticas dolor ligamentoso
�� Abuso biomecánicoAbuso biomecánico
�� Intermitente/morder fuerte (pterigoideo ext sup)Intermitente/morder fuerte (pterigoideo ext sup)
�� Generalmente solo disconfort con movimientos mandibularesGeneralmente solo disconfort con movimientos mandibulares
Dolor retrodiscalDolor retrodiscal�� Tejidos retrodiscales Tejidos retrodiscales –– presión condilarpresión condilar
�� Dolor e Inflamación importante (RETRODISCITIS Dolor e Inflamación importante (RETRODISCITIS AGUDA)AGUDA)
Maloclusión aguda en reposoMaloclusión aguda en reposoDisminuye Disminuye ------ separadorseparadorAumenta Aumenta ------ desviaciones homolaterales desviaciones homolaterales
posición máxima intercuspidación posición máxima intercuspidación
Dolor capsularDolor capsular
�� Maloclusión si aumento líquido sinovial (Fluctuación ATM) Maloclusión si aumento líquido sinovial (Fluctuación ATM)
�� No disminuye con férulaNo disminuye con férula�� No aumenta en posición de máxima intercuspidación.No aumenta en posición de máxima intercuspidación.

22/01/2010
5
Dolor artríticoDolor artrítico
�� Artritis traumática / reumática:Artritis traumática / reumática:
�� Maloclusion aguda lado afectoMaloclusion aguda lado afecto
�� Aumenta: presión oclusal ( masticación )Aumenta: presión oclusal ( masticación )�� Mejora con férula lado afectoMejora con férula lado afecto
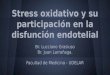
EXPLORACIONES EXPLORACIONES COMPLEMENTARIASCOMPLEMENTARIAS
�� RxRx: ortopantomografía: ortopantomografía
�� ECOGRAFIAECOGRAFIA: : exploración dinámicaexploración dinámica
�� TACTAC / / TAC helicoidalTAC helicoidal / / TAC luz cónicaTAC luz cónica (Menor radiación, (Menor radiación, menor coste)menor coste)
�� RMNRMN (más útil si trastornos internos disco)(más útil si trastornos internos disco)�� Disco, ligamentos, músculos.Disco, ligamentos, músculos.
�� ArtroscopiaArtroscopia
ORTOPANTOMOGRAFIA TAC HELICOIDAL
RMN
2) 2) DOLOR MIOFASCIALDOLOR MIOFASCIAL
�� MASETEROMASETERO�� TEMPORALTEMPORAL�� PTERIGOIDEO INTERNO y EXTERNOPTERIGOIDEO INTERNO y EXTERNO�� DIGASTRICODIGASTRICO�� ECMECM
Travel y Simons.Travel y Simons. Dolor y disfunción miofascialDolor y disfunción miofascial. El manual de los puntos gatillo. . El manual de los puntos gatillo.
Editorial médica panamericana. 2ª edición. 2002.Editorial médica panamericana. 2ª edición. 2002.

22/01/2010
6
MaseteroMasetero: porción profunda: porción profunda
�� Dolor referidoDolor referido: : oído y región oído y región ATMATM
�� Importante restricción Importante restricción apertura mandibular (apertura mandibular (-- 40 mm) 40 mm) Tinnitus unilateralTinnitus unilateral
�� PG asociados: Temporal y PG asociados: Temporal y Pterigoideo medial Pterigoideo medial homolaterales/ Masetero homolaterales/ Masetero contralateral contralateral
�� A menudo son puntos satelites A menudo son puntos satelites ECMECM
TemporalTemporal
�� Dolor referido: Región Dolor referido: Región temporal, ceja, dientes temporal, ceja, dientes superiores. Maxilar superior y superiores. Maxilar superior y ATMATM
�� Apertura normal mandibular Apertura normal mandibular pero incoordinación pero incoordinación apertura/cierre apertura/cierre
�� PG pueden ser puntos PG pueden ser puntos satelites: ECM, trapecio.satelites: ECM, trapecio.
Pterigoideo medialPterigoideo medial
�� Dolor debajo y detrás ATM y Dolor debajo y detrás ATM y dentro del oídodentro del oído ..Dolor Dolor garganta y dificultad para garganta y dificultad para tragar. tragar.
�� Apertura mandibular Apertura mandibular dolorosa/moderadamente dolorosa/moderadamente restringidarestringida
�� Desviación trayectoria incisal Desviación trayectoria incisal lado opuesto durante apertura lado opuesto durante apertura máximamáxima
�� Generalmente asociado a PG Generalmente asociado a PG Pterigoideo lateralPterigoideo lateral
Pterigoideo lateralPterigoideo lateral
�� El más implicado trastornos El más implicado trastornos ATM.ATM.
�� Dolor referido maxilar superior, Dolor referido maxilar superior, incluyendo zona ATM.incluyendo zona ATM.
�� Restricción apertura Restricción apertura mandibularmandibular--trayectoria incisal trayectoria incisal distorsionadadistorsionada--alteración alteración oclusiónoclusión
�� TinnitusTinnitus
DigástricoDigástrico�� Dolor referido a parte superior Dolor referido a parte superior ECM, pero tb a oído.ECM, pero tb a oído.
�� PG consecuencia PG PG consecuencia PG antagonistas: masetero y otros antagonistas: masetero y otros elevadores.elevadores.
ECMECM
División clavicular: División clavicular:
cefalea frontal y dolor oídocefalea frontal y dolor oído
DIAGNOSTICODIAGNOSTICODIFERENCIALDIFERENCIAL
Artralgia origen no masticatorioArtralgia origen no masticatorioHiperuricemias/AR.Hiperuricemias/AR.Inflamación periarticular (Otitis media)Inflamación periarticular (Otitis media)
Otros dolores referidosOtros dolores referidosAfectación trigémino / glándulas salivalesAfectación trigémino / glándulas salivales

22/01/2010
7
Sd EagleSd Eagle
�� Elongación apófisis Elongación apófisis estiloides o calcificación estiloides o calcificación del lig estilohioideodel lig estilohioideo
�� Irritación garganta Irritación garganta persistente con disfagiapersistente con disfagia
�� Dolor referido región Dolor referido región auricular y oftálmicaauricular y oftálmica
�� Limitación movimientos del Limitación movimientos del cuello. cuello.
�� Sincope giros cefálicos Sincope giros cefálicos (compromiso flujo arteria (compromiso flujo arteria carotida por presión)carotida por presión)
Neuralgia glosofaringeaNeuralgia glosofaringea
�� Estimulación receptores mucosa faríngeaEstimulación receptores mucosa faríngea�� Fonación Fonación �� Movimientos mandibulares y de la garganta (masticar/deglutir)Movimientos mandibulares y de la garganta (masticar/deglutir)
�� Dolor retromandibular e infraauricular.Dolor retromandibular e infraauricular.
�� Anestesia tópica mucosa faringea es dx.Anestesia tópica mucosa faringea es dx.
TRATAMIENTOTRATAMIENTO�� EDUCACION DEL PACIENTEEDUCACION DEL PACIENTE
�� TTO FISICOTTO FISICO
�� TTO FARMACOLOGICOTTO FARMACOLOGICO
�� TTO CON FERULA OCLUSAL.TTO CON FERULA OCLUSAL.
Educación del pacienteEducación del paciente
�� Reducir carga ATM:Reducir carga ATM:
�� Alimentos más blandos, masticar más lento, mordiscos más Alimentos más blandos, masticar más lento, mordiscos más pequeños, evitar chicles.pequeños, evitar chicles.
�� Realizar movimientos no dolorosos / no “click”.Realizar movimientos no dolorosos / no “click”.
�� Informar:Informar:
�� Trastorno autolimitado pero prolongadoTrastorno autolimitado pero prolongado�� Animar apertura bucal cuando mejore sintomáticamenteAnimar apertura bucal cuando mejore sintomáticamente
Tratamiento FísicoTratamiento Físico
�� PARA MEJORAR EL DOLORPARA MEJORAR EL DOLOR::�� Calor superficialCalor superficial ( vascularización/repara) ( vascularización/repara) 1010--15’15’
�� Toalla húmeda y caliente que envuelva botella agua Toalla húmeda y caliente que envuelva botella agua caliente/almohada eléctricacaliente/almohada eléctrica
�� FríoFrío (analgésico(analgésico--antiinflamatorio) antiinflamatorio) 55--7’7’�� Movimientos circulares sin presión con hieloMovimientos circulares sin presión con hielo�� Aerosol refrigerante (cloruro de etilo/ fluorometano)Aerosol refrigerante (cloruro de etilo/ fluorometano)
�� IONOFORESISIONOFORESIS--FONOFORESISFONOFORESIS
�� LASERLASER (Acelera la síntesis de colágeno / Aumenta la (Acelera la síntesis de colágeno / Aumenta la vascularización tejidos / Analgésico)vascularización tejidos / Analgésico)
1).- Marega S Medlicott, Susan R Harris: A systematic reviewed of the effectiveness of exercise, A systematic reviewed of the effectiveness of exercise, manual therapy, electrotherapy, relaxation training, and biofeedback in the managment of manual therapy, electrotherapy, relaxation training, and biofeedback in the managment of temporomandibular disordertemporomandibular disorder. Physical Therapy. 86,7. July 2006. Physical Therapy. 86,7. July 2006
2).2).-- Jan M Bjordal1, Christian Couppé2, Roberta T Chow3Jan M Bjordal1, Christian Couppé2, Roberta T Chow3. . A systematic review of low level laser A systematic review of low level laser
therapy with locationtherapy with location--specific doses for pain from chronic joint disordersspecific doses for pain from chronic joint disorders 11University of Bergen, University of Bergen,
Norway Norway 22Lund University, Sweden Lund University, Sweden 33PrivatePrivate Medical Practice, Sydney. Australian Journal of Medical Practice, Sydney. Australian Journal of
Physiotherapy Physiotherapy 49: 10749: 107--116]116]

22/01/2010
8
Para mejorar la funciónPara mejorar la función�� Ejercicios autopasivos apertura mandibularEjercicios autopasivos apertura mandibular
�� Ejercicios excéntricosEjercicios excéntricos
�� Ejercicios activosEjercicios activos
�� Distracción pasiva ATM:Distracción pasiva ATM:
�� Incrementa movilidad/inhibir músculos elevadoresIncrementa movilidad/inhibir músculos elevadores
�� Mano cráneo/ pulgar sobre 2º molar inferior Mano cráneo/ pulgar sobre 2º molar inferior �� Fuerza distracción segundos/relajación (varias veces)Fuerza distracción segundos/relajación (varias veces)
1).1).-- Margaret L McNeely, Susan Armijo Olivo, David J Magee .Physical Therapy . Volume 86 . Number 5 . May 2006. A Margaret L McNeely, Susan Armijo Olivo, David J Magee .Physical Therapy . Volume 86 . Number 5 . May 2006. A Systematic Review of the Effectiveness of Physical Therapy Interventions for Temporomandibular DisordersSystematic Review of the Effectiveness of Physical Therapy Interventions for Temporomandibular Disorders
2). 2). -- Marega S Medlicott, Susan R Harris: A systematic reviewed of the effectiveness of exercise, manual therapy, Marega S Medlicott, Susan R Harris: A systematic reviewed of the effectiveness of exercise, manual therapy, electrotherapy, relaxation training, and biofeedback in the managment of temporomandibular disorder. Physical electrotherapy, relaxation training, and biofeedback in the managment of temporomandibular disorder. Physical Therapy. 86,7. July 2006Therapy. 86,7. July 2006
Tto farmacológicoTto farmacológico
�� Solo para síntomas asociadosSolo para síntomas asociados�� ANALGESICOSANALGESICOS
�� AINES AINES
�� CORTICOIDESCORTICOIDES�� 1 Inyección ia hidrocortisona 1 Inyección ia hidrocortisona �� Múltiples Múltiples ---- nocivas para las estructuras articularesnocivas para las estructuras articulares
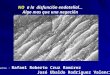
Tratamiento con férula oclusalTratamiento con férula oclusal
�� Años 70, Farrar:Años 70, Farrar:�� Férula reposición anteriorFérula reposición anterior
�� Diversos estudios muestran respuesta al tto:Diversos estudios muestran respuesta al tto:�� Posición condilar más anterior (sin recapturar disco) Posición condilar más anterior (sin recapturar disco)
�� Evita presión tejidos retrodiscales/ dolorEvita presión tejidos retrodiscales/ dolor�� Cambios adaptativos y reparativos (fibrosis)/carga no Cambios adaptativos y reparativos (fibrosis)/carga no dolorosadolorosa
�� Diversos estudios concluyenDiversos estudios concluyen�� Relación oclusal tras férula no se modifica.Relación oclusal tras férula no se modifica.�� 66 % ruídos articulares.66 % ruídos articulares.�� Ruidos articulares muy comunes población general Ruidos articulares muy comunes población general
�� no relación : dolor, reducción movilidad, predictores de no relación : dolor, reducción movilidad, predictores de trastornos evolutivostrastornos evolutivos
�� Solo 25 % con dolor/ objetivo terapéuticoSolo 25 % con dolor/ objetivo terapéutico
1).1).-- D Eberhard, HD Eberhard, H--P. Batleon and W. StegerP. Batleon and W. Steger ..The efficacy on anterior repositioning splint therapy study by The efficacy on anterior repositioning splint therapy study by magnetic resonance imagingmagnetic resonance imaging.. European Journal of Orthodontics... European Journal of Orthodontics.
2).2).-- Edmond Truelove, DDS, MSD; Kimberly Hanson Huggins, RDH, BS; Lloyd Mancl, PhD; Samuel F. Edmond Truelove, DDS, MSD; Kimberly Hanson Huggins, RDH, BS; Lloyd Mancl, PhD; Samuel F. DworkinDworkin The efficacy of traditional, lowThe efficacy of traditional, low--cost and nonsplint therapies for temporomandibular cost and nonsplint therapies for temporomandibular disorderdisorder A randomized controlled trialA randomized controlled trial, DDS, PhD , DDS, PhD JADA, Vol. 137 August 2006 American Dental Association JADA, Vol. 137 August 2006 American Dental Association
�� Efectos 2º férula RAEfectos 2º férula RA
�� Mordida abierta posterior por contractura reversible m. Mordida abierta posterior por contractura reversible m. pterigoideo externo inferiorpterigoideo externo inferior
�� Proporcional a tiempo de ferulización:Proporcional a tiempo de ferulización:�� Al ppio 24 horas durante 3Al ppio 24 horas durante 3--6 meses6 meses�� Actualmente se reduce al máximo el tiempo al necesario para Actualmente se reduce al máximo el tiempo al necesario para reducir síntomasreducir síntomas
�� Noches (bruxismo)Noches (bruxismo)
�� Contraindicada:Contraindicada:Desplazamiento disco sin reducciónDesplazamiento disco sin reducción
Agravará desplazamiento anteriorAgravará desplazamiento anterior
Férula reposición anterior
Férula relajación muscular

22/01/2010
9
�� CORRECCION OCLUSAL CORRECCION OCLUSAL ------ Estudios a largo plazo Estudios a largo plazo
�� Supone tto dental extensoSupone tto dental extenso
�� Adaptación natural funciona bien en mayoría pacientesAdaptación natural funciona bien en mayoría pacientes
�� Reconstrucción ortodóncica : sólo pacientes inestabilidad Reconstrucción ortodóncica : sólo pacientes inestabilidad ortopédica importante.ortopédica importante.
1).1).-- Waseem Jerjes*1,2,3,4, Tahwinder Upile2,3,4, Syedda Abbas2, Panagiotis Kafas5, Michael Waseem Jerjes*1,2,3,4, Tahwinder Upile2,3,4, Syedda Abbas2, Panagiotis Kafas5, Michael
Vourvachis2, Jubli Rob6, Eileen Mc Carthy2, Nikolaos Angouridakis7 and Colin Hopper1,2,3 Vourvachis2, Jubli Rob6, Eileen Mc Carthy2, Nikolaos Angouridakis7 and Colin Hopper1,2,3 Muscle disorders and Muscle disorders and
dentitiondentition--related aspects in temporomandibular disorders: controversies in the most commonly used related aspects in temporomandibular disorders: controversies in the most commonly used
treatment modalitiestreatment modalities International Archives of Medicine International Archives of Medicine 2008, 2008, 11:23 doi:10.1186/1755:23 doi:10.1186/1755--76827682--11--2323
Otros tratamientosOtros tratamientos
�� Tto quirúrgicoTto quirúrgico�� ArtroscópicoArtroscópico�� A cielo abiertoA cielo abierto
�� AcupunturaAcupuntura
�� Mejoras estadísticamente significativasMejoras estadísticamente significativas
�� Acido hialurónicoAcido hialurónico
1).1).-- Shen YF, Godard G. Shen YF, Godard G. THE SHORTTHE SHORT--TERM EFFECT OF ACUPUNCTURE ON MYOFASCIAL PAIN PATIENTS AFTER CLENCHINGTERM EFFECT OF ACUPUNCTURE ON MYOFASCIAL PAIN PATIENTS AFTER CLENCHING. Center for orofacial pain. . Center for orofacial pain. University of California, San Francisco. Pain Pract 2007 Sept 7 (3) 256University of California, San Francisco. Pain Pract 2007 Sept 7 (3) 256--6464
2).2).-- Smith P. Mosscrop D, Davies S, Sloan P, AlSmith P. Mosscrop D, Davies S, Sloan P, Al-- AniZ AniZ THE EFFICACY OF ACUPUNCTURE IN THE TREATMENT OF TM JOINT MYOFASCIAL PAIN: A THE EFFICACY OF ACUPUNCTURE IN THE TREATMENT OF TM JOINT MYOFASCIAL PAIN: A RANDOMISED CONTROLLED TRIALRANDOMISED CONTROLLED TRIAL.. School of Dentistry, The university of Manchester. U.K. J. Dent. Mar; 35(3): 259.. School of Dentistry, The university of Manchester. U.K. J. Dent. Mar; 35(3): 259--6767
�� TTO LIBERACION PG MIOFASCIALESTTO LIBERACION PG MIOFASCIALES::�� Correcciones posturalesCorrecciones posturales�� Sprays frío y estiramientos (previo calor) Sprays frío y estiramientos (previo calor)
�� Cuidadosa si sospecha DTMCuidadosa si sospecha DTM�� Inhibición recíproca (Contracción isométrica autorresistida)Inhibición recíproca (Contracción isométrica autorresistida)
�� Liberación por presiónLiberación por presión�� RasgueoRasgueo�� Infiltración anestésico localInfiltración anestésico local�� Punción secaPunción seca�� Infiltración con toxina botulínicaInfiltración con toxina botulínica
1).1).-- Travel y Simons.Travel y Simons. Dolor y disfunción miofascial. El manual de los puntos gatillo. Dolor y disfunción miofascial. El manual de los puntos gatillo.
Editorial médica panamericana. 2ª edición. 2002.Editorial médica panamericana. 2ª edición. 2002.
2).2).-- Lee SJ, McCall WD, Jr., Kim YK, Chung SC, Chung JW: Effect of botulinum toxin injection on nocturnal bruxism: Lee SJ, McCall WD, Jr., Kim YK, Chung SC, Chung JW: Effect of botulinum toxin injection on nocturnal bruxism:
A randomized controlled trial. Am J Phys Med Rehabil 2010;89:16A randomized controlled trial. Am J Phys Med Rehabil 2010;89:16––23.23.
3).3).-- Kurtoglu. Gur OH. Kurkcu Effect of Botulinum toxinKurtoglu. Gur OH. Kurkcu Effect of Botulinum toxin--A in myofascial pain patient with or without functional disc A in myofascial pain patient with or without functional disc
displacement. M. University of Cukurova, Adana, Turkey. J. Oral Maxilofac. Surg. 2008 Aug 66(8) 1644displacement. M. University of Cukurova, Adana, Turkey. J. Oral Maxilofac. Surg. 2008 Aug 66(8) 1644--5151
CONCLUSIONESCONCLUSIONES1.1.-- Tto educacional y físicoTto educacional y físico: los más recomendables: los más recomendables
MC últimos estadíosMC últimos estadíos�� Temor dolor últimos grados apertura mandibularTemor dolor últimos grados apertura mandibular�� Ligera reducción apertura bucalLigera reducción apertura bucal
2.2.-- Papel Médico RehabilitadorPapel Médico Rehabilitador�� Tto dolores miofascialesTto dolores miofasciales�� Tto conjunto con otras especialidadesTto conjunto con otras especialidades
1).1).--Marega S Medlicott, Susan R Harris:Marega S Medlicott, Susan R Harris: A systematic reviewed of the effectiveness of exercise, manual therapy, A systematic reviewed of the effectiveness of exercise, manual therapy, electrotherapy, relaxation training, and biofeedback in the managment of temporomandibular disorderelectrotherapy, relaxation training, and biofeedback in the managment of temporomandibular disorder. Physical Therapy. . Physical Therapy. 86,7. July 2006 (108 art 96 86,7. July 2006 (108 art 96 --2005)2005)
2).2).-- Margaret L McNeely, Susan Armijo Olivo, David J Magee .Physical Therapy . Volume 86 . Number 5 . May 2006. A Systematic ReMargaret L McNeely, Susan Armijo Olivo, David J Magee .Physical Therapy . Volume 86 . Number 5 . May 2006. A Systematic Review view of the Effectiveness of Physical Therapy Interventions for Temporomandibular Disordersof the Effectiveness of Physical Therapy Interventions for Temporomandibular Disorders
¡ ¡ MUCHAS MUCHAS
GRACIASGRACIAS !!