Embed Size (px)
Citation preview

KINESIOLOGÍA EN BRONQUIOLITIS AGUDA
Kinesiólogo Claudio Torres Tapia.Terapista Respiratorio Certificado
Coordinador 4º turno UPCI CAVRR- Los AngelesPrograma AVNI- Servicio de Salud Biobio

BRONQUIOLITIS AGUDA
• Primer episodio agudo de dificultad respiratoria con sibilancias, precedido por un cuadro catarral de vías altas (rinitis, tos, con/sin fiebre), que afecta a niños menores de 2 años An Pediatr (Barc). 2010. doi:10.1016/j.anpedi.2009.11.020
• Actualmente usado indistintamente para los siguientes cuadros de obstrucción viral siempre que no se plantee el diagnostico de asma del lactante. Enfoque clínico de las enfermedades respiratorias del niño, Sanchez-Prado. 2007.

obstrucción multifactorial
controversia Medidas
Terapéuticas
• Caracterizado por inflamación aguda edema de la mucosa, hipersecreción, broncoespasmo y necrosis epitelial.
• sibilancias y crepitaciones
• hiperinsuflación.
• focos condensantes.

EPIDEMIOLOGÍA• principal causa de hospitalización en lactantes menores (epidémico)
• curso similar al VRS (90%)
• 1º año de vida 80%
• 100% a los 2 años.
• 15% desarrolla bronquiolitis.
• 3% requiere hospitalización
• multiples factores de riesgos de bronquiolitis grave.
• otros agentes: Influenza, Rinovirus, Metapneumovirus, adenovirus.
• asociado a sibilancias recurrentes.

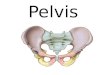
CONSIDERACIONES ANATÓMICAS Y FUNCIONALES DEL LACTANTE

Consideraciones Anatómicas y Funcionales del Lactante

INTERVENCIONES EN BRONQUIOLITIS
profilaxis en niños con factores de riesgo: beneficioso el uso de anticuerpos monoclonales
Prevención de la propagación: podría ser beneficioso
aislamiento en cohorte
lavado de manos
batas
mascarillas
guantes y gafas de protecciónJuan Manuel Lozano, Evidence 2007;10:308

INTERVENCIONES EN BRONQUIOLITIS
Tratamiento: Efectividad demostrada Emerg Med Clin N Am 25 (2007) 961–979
•Oxigenoterapia
•Hidratación.
• succión nasal.
• VM.
•Nbz. solución hipertónica. Zhang L, Mendoza-Sassi RA, Wainwright C, Klassen TP. Nebulized hypertonic saline so- lution for acute bronchiolitis in infants. Cochrane Database of Systematic Reviews 2008, Issue 4

INTERVENCIONES EN BRONQUIOLITIS
Tratamiento: Efectividad no demostrada
• aerosolterapia.
• B2 oral.
• montelukast Am J Respir Crit Care Med Vol 178. pp 854–860, 2008
• antivirales
• surfactantes
• ATB Spurling GKP, Fonseka K, Doust J, Del Mar C. Antibiotics for bronchiolitis in children. Cochrane Database of Systematic Reviews 2007
• Corticoesteroides (improbable que sea beneficicoso)
• fisioterapia respiratoriaJuan Manuel Lozano, Evidence 2007;10:308

EVIDENCIA DISPONIBLE...
• TEF, DP/vibraciones, grupo control no mejoran los parámetros cardiorrespiratorios, podría disminuir FR a largo plazo. J Bras Pneumol. 2009;35(9):860-867
• CPT (vibración/percusión) no disminuye los días de hospitalización, requerimientos de O2 ni mejoría en los score clínicos. Perrotta C, Ortiz Z, Roqué i Figuls M. Chest physiotherapy for acute bronchiolitis in paediatric patients between 0 and 24 months old. Cochrane Database of Systematic Reviews 2007
• Aceleración de flujos espiratorios/tos asistida no tiene efectos significativos en lactantes con BA e historia de atopia. Gajdos V, Katsahian S, Beydon N, Abadie V, de Pontual L, et al. (2010) Effectiveness of Chest Physiotherapy in Infants Hospitalized with Acute Bronchiolitis: A Multicenter, Randomized, Controlled Trial

CRÍTICAS A LA EVIDENCIA
• Técnicas de CPT no consideran diferencias anatomofuncionales de los lactantes.
• anglosajones: técnicas de alto impacto (deletéreas)
• extrapolación de lo realizado en adultos.
• no consideran la combinación con otras terapias de apoyo.

A y B bronquios de cerdo de una semana de edad sometidos a Pº intraluminal de +5 y -5 cmH2O respectivamente.
Eur Respir J 1997; 10: 322–329

PROPUESTA...

• espiración lenta prolongada/tos provocada
• 19 lactantes
• score de Wang
• oximetría de pulso
• FC
Kinesither Rev 2006;(55):35-41
R É S U M É
But de l’étude. Évaluer l’efficacité et l’innocuité de la séancede kinésithérapie respiratoire (KR) associant Expiration LenteProlongée et Toux Provoquée chez des nourrissons hospitali-sés pour bronchiolite aiguë modérée.Matériel et Méthode. Étude prospective longitudinale de19 nourrissons (7,75 ± 6,6 mois, moyenne ± SD). Les patientssont évalués avant et après 57 séances de kinésithérapie com-prenant ELPr : Expiration Lente Prolongée et TP : Toux Pro-voquée. Le score de sévérité clinique de Wang (CS), l’oxy-métrie pulsée (SpO2), la fréquence cardiaque (FC), lesépisodes antérieurs de bronchiolite (AB), la prématurité (AP)et la présence d’anomalies radiologiques (RX) ont été calcu-lés pour l’effet séance et l’effet jour aux premier (J1), deuxième(J2) et dernier jours (JD).Résultats. CS (n = 19) : 4,3 ± 2 (moy ± SD), 3,7 ± 1,8, 2,1± 1,3 avant KR comparé à : 2,1 ± 0,8, 1,8 ± 1,1, 0,9 ± 0,6respectivement après KR (p < 0,001). SpO2 (n = 18) : 96,2± 2,2, 96,8 ± 2,4 et 97,1 ± 1,4, comparé à : 97,67 ± 1,57,98,28 ± 1,56, 98,67 ± 1,27 (p < 0,001). FC (n = 16) : 149,4± 17,4, 148,7 ± 17,4, 145,1 ± 16,4, comparé à : 142,2 ± 16,4,138,7 ± 14,4, 134,4 ± 13,1 (p < 0,001). Nombre moyen deséances (NS) : 3,8 ± 1,7. Un effet jour est observé sur CS
(p < 0,028), et l’effet séance diffère à J1 et JD pour AB surCS (p = 0,020) et sur SpO2 (p < 0,039). Le coefficient decorrélation entre CS et SpO2 est exprimé par Y = – 0,4716X + 98,55, r = – 0,407, p < 0,001. Un seul effet adverse estobservé. Conclusion. Le protocole de kinésithérapie respiratoire asso-ciant Expiration Lente Prolongée et Toux provoquée peutcontribuer à l’amélioration clinique des symptômes de l’obs-truction bronchique dans la bronchiolite aiguë modérée dunourrisson et ne présente pas de risque.
35
Kinesither Rev 2006;(55):35-41SavoirsContribution originale
Effets de la kinésithérapie respiratoire associantExpiration Lente Prolongée et Toux Provoquée
dans la bronchiolite du nourrissonGUY POSTIAUX (1), ROBERT DUBOIS (2), ETIENNE MARCHAND (1),
MICHEL DEMAY (2), JEAN JACQUY (2), MYLÈNE MANGIARACINA (1)
M O T S C L É S
Bronchiolite viraleChest PhysiotherapyExpiration Lente ProlongéeKinésithérapie respiratoireNourrissonObstruction bronchiqueToux Provoquée
La preuve scientifique de l’efficacité de la kinésithérapierespiratoire dans la bronchiolite du nourrisson n’est pas établie.L’utilisation d’un score clinique validé de l’obstructionbronchique peut contribuer à objectiver les effets des techniquesde désobstruction chez le nourrisson atteint de bronchiolitevirale.
(1) Centre Hospitalier Notre-dame et Reine Fabiola, Service de médecineinterne, Unité de pneumologie (Dr Guy Alsteens, Dr Etienne Marchand),Avenue du Centenaire, 73, 6061 Montignies-Sur-Sambre, Belgique.(2) Centre Hospitalier Universitaire, Unité de pédiatrie (Dr MichelDemay), Boulevard Paul Janson, 6000 Charleroi, Belgique.Correspondance : Guy Postiaux E-mail : [email protected]
AbréviationsAB = antécédents de bronchioliteAFE = augmentation lente du flux expiratoireAP = antécédent de prématuritécCPT = Conventional Chest PhysiotherapyCS = score de sévérité clinique de WangnCPT = New Chest PhysiotherapyELPr = expiration lente prolongéeFC = fréquence cardiaqueGA = aspect cliniqueNS = nombre de séances.RE = tirageRR = rythme respiratoireRX = anomalie radiologiqueSpO2 = oxymétrie pulséeTP = toux provoquéeWh = sibilances
Kinesither Rev 2006;(55):35-41
37
Effets de la kinésithérapie respiratoire
KinésithérapieLe premier jour après l’admission, les patients ont bé-néficié du protocole de kinésithérapie comprenantELPr, qui consiste en une pression bi-manuelle lenteexercée par le kinésithérapeute simultanément sur lethorax et l’abdomen dans le sens expiratoire dans levolume de réserve expiratoire (VRE), et la TP qui estune toux réflexe déclenchée par une pression trachéalebrève appliquée au-dessus de l’incisure sternale. Enraison de la fréquente tachypnée présentée par les en-fants broncho-obstructifs, la pression thoraco-abdomi-nale peut être exercée durant deux ou trois phases ex-piratoires consécutives pour obtenir la meilleuredéflation pulmonaire possible. Le nombre moyen de manœuvres est d’environ 20 ap-pliquées durant 20-30 minutes. L’enfant est placé endécubitus dorsal en position surélevée (35°) pour mi-nimiser le risque de reflux gastro-œsophagien (RGO)[10]. Le traitement est appliqué au moins deux heuresaprès le dernier repas pour éviter le réflexe de vomis-sement lors de l’expectoration. Même si l’action des bronchodilatateurs est controver-sée ou de courte durée dans la bronchiolite [11], la ki-nésithérapie est appliquée à une distance d’au moins3 heures de toute nébulisation pour éviter un biais ré-sultant de l’effet des médications. Les patients ont reçuune séance par jour jusqu’à normalisation du score cli-nique de Wang (CS) appréciée par le médecin.
MesuresTrois catégories de paramètres ont été mesurées avantet 15 minutes après le traitement lorsque l’enfant estcalme et en l’absence de pleurs ; 1) les paramètres cli-niques composant le score de Wang (Tableau I) [12] :rythme respiratoire (RR), sibilances – wheezing (Wh),
tirage – rétraction (RE) et appréciation de l’état cli-nique – general appearance (GA). Le score attribue unevaleur de 0 à 3 à chaque variable, les plus atteints re-cevant le score le plus élevé ; 2) les paramètres objec-tifs: oxymétrie pulsée (SpO2) (Ohmeda Biox 3700) etfréquence cardiaque (FC) ; 3) les épisodes antérieursde bronchiolite (AB), de prématurité – âge gestation-nel inférieur à 34 semaines (AP), et la présence d’ano-malies radiologiques (RX) (hyperinflation et/ou opa-cités), sont notés. Les enfants sont leur proprecontrôle et sont évalués par deux investigateurs n’as-sistant pas au traitement (GP et RD). Le kinésithéra-peute traitant (MM) ignore les résultats jusqu’à la finde l’étude.
StatistiqueLe calcul statistique porte sur quatre groupes de va-riables. L’analyse de variance pour tester : 1) les diffé-rences de CS, SpO2 et FC avant (valeur basale) et aprèskinésithérapie respiratoire (KR) (effet séance) aux pre-mier (J1), deuxième (J2) et dernier jours (JD), lesvariations dans le temps (effet jour) des séances ; 2) lesrelations entre AB, AP, RX et les effets séance et jour ;3) le calcul de régression logistique pour variables noncontinues pour évaluer les relations entre l’âge, AB, AP,RX, CS, SpO2, considérant comme bon répondeur à laKR une amélioration de CS d’au moins deux points ;4) le t test de Mann – Whitney – Wilcoxon pour échan-tillons indépendants pour tester la relation entre lenombre de séances (NS) et AB, AP, RX. Le coefficientde corrélation est calculé entre CS et SpO2. Une valeurde p < 0,05 est considérée comme statistiquementsignificative.
Résultats
22 enfants ont été inclus dans l’étude. 60 séances de KRont été réalisées. 3 patients ont été écartés du calcul sta-tistique en raison de données incomplètes, 57 séancessur 19 enfants (10 sujets masculins, 9 sujets féminins)ont été retenues. L’âge moyen des enfants retenus estde 7,75 ± 6,6 mois (extrêmes : 1 à 23). Le nombre deséances était de 3,8 ± 1,7. 6/19 patients (32%) avaientdes antécédents de bronchiolite (un épisode pour 5 pa-tients, 2 épisodes pour 1 patient), 5/19 (26%) patientsavaient des antécédents de prématurité et 9/19 (47%)avaient des signes radiologiques positifs. Les résultatssont exprimés en moyenne ± SD.A J1, J2 et JD, l’effet séance sur CS (n = 19), SpO2(n = 18), et FC (n = 16) sont hautement significatifs (p < 0,001). CS (n = 19) est : 4,3 ± 2 ; 3,7 ± 1,8 ; 2,1 ± 1,3 avant KR respectivement, comparé à : 2,1 ± 0,8 ;1,8 ± 1,1 ; 0,9 ± 0,6 après KR (significativement amé-lioré : p < 0,001) (figure 1). SpO2 (n = 18) : 96,2 ± 2,2 ;96,8 ± 2,4 et 97,1 ± 1,4, comparé à : 97,7 ± 1,6 ;
Tableau I. Score de sévérité clinique de Wang. Le scoreattribue une cotation de 0 à 3 à chaque variable, une sévéritécroissante recevant un score de plus en plus élevé.Respiratory rate = rythme respiratoire, wheezing = sibilances,rétractions = tirage, general condition = appréciation de l’étatclinique [12].
0 1 2 3
Respiratory rate < 30 31-45 46-60 > 60
Wheezing None Terminal Entire Inspirationexpiration expiration and
or only with or audible expirationstethoscope on expiration without
without stethoscopestethoscope
Retractions None Intercostal Tracheosternal Severe withonly nasal flaring
General Normal Irritable,condition lethargic,
poor feeding

TELPR
• aplicación de una presión bimanual toraco-abdominal pasiva
• obtener una espiración lenta prolongada hasta VRE
• controlada por los ruidos respiratorios en la boca
• 2 a 3 ciclos seguidos para favorecer mayor deflación pulmonar

98,3 ± 1,6 ; 98,7 ± 1,3 (p < 0,001). FC (n = 16) : 149,4± 17,4 ; 148,7 ± 17,4 ; 145,1 ± 16,4, comparé à : 142,2± 16,4 ; 138,7 ± 14,4 ; 134,4 ± 13,1 (p < 0,001) (figure 2).L’effet jour est significatif sur CS (p < 0,028) et non si-gnificatif sur SpO2 (p = 0,989) et FC (p = 0,649). L’ef-fet séance est significativement différent sur CS entre lespatients avec AB et sans AB (p = 0,02) (figure 3). A J2et JD, l’effet séance est significativement inférieur (p =0,031) pour les patients avec AB (p < 0,039). A J1, lavaleur basale de CS et l’effet séance ne diffèrent pas si-gnificativement pour les patients sans et avec AB. Au-cune relation de SpO2 et FC avec AB, AP ou RX sur l’ef-
fet séance ou l’effet jour n’est observée. Le coefficientde corrélation linéaire entre CS et SpO2 est Y = – 0,4716X + 98,55 ; r = – 0,407, p < 0,001 (figure 4).
Discussion
cCPT versus KRÀ notre connaissance sont ici rapportés pour la pre-mière fois des résultats objectivant l’action de la kiné-sithérapie respiratoire sur certains symptômes d’obs-truction bronchique présents dans la bronchiolite du
Kinesither Rev 2006;(55):35-41
38
GUY POSTIAUX et al.
Effet séance sur CS7,0
6,0
5,0
4,0
3,0
2,0
1,0
0,0J1 J2 JD
Jours
CS Av KR
Ap KR
Figure 1. Effet des séances de kinésithérapie respiratoire (KR)sur le score de sévérité clinique de Wang (CS) aux premier J1,deuxième J2, et dernier jour JD. CS diffère significativement(p < 0,001) avant (Av KR) et après Ap KR) et chaque jour.L’effet jour est significatif (p = 0,028) N = 19.
Effet de nCPT sur la Sp02
102,00
100,00
98,00
96,00
94,00
92,00
90,00J1 J2 JD
Jours
Sp0
2 Av KR
Ap KR
Figure 2. Effet des séances de kinésithérapie respiratoire (KR)sur la saturation (SpO2) aux premier J1, deuxième J2, etdernier jour JD. SpO2 diffère significativement (p < 0,001)avant et après KR et chaque jour. L’effet jour n’est passignificatif.
Effet de AB sur CS8,000
7,000
6,000
5,000
4,000
3,000
2,000
1,000
0,000J1 avKR J1 apKR J2 avKR J2 apKR JD avKR JD apKR
AB-
AB+CS
CS à J1, J2, JD
Figure 3. Relation entre CS (moyenne ± SD) et AB. Un effetjour est observé : p < 0,020. A J1, il n’y a pas d’influence deAB sur les valeurs basales mais l’effet séance estsignificativement différent sur CS entre les patients avec AB etsans AB (p = 0,02). A J2 et JD, les valeurs basales et l’effetséance sont significativement différents p = 0,031.
102
100
98
96
94
92
90
880 2
y = -0,4716x + 98,55
4 6 8
Cœfficient de corrélation entre CS et Sp02
Sp0
2
CS
Figure 4. Coefficient de corrélation entre le score clinique deWang (CS) et la saturation (SpO2). La régression linéaire estcalculée pour: Y = – 0,4716 X + 98, 55 ; r = – 0,407,p < 0,001.
98,3 ± 1,6 ; 98,7 ± 1,3 (p < 0,001). FC (n = 16) : 149,4± 17,4 ; 148,7 ± 17,4 ; 145,1 ± 16,4, comparé à : 142,2± 16,4 ; 138,7 ± 14,4 ; 134,4 ± 13,1 (p < 0,001) (figure 2).L’effet jour est significatif sur CS (p < 0,028) et non si-gnificatif sur SpO2 (p = 0,989) et FC (p = 0,649). L’ef-fet séance est significativement différent sur CS entre lespatients avec AB et sans AB (p = 0,02) (figure 3). A J2et JD, l’effet séance est significativement inférieur (p =0,031) pour les patients avec AB (p < 0,039). A J1, lavaleur basale de CS et l’effet séance ne diffèrent pas si-gnificativement pour les patients sans et avec AB. Au-cune relation de SpO2 et FC avec AB, AP ou RX sur l’ef-
fet séance ou l’effet jour n’est observée. Le coefficientde corrélation linéaire entre CS et SpO2 est Y = – 0,4716X + 98,55 ; r = – 0,407, p < 0,001 (figure 4).
Discussion
cCPT versus KRÀ notre connaissance sont ici rapportés pour la pre-mière fois des résultats objectivant l’action de la kiné-sithérapie respiratoire sur certains symptômes d’obs-truction bronchique présents dans la bronchiolite du
Kinesither Rev 2006;(55):35-41
38
GUY POSTIAUX et al.
Effet séance sur CS7,0
6,0
5,0
4,0
3,0
2,0
1,0
0,0J1 J2 JD
Jours
CS Av KR
Ap KR
Figure 1. Effet des séances de kinésithérapie respiratoire (KR)sur le score de sévérité clinique de Wang (CS) aux premier J1,deuxième J2, et dernier jour JD. CS diffère significativement(p < 0,001) avant (Av KR) et après Ap KR) et chaque jour.L’effet jour est significatif (p = 0,028) N = 19.
Effet de nCPT sur la Sp02
102,00
100,00
98,00
96,00
94,00
92,00
90,00J1 J2 JD
Jours
Sp0
2 Av KR
Ap KR
Figure 2. Effet des séances de kinésithérapie respiratoire (KR)sur la saturation (SpO2) aux premier J1, deuxième J2, etdernier jour JD. SpO2 diffère significativement (p < 0,001)avant et après KR et chaque jour. L’effet jour n’est passignificatif.
Effet de AB sur CS8,000
7,000
6,000
5,000
4,000
3,000
2,000
1,000
0,000J1 avKR J1 apKR J2 avKR J2 apKR JD avKR JD apKR
AB-
AB+CS
CS à J1, J2, JD
Figure 3. Relation entre CS (moyenne ± SD) et AB. Un effetjour est observé : p < 0,020. A J1, il n’y a pas d’influence deAB sur les valeurs basales mais l’effet séance estsignificativement différent sur CS entre les patients avec AB etsans AB (p = 0,02). A J2 et JD, les valeurs basales et l’effetséance sont significativement différents p = 0,031.
102
100
98
96
94
92
90
880 2
y = -0,4716x + 98,55
4 6 8
Cœfficient de corrélation entre CS et Sp02
Sp0
2
CS
Figure 4. Coefficient de corrélation entre le score clinique deWang (CS) et la saturation (SpO2). La régression linéaire estcalculée pour: Y = – 0,4716 X + 98, 55 ; r = – 0,407,p < 0,001.

98,3 ± 1,6 ; 98,7 ± 1,3 (p < 0,001). FC (n = 16) : 149,4± 17,4 ; 148,7 ± 17,4 ; 145,1 ± 16,4, comparé à : 142,2± 16,4 ; 138,7 ± 14,4 ; 134,4 ± 13,1 (p < 0,001) (figure 2).L’effet jour est significatif sur CS (p < 0,028) et non si-gnificatif sur SpO2 (p = 0,989) et FC (p = 0,649). L’ef-fet séance est significativement différent sur CS entre lespatients avec AB et sans AB (p = 0,02) (figure 3). A J2et JD, l’effet séance est significativement inférieur (p =0,031) pour les patients avec AB (p < 0,039). A J1, lavaleur basale de CS et l’effet séance ne diffèrent pas si-gnificativement pour les patients sans et avec AB. Au-cune relation de SpO2 et FC avec AB, AP ou RX sur l’ef-
fet séance ou l’effet jour n’est observée. Le coefficientde corrélation linéaire entre CS et SpO2 est Y = – 0,4716X + 98,55 ; r = – 0,407, p < 0,001 (figure 4).
Discussion
cCPT versus KRÀ notre connaissance sont ici rapportés pour la pre-mière fois des résultats objectivant l’action de la kiné-sithérapie respiratoire sur certains symptômes d’obs-truction bronchique présents dans la bronchiolite du
Kinesither Rev 2006;(55):35-41
38
GUY POSTIAUX et al.
Effet séance sur CS7,0
6,0
5,0
4,0
3,0
2,0
1,0
0,0J1 J2 JD
Jours
CS Av KR
Ap KR
Figure 1. Effet des séances de kinésithérapie respiratoire (KR)sur le score de sévérité clinique de Wang (CS) aux premier J1,deuxième J2, et dernier jour JD. CS diffère significativement(p < 0,001) avant (Av KR) et après Ap KR) et chaque jour.L’effet jour est significatif (p = 0,028) N = 19.
Effet de nCPT sur la Sp02
102,00
100,00
98,00
96,00
94,00
92,00
90,00J1 J2 JD
Jours
Sp0
2 Av KR
Ap KR
Figure 2. Effet des séances de kinésithérapie respiratoire (KR)sur la saturation (SpO2) aux premier J1, deuxième J2, etdernier jour JD. SpO2 diffère significativement (p < 0,001)avant et après KR et chaque jour. L’effet jour n’est passignificatif.
Effet de AB sur CS8,000
7,000
6,000
5,000
4,000
3,000
2,000
1,000
0,000J1 avKR J1 apKR J2 avKR J2 apKR JD avKR JD apKR
AB-
AB+CS
CS à J1, J2, JD
Figure 3. Relation entre CS (moyenne ± SD) et AB. Un effetjour est observé : p < 0,020. A J1, il n’y a pas d’influence deAB sur les valeurs basales mais l’effet séance estsignificativement différent sur CS entre les patients avec AB etsans AB (p = 0,02). A J2 et JD, les valeurs basales et l’effetséance sont significativement différents p = 0,031.
102
100
98
96
94
92
90
880 2
y = -0,4716x + 98,55
4 6 8
Cœfficient de corrélation entre CS et Sp02
Sp0
2
CS
Figure 4. Coefficient de corrélation entre le score clinique deWang (CS) et la saturation (SpO2). La régression linéaire estcalculée pour: Y = – 0,4716 X + 98, 55 ; r = – 0,407,p < 0,001.

Postiaux G. et al. Eur Resp J 2008; sept. n° 0126-2008
• evaluar durante 3 temporadas inviernos (2004-2005, 2005-2006, 2006-2007) la eficacia de un protocolo nCPT incluyendo ELPr + TP después de nebulización con SH 3% + salbutamol ®
• se evalua efectividad sobre score wang
• grupo control NBZ + SBT
0
1
2
3
4
5
6
7
Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 C
S
Control nCPT
p = 0,002
p = 0,056

Non-invasive ventilation as primary ventilatory support for infants with severe bronchiolitis Intensive Care Med (2008) 34:1608–1614
• aplicación de CPAP (5 a 10 cmH2O) precoz en BA severa.
• comparar con BA en VMC del invierno anterior
support duration was longer for infants who failed to NIVcompared to those for whomNIVwas successful (Table 3).Among the five infantswho failed toNIV, two had bacterialpulmonary co-infection of whom one had concomitanturinary infection. The two others had history of prematurityand heart disease, and presented with severe apnoea.
Discussion
In our PICU, a ventilation strategy based on NIV as theprimary ventilation support in infants with severe
bronchiolitis was associated with a lower rate of venti-lator-associated pneumonia, with a shortened duration ofsupplemental oxygen and with a trend of a reduction inthe length of hospital stay.
Previous studies carried out in adults with COPD hadshown that NIV may reduce the rates of bacterial pul-monary infections and improve the survival [6, 29, 30].For children, the mean duration of mechanical ventilationand PICU stay is longer for patients with VAP [31, 32].The rates of bacterial pulmonary co-infection observed inour study (28% in IV group, 22% in the NIV group) areconsistent with previous studies [5, 33–35]. Kneyber et al.
Table 1 Characteristics of infants with severe bronchiolitis: comparison between the IV (2003–2004) and the NIV period (2004–2005)
IV period (n = 53) NIV period (n = 27) p value
Medical pastAge in days: median (1st quartile–3rd quartile) 40 (26–75) 41 (22–61) 0.71Male number (%) 34 (64) 11 (41) \0.05Prematurity: number (%) 29 (54) 10 (40)d 0.22Chronic respiratory failure:a number 2 2 0.29Congenital heart disease: number 1 4Immunocompromised states number 2 0At least one risk factor:b number (%) 5 (9) 5 (19)Presenting symptomsDays ill before referral: median (range) 2 (1–4) 3 (2–4) 0.29Oxygen requirement on admission: number (%) 33 (67)e 15 (58)c 0.34Apnoea on admission: number (%) 35 (67)d 9 (33) \0.01Atelectasis on admission: number (%) 16 (34)f 5 (22)e 0.27Infants treated by antibiotics on admission number (%) 11 (21%) 3 (11%) 0.36PRISM II scoreg median (1st quartile–3rd quartile) 14 (9–18) 12 (8–15) 0.20
IV invasive ventilation; NIV non-invasive ventilationa Bronchopulmonary dysplasia, laryngo-tracheomalaciab Chronic respiratory failure, congenital heart disease, and/or immunocompromisedc Data unknown for 1 patientd Data unknown for 2 patientse Data unknown for 4 patientsf Data unknown for 7 patientsg Paediatric risk of mortality (PRISM); data unknown for 3 patients in IV group; using Wilcoxon Signed-Ranks test
Table 2 Outcome of infants admitted in PICU for severe bronchiolitis: comparison between the IV (2003–2004) and the NIV period(2004–2005)
IV period (n = 53) NIV period (n = 27) p value
Duration of ventilation support: median (1st–3rd quartile) 100 (60–176) 87 (24–144) 0.45Oxygen duration: median (1st–3rd quartile) 10 (5–14) 8 (3–10) 0.10Oxygen duration[8 days: number (%) 33 (65)c 10 (37) \0.05Bacterial pulmonary co-infections: number (%) 15 (28)b 5 (19) 0.32Ventilatory-associated pneumonia: number (%) 9 (17)d 0 \0.05Other infections:a number (%) 4 (8)b 1 (4) 0.66Infants treated by antibiotics during PICU stay number (%) 33 (62%) 7 (26%) \0.01Barotrauma: number (%) 2 (4) 2 (7) 0.26Length of stay (LOS) in days: median (1st–3rd quartile) 12 (9–17) 11 (7–13) 0.14LOS[10 days: number (%) 36 (68) 13 (48) 0.09
IV invasive ventilation; NIV non-invasive ventilationa Urinary tract infections, bacteraemiab Data unknown for 1 patientc Data unknown for 2 patientsd For infants in the NIV period, the rate of ventilator-associated pneumonia was only calculated among those who were not intubated atadmission (n = 23 infants). The unilateral exact Fischer Exact test was used in this situation
1611

• optimizar el uso de broncodilatador
• optimizar la evaluación de la mecánica respiratoria.
• reducir costos.
• aplicación de score de gravedad.
• minimizar complicaciones.
• reducir días de hospitalización.
• mejora satisfacción.
4. The respiratory therapy recommendations stickerswere placed in the chart separately from the orders, so thestickers were not routinely reviewed by the ordering phy-sician.5. RTs did not receive feedback on how they were per-
forming.A program was developed to address the RTs’ concerns
and to encourage respiratory function assessment, to de-termine the need for and effect of bronchodilator treat-ment. The program was implemented on January 14, 2002.It included:1. A revised respiratory assessment form (see Appendix
2). The revised form reflected the guideline recommenda-tion that nasal suctioning and respiratory scoring be doneprior to any bronchodilator treatment and that respiratoryscoring be done 15–30 min following treatment, to deter-mine if the treatment improved the respiratory score.2. A change in the respiratory score threshold for a
recommendation for bronchodilator treatment. Though arecommendation for bronchodilator treatment with a re-spiratory score of ! 2 was deemed appropriate for asthmapatients, that did not account for the typical presentation ofa bronchiolitis patient, which includes increased secre-tions, increased respiratory rate, and decreased air move-ment. Therefore, a respiratory score ! 3 was required torecommend bronchodilator treatment for a guideline-eli-gible bronchiolitis patient. Patients who warranted a trialbronchodilator therapy typically had elevated respiratoryrate, increased use of accessory muscles, decreased airexchange, and mild expiratory wheezes, due to increasedsecretions and airway inflammation. Figure 1 shows therevised treatment algorithm.3. Multidisciplinary rounds. When possible an RT ac-
companied the physician on morning rounds. Attendingphysicians familiar with the evidence encouraged the res-idents to listen to the RTs’ recommendations. The educa-tion coordinator for Health Policy and Clinical Effective-ness attended rounds 1 day each week, with each of the 3physician teams responsible for treating bronchiolitis pa-tients. She tracked eligible patients and reinforced use ofthe new respiratory assessment form and treatment recom-mendations.4. Improved effective, data-based communication be-
tween the RTs and physicians. The chart sticker (that sum-marized the RT’s recommendations) was discontinued andreplaced by the RTs making their recommendations ver-bally to the physician. Specifically, when an order waswritten for a bronchodilator treatment, the RT would dothe nasal suctioning and before-and-after-treatment scor-ing. If the post-suctioning score was ! 3, the RT wouldpage the physician who wrote the order and advise thatbronchodilator was unwarranted. If the post-suctioningscore was ! 3, the RT would conduct the treatment and
the post-treatment respiratory scoring and advise the phy-sician whether the therapy should be continued.5. Better-informed RTs. The respiratory therapy educa-
tion coordinator (author EC) reviewed the charts of allbronchiolitis patients daily and conducted biweekly meet-ings to increase communication among the RTs, to receivetheir opinions on what was and was not working, and toshare the data being regularly collected. Two RTs, onefrom the day shift and one from the night shift, becameguideline champions on the floor. Therapists were givenwatches with timers to remind them to conduct the fol-low-up respiratory scoring 15–30 min following broncho-dilator treatment.
Study Population
Guideline-eligible patients were infants " 1 year oldand admitted to the hospital with a first-time episode ofuncomplicated bronchiolitis.35,36 All guideline-eligible pa-tients were included in the study, except for infants whohad histories of cystic fibrosis, immunodeficiency, con-genital heart disease, bronchopulmonary dysplasia, con-genital airway disease, or any other comorbid condition
Fig. 1. Infant bronchiolitis treatment algorithm.
QUALITY CARE FOR INFANTS WITH BRONCHIOLITIS
RESPIRATORY CARE • JUNE 2004 VOL 49 NO 6 591
Original Contributions
Empowering Respiratory Therapists to Take a More Active Rolein Delivering Quality Care for Infants With Bronchiolitis
Edward Conway RRT, Pamela J Schoettker MSc, Kate Rich, Amy Moore CRT,Maria T Britto MD MPH, and Uma R Kotagal MBBS MSc
BACKGROUND: Cincinnati Children’s Hospital Medical Center developed a bronchiolitis-treat-ment guideline and implemented a program, led by respiratory therapists, to encourage the use ofrespiratory function assessment to determine the need for and effect of bronchodilator treatment ofinfant bronchiolitis patients. METHODS: The program was implemented on January 14, 2002, andincluded (1) a revised respiratory scoring form, (2) a change in the respiratory score threshold fora recommendation of bronchodilator treatment, (3) establishment of multidisciplinary rounds, (4)providing current data to the respiratory therapists, and (5) increasing effective data-based com-munication between the respiratory therapists and physicians. Guideline-eligible patients admittedbefore the implementation of the program (between 12/1/01 and 1/13/02) were compared to patientsadmitted during the program (between 1/14/02 and 3/31/02). We compared the mean numbers ofbronchodilator treatments per patient in fiscal years 2001 and 2002. We defined “perfect respira-tory care” as administration of bronchodilator only if preceded by suction treatment that resultedin a post-suction respiratory score > 3. RESULTS: Documentation of respiratory scoring signifi-cantly increased following implementation of the program, as did “perfect respiratory care.” Be-tween the 2001 and 2002 bronchiolitis seasons, there was a decrease in both the mean number andthe variability in the number of bronchodilator doses administered. CONCLUSIONS: Expandingguideline recommendations to the level of specific protocols and empowering respiratory therapiststo take a more active role improve the quality of care for infant bronchiolitis patients. Key words:bronchiolitis, guideline, protocol, evidence-based medicine, respiratory therapy, suction, bronchodilator.[Respir Care 2004;49(6):589–599. © 2004 Daedalus Enterprises]
Introduction
Bronchiolitis is an acute inflammatory disease of thelower respiratory tract, resulting from obstruction of smallairways. It is initiated by infection of the upper respiratorytract by any one of several seasonal viruses, the mostcommon of which is respiratory syncytial virus (RSV).1–4Bronchiolitis is the most common cause of pediatric hos-pital admission during the winter months, and since 1980the hospitalization rate of children suffering bronchiolitishas increased over 200%.5
SEE THE RELATED EDITORIAL ON PAGE 581
There is considerable disagreement about and variabil-ity in the clinical management of infant bronchiolitis. Var-ious therapies have been advanced and practiced, but mosthave been shown to be ineffective when tested in rigorousclinical trials.6,7 Ribavirin, interferon-! and vitamin A havenot been effective in clinical practice.8–11 One well-con-ducted systematic review found shorter duration of stay
Edward Conway RRT and Amy Moore CRT are affiliated with theDivision of Respiratory Care; Pamela J Schoettker MSc, Kate Rich, andUma R Kotagal MBBS MSc are affiliated with the Division of HealthPolicy and Clinical Effectiveness; and Maria T Britto MD MPH is af-filiated with the Division of Adolescent Medicine—Cincinnati Children’sHospital Medical Center, Cincinnati, Ohio.
A version of this report was present at the American Association forRespiratory Care OPEN FORUM at the 48th International Respiratory Con-gress, held October 5–8, 2002, in Tampa, Florida.
Correspondence: Edward Conway RRT, Department of Respiratory Care,Children’s Hospital Medical Center, 3333 Burnet Avenue, Cincinnati OH45229-3039. E-mail: [email protected].
RESPIRATORY CARE • JUNE 2004 VOL 49 NO 6 589
RESPIRATORY CARE • JUNE 2004 VOL 49 NO 6


delivery was shorter with the Aeroneb Pro (2 min) thanwith the Mistyneb (10 min) (p ! 0.001). The efficiency ofthe jet nebulizer was consistent with other animal modelsand in vivo infant studies, but deposition with the AeronebPro was greater than previously reported from a nebulizerin infant ventilation.
Outcome Studies in Ventilated Infants
The relatively low efficiency of aerosol deposition dur-ing infant ventilation may be misleading, in that a small
absolute lung dose provides a larger dose/kg of bodyweightthan in adults. It is more clinically relevant to evaluate thephysiological effect of a pharmacologic aerosol than todwell on scant deposition data.
Bronchodilators
Rotschild et al36 studied 20 ventilator-dependent infants(weighing! 1,500 g) and found that 2.5 mg of aerosolizedalbuterol improved static compliance significantly morethan placebo and decreased PCO2.Denjean et al37 reported a dose-response study in which
they administered 1 or 2 MDI puffs of albuterol via man-ual ventilation over 30 seconds and found that 30 min aftertreatment the total compliance of the respiratory systemhad increased 67% and the total resistance of the respira-tory system had decreased 33% (Fig. 7).With 8 ventilated infants Pfenninger and Aebi38 found
no difference in patient response between 10 !g/kg ofintravenous albuterol and 200 !g albuterol via MDI/spaceradapter.With 11 ventilated infants Torres et al39 compared de-
livery of albuterol via hand ventilation with nebulizer (1.5mg in 3mL saline) and viaMDI/chamber (360!g). Changein total resistance and total compliance of the respiratorysystem persisted for 2 hours after administration, but not at4 hours, and there was no difference between the methods(Fig. 8).Fok et al40 compared administration of 200 !g of albu-
terol from an MDI/Aerochamber (with valve removed), aSiemens ultrasonic nebulizer, and 2 jet nebulizers (Side-Stream and Hudson) operated at 6 L/min. The MDI andultrasonic nebulizer provided greater reductions in totalresistance of the respiratory system than did either jet neb-ulizer. The ultrasonic nebulizer trended toward a greaterbronchodilator effect than the MDI (Fig. 9).Sivakumar et al41 obtained similar results in premature
infants who required ventilation after 7 days of age. Al-buterol via MDI/spacer increased passive respiratory sys-tem compliance more than did albuterol via low-flow neb-ulizer (34% vs 11%, p ! 0.02).Holt et al42 demonstrated the use of flow-volume loops
and lung function testing to differentiate infants’ responseto bronchodilators during mechanical ventilation (Fig. 10).
Inhaled Steroids
Arnon et al43 evaluated the effects of 600 !g of inhaledbudesonide via nebulizer (twice a day) in ventilator-de-pendent preterm infants at 14 days of age. The steroid-treated infants required lower airway pressures and lowerinspired oxygen concentration than did the control infantsafter 4 days of therapy (Fig. 11). However, there was no
Fig. 10. Tidal flow-volume loops based on mechanical breaths inan infant with a positive response to inhaled bronchodilators (A)before (ie, at baseline) and (B) 20 min after administration. (FromReference 42, with permission.)
AEROSOL DELIVERY TO VENTILATED INFANT AND PEDIATRIC PATIENTS
662 RESPIRATORY CARE • JUNE 2004 VOL 49 NO 6
delivery was shorter with the Aeroneb Pro (2 min) thanwith the Mistyneb (10 min) (p ! 0.001). The efficiency ofthe jet nebulizer was consistent with other animal modelsand in vivo infant studies, but deposition with the AeronebPro was greater than previously reported from a nebulizerin infant ventilation.
Outcome Studies in Ventilated Infants
The relatively low efficiency of aerosol deposition dur-ing infant ventilation may be misleading, in that a small
absolute lung dose provides a larger dose/kg of bodyweightthan in adults. It is more clinically relevant to evaluate thephysiological effect of a pharmacologic aerosol than todwell on scant deposition data.
Bronchodilators
Rotschild et al36 studied 20 ventilator-dependent infants(weighing! 1,500 g) and found that 2.5 mg of aerosolizedalbuterol improved static compliance significantly morethan placebo and decreased PCO2.Denjean et al37 reported a dose-response study in which
they administered 1 or 2 MDI puffs of albuterol via man-ual ventilation over 30 seconds and found that 30 min aftertreatment the total compliance of the respiratory systemhad increased 67% and the total resistance of the respira-tory system had decreased 33% (Fig. 7).With 8 ventilated infants Pfenninger and Aebi38 found
no difference in patient response between 10 !g/kg ofintravenous albuterol and 200 !g albuterol via MDI/spaceradapter.With 11 ventilated infants Torres et al39 compared de-
livery of albuterol via hand ventilation with nebulizer (1.5mg in 3mL saline) and viaMDI/chamber (360!g). Changein total resistance and total compliance of the respiratorysystem persisted for 2 hours after administration, but not at4 hours, and there was no difference between the methods(Fig. 8).Fok et al40 compared administration of 200 !g of albu-
terol from an MDI/Aerochamber (with valve removed), aSiemens ultrasonic nebulizer, and 2 jet nebulizers (Side-Stream and Hudson) operated at 6 L/min. The MDI andultrasonic nebulizer provided greater reductions in totalresistance of the respiratory system than did either jet neb-ulizer. The ultrasonic nebulizer trended toward a greaterbronchodilator effect than the MDI (Fig. 9).Sivakumar et al41 obtained similar results in premature
infants who required ventilation after 7 days of age. Al-buterol via MDI/spacer increased passive respiratory sys-tem compliance more than did albuterol via low-flow neb-ulizer (34% vs 11%, p ! 0.02).Holt et al42 demonstrated the use of flow-volume loops
and lung function testing to differentiate infants’ responseto bronchodilators during mechanical ventilation (Fig. 10).
Inhaled Steroids
Arnon et al43 evaluated the effects of 600 !g of inhaledbudesonide via nebulizer (twice a day) in ventilator-de-pendent preterm infants at 14 days of age. The steroid-treated infants required lower airway pressures and lowerinspired oxygen concentration than did the control infantsafter 4 days of therapy (Fig. 11). However, there was no
Fig. 10. Tidal flow-volume loops based on mechanical breaths inan infant with a positive response to inhaled bronchodilators (A)before (ie, at baseline) and (B) 20 min after administration. (FromReference 42, with permission.)
AEROSOL DELIVERY TO VENTILATED INFANT AND PEDIATRIC PATIENTS
662 RESPIRATORY CARE • JUNE 2004 VOL 49 NO 6
RESPIRATORY CARE • JUNE 2004 VOL 49 NO 6
Aerosol Delivery to Ventilated Infant and Pediatric Patients James B Fink MSc RRT FAARC

CONCLUSIONES
• Manejo controversial en BA
• no RCT
• favorecer técnicas de menor impacto CPT v/s KTR
• optimizar adecuados VP
• imperativo conservar la estabilidad de la VA
• considerar uso de PP
• implementación de protocolos.
• interpretacion de GV en VM.