Embed Size (px)
Citation preview
T i Vi lTropismo Viral
Federico GarcíaFederico GarcíaHU San Cecilio, Granada
Contenidos
Tropismo del VIH: ImportanciaTropismo del VIH: ImportanciaCómo se puede determinar el tropismoControversias en 2009:
Existen alternativas a Trofile?Existen alternativas a Trofile?Que hacer con pacientes con CV Indetectable (simplificación toxicidad )Indetectable (simplificación, toxicidad,...)
Ent ada de VIHEntrada de VIH
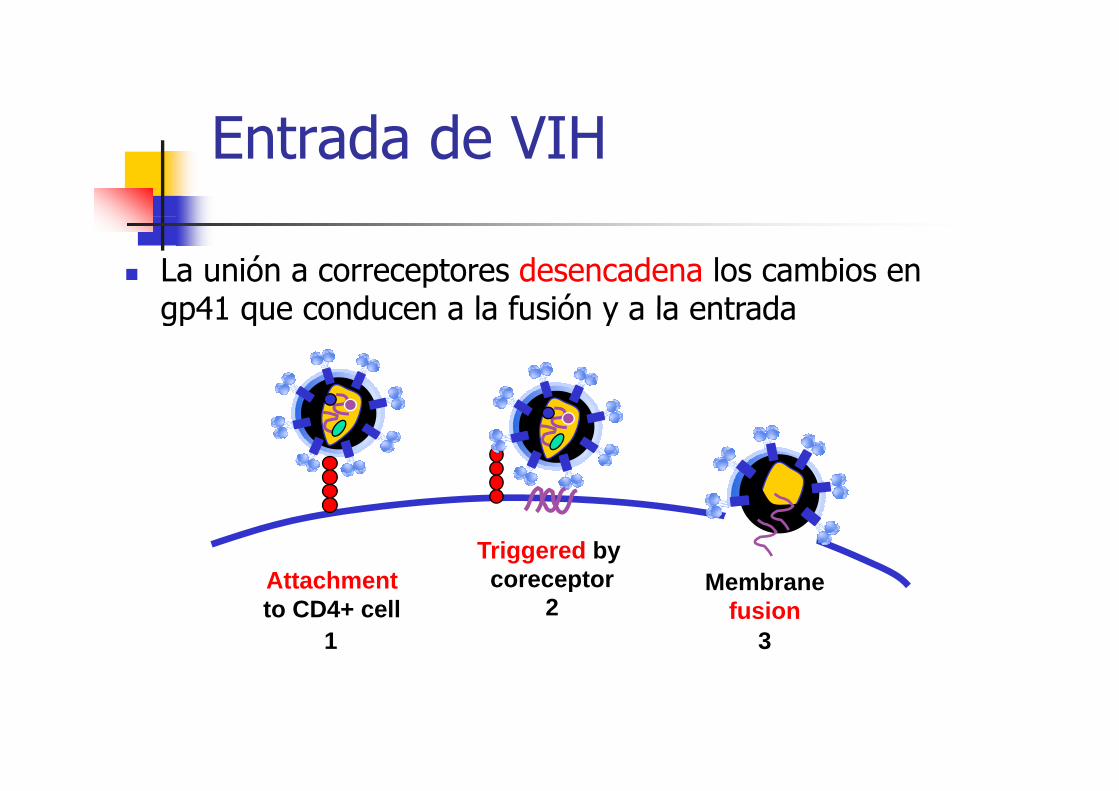
La unión a correceptores desencadena los cambios en gp41 que conducen a la fusión y a la entradagp41 que conducen a la fusión y a la entrada
Att h tTriggered by coreceptor M bAttachment
to CD4+ cellcoreceptor Membrane
fusion1
23
Ti d CTipos de Correceptores
NF G
YS Q Y Q F
WKN
H
PF
EFFGL N N C
SSS
QVNI K Q C
PES
TYYNIDYIPSS V Q Y D M - NH2 CCR5
DW
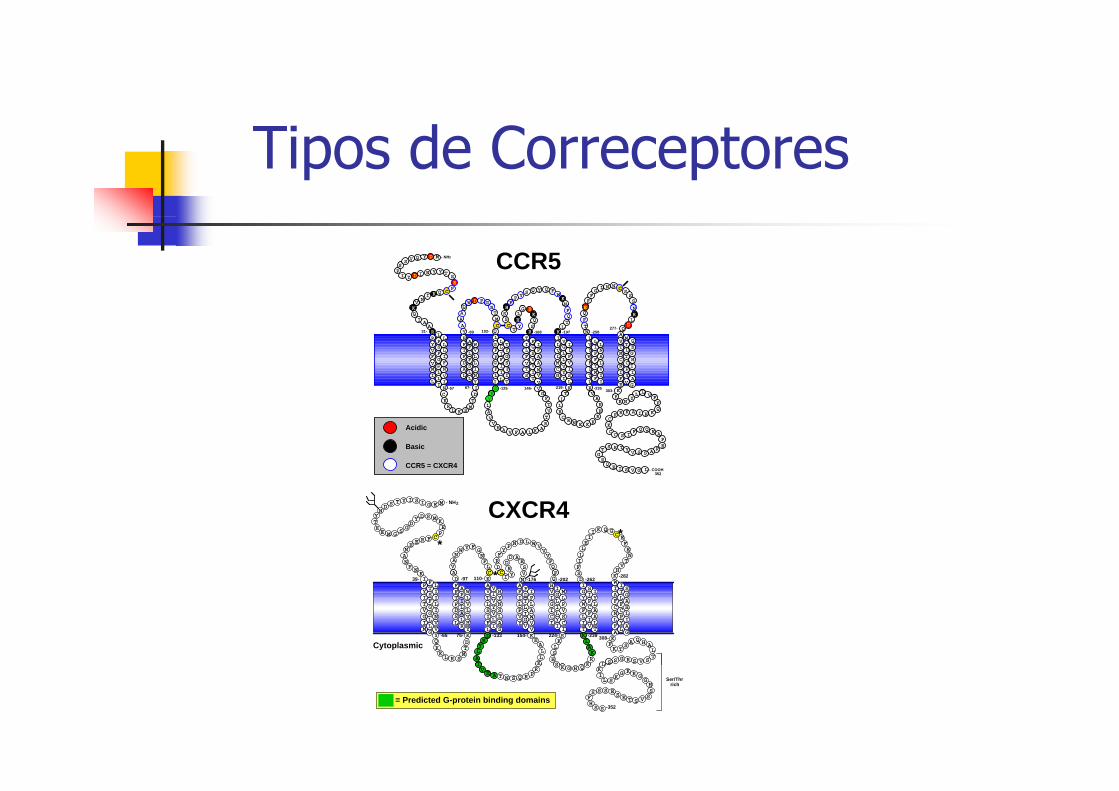
CCR5
C
LAD
TF
F
H
LL
S
PL
A
F
NY
I
VL
W
L
LF
I
G
FG
F
L
IL
I
LI
L
F
IT
F
YG
T
S
STV
LI
F
T
IT
V
GS
F
V
VV
W
PA
I
A
GCM
VL
L
I
YI
V
GL
V
L
SL
I
LP
I
V
TI
L
F
YV
W
L
MF
Y
IP
L
F
II
V
NA
L
LMV
I
F
YP
V
GL
G
L
S
L
F
NV
F
I
L
L
I
LIN
IN
F
C
TV
M
A
PY
C
V
TL
M
T
IA
I
G
EG
Q
H
EID
Y
TMCQ
N
RVG
SQK
EGLHY
TCS
FQ
HS
KT V
NTFQE N
R
DQ
L
KF L L
V
AA
AQ
AAI
QK
R31-
-57 67-
-89 102-
-125 146-
-168 -197
219- -235
-258
303-
TL
R
PL
D
K
R
277-
352
C D
L
KR M
T
K S
YLAVV
A F A K ARTVTF
HV L
LL
HR
KKENRCR
CK
FFR N
YL V
HIAKRF
F
QK
ACC S I
F Q Q
SVYTRS
TG
E
PE
RASEQE - COOH
RA
I S V G L
Acidic
Basic
CCR5 = CXCR4
FLC
N
Y FG
VSE
ADDRYI
CD
N D L W VVVFQF
F
PY
R
SFILLEII K Q G
C EFENT
HK
VVA
ANW
KNF
NANE E R F C
PEKM
SDYD
GSGME
ETYND S T Y I S I G E M - NH2
*
*
*
282
CXCR-4CXCR4
Q
LSD
TF
F
LR
A
PI
A
L
HY
V
LV
W
L
FI
L
S
TV
L
A
LI
V
IV
V
Y
AS
L
YN
H
S
YVP
IF
L
A
GV
I
DT
F
L
VV
W
PL
I
A
ICI
IV
G
H
YI
L
GL
I
I
CI
S
LP
M
V
IL
T
F
YG
W
I
IV
F
IP
S
C
LT
A
YL
I
AGV
I
T
YP
I
I
GL
G
L
TS
F
F
NV
I
V
II
L
L
M G Y
LN
F
C
AI
F
W
PY
C
L
TL
I
F
IA
L
G
GA
S
H
AKD
L
KK M
T
R S
D K
DRYLAI K
LLA
KE
VYI Q
SKLS
KLAKRKS
H
DS K
L
K
LFK T
SA Q H
VSRGSS
A
TS
KN
Cytoplasmic
39-
-65 75-
-97 110-
-133 154-
-176 -202
224- -239
-262-282
308-
F
IV
N S R PR
HT Q
KQHGKS LK
GIL S
KG K R
TESESSS
F
G
HSSVSH
S S
Ser/Thr rich
-352
A
= Predicted G-protein binding domains
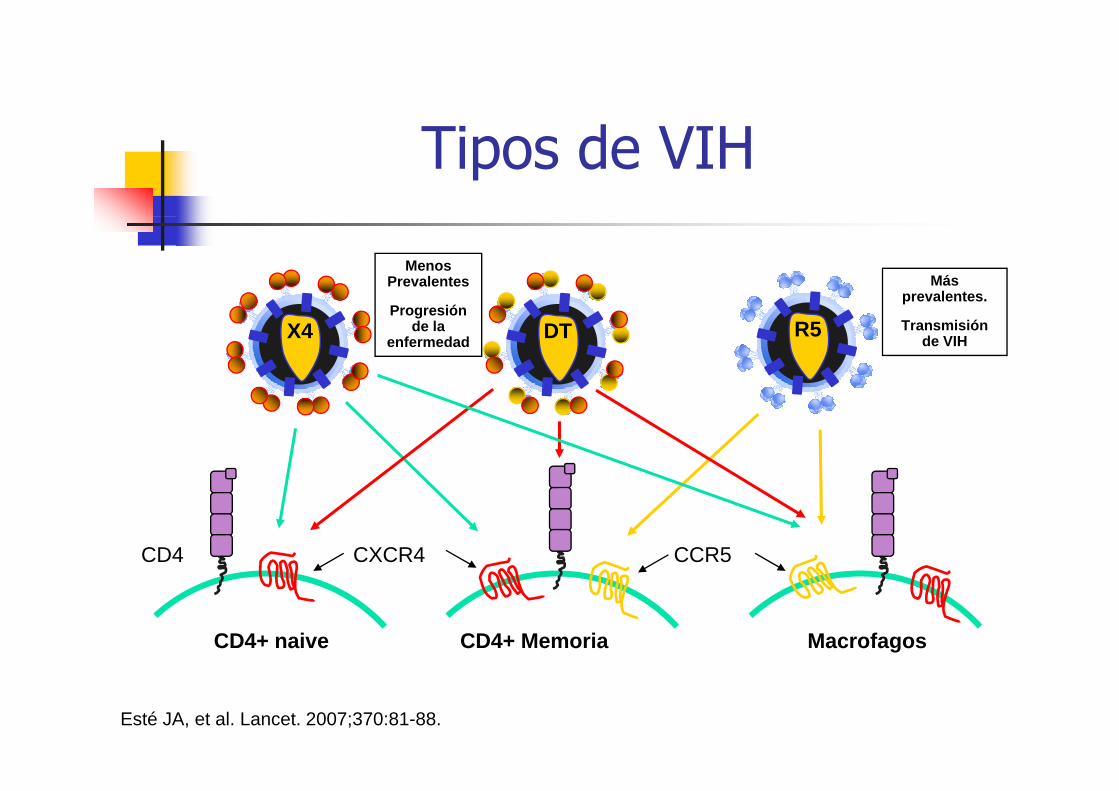
Ti d VIHTipos de VIH
Menos Prevalentes
P ió
Más prevalentes.
R5X4 DTProgresión
de la enfermedad
Transmisión de VIH
CXCR4 CCR5CD4
CD4+ naive CD4+ Memoria Macrofagos
Esté JA, et al. Lancet. 2007;370:81-88.
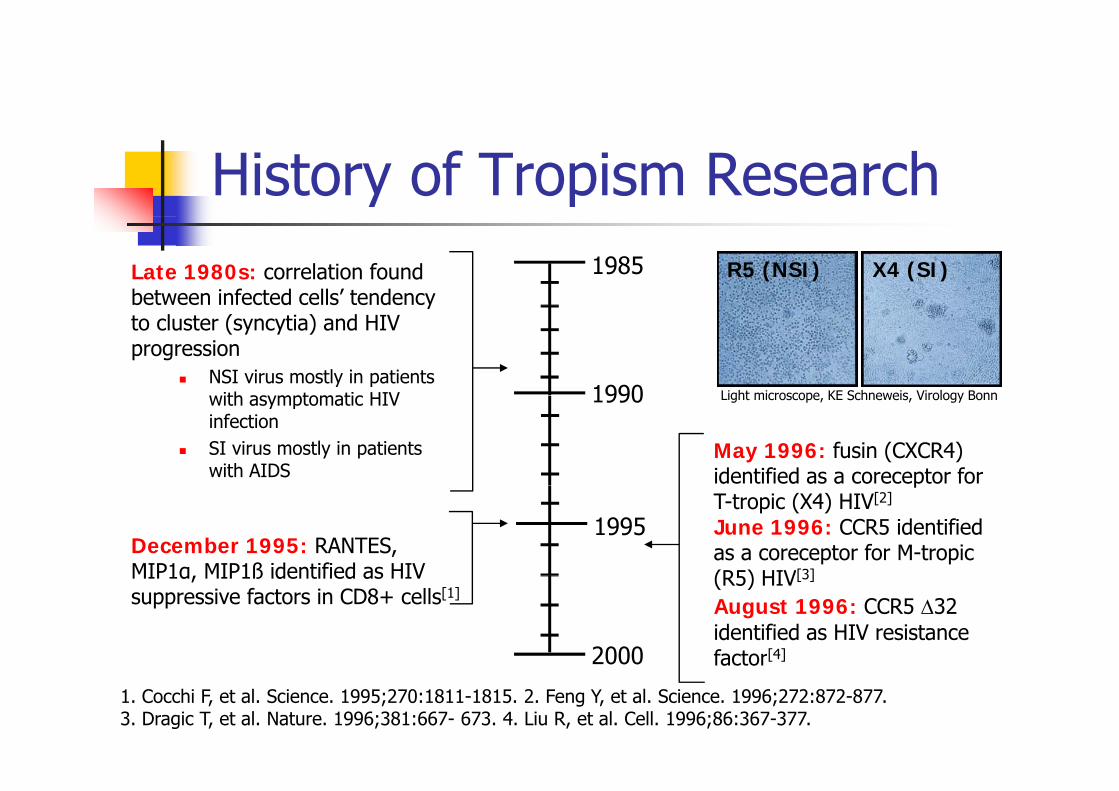
History of Tropism ResearchLate 1980s: correlation found between infected cells’ tendency
1985 R5 (NSI) X4 (SI)y
to cluster (syncytia) and HIV progression
NSI virus mostly in patients with asymptomatic HIV 1990 Light microscope KE Schneweis Virology Bonnwith asymptomatic HIV infectionSI virus mostly in patients with AIDS
1990
May 1996: fusin (CXCR4) identified as a coreceptor for
Light microscope, KE Schneweis, Virology Bonn
December 1995: RANTES, MIP1α MIP1ß identified as HIV
pT-tropic (X4) HIV[2]
June 1996: CCR5 identified as a coreceptor for M-tropic (R5) HIV[3]
1995
2000
MIP1α, MIP1ß identified as HIV suppressive factors in CD8+ cells[1]
(R5) HIV[3]
August 1996: CCR5 ∆32identified as HIV resistance factor[4]
1. Cocchi F, et al. Science. 1995;270:1811-1815. 2. Feng Y, et al. Science. 1996;272:872-877. 3. Dragic T, et al. Nature. 1996;381:667- 673. 4. Liu R, et al. Cell. 1996;86:367-377.
factor
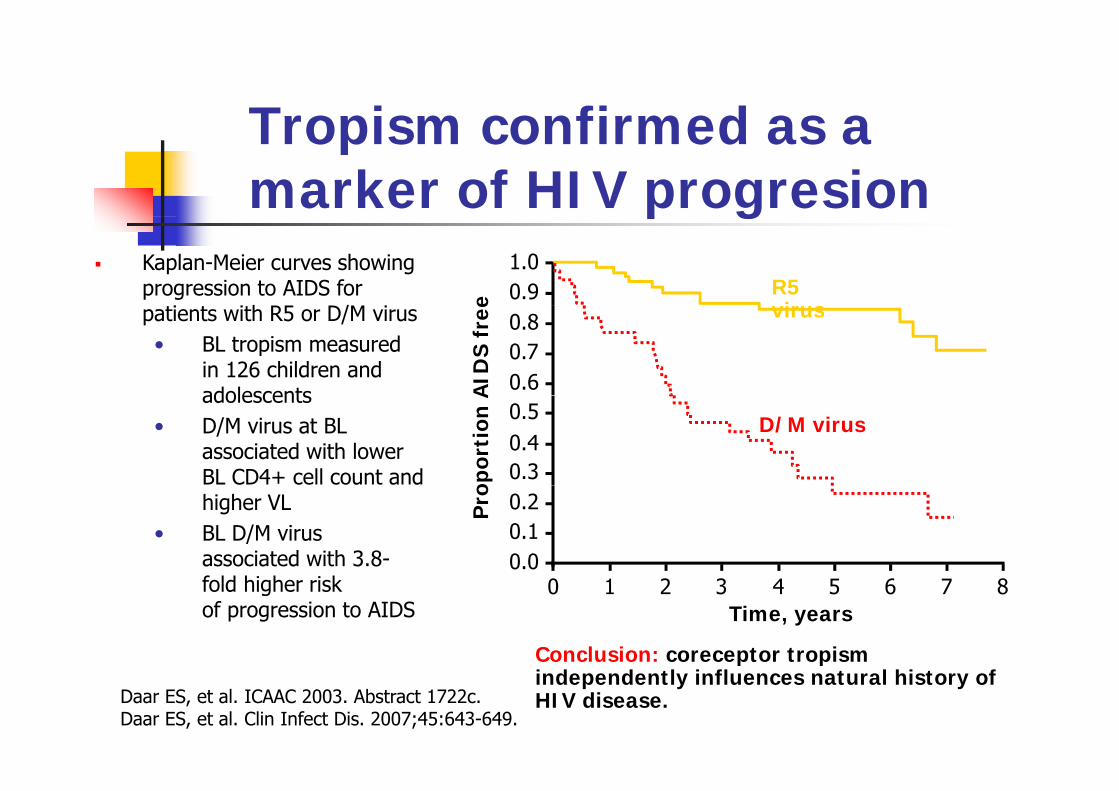
Tropism confirmed as aTropism confirmed as a marker of HIV progresionp g
Kaplan-Meier curves showing progression to AIDS for
i i h R5 D/M iR5 virus
0.91.0
e
0.6
patients with R5 or D/M virus• BL tropism measured
in 126 children and adolescents
virus
0.70.8
AID
S fr
ee
0.40.5
adolescents• D/M virus at BL
associated with lower BL CD4+ cell count and
D/M virus
0.3op
orti
on A
higher VL• BL D/M virus
associated with 3.8- 0.00.10.2P
ro
fold higher risk of progression to AIDS
0 1 2 3 4 5 6 7 8Time, years
Conclusion: coreceptor tropism
Daar ES, et al. ICAAC 2003. Abstract 1722c.Daar ES, et al. Clin Infect Dis. 2007;45:643-649.
p pindependently influences natural history of HIV disease.
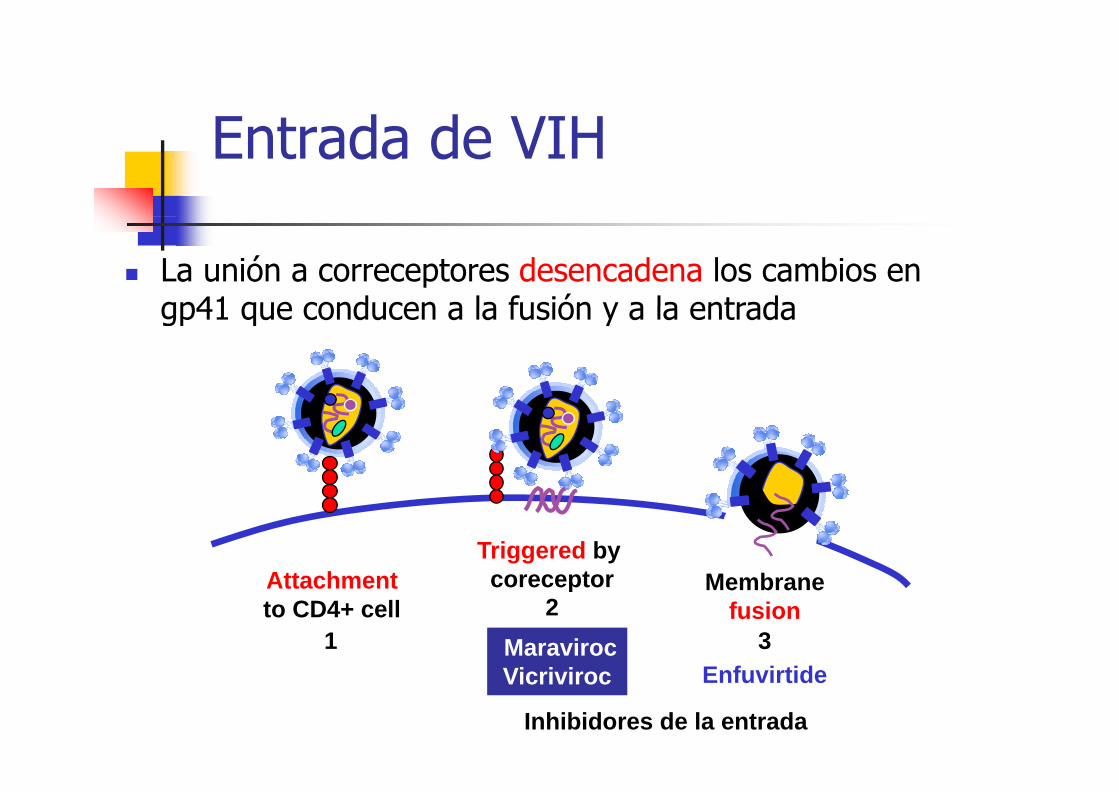
Ent ada de VIHEntrada de VIH
La unión a correceptores desencadena los cambios en gp41 que conducen a la fusión y a la entradagp41 que conducen a la fusión y a la entrada
Att h tTriggered by coreceptor M bAttachment
to CD4+ cellcoreceptor Membrane
fusion1
23Maraviroc
Vicriviroc Enfuvirtide
Inhibidores de la entrada
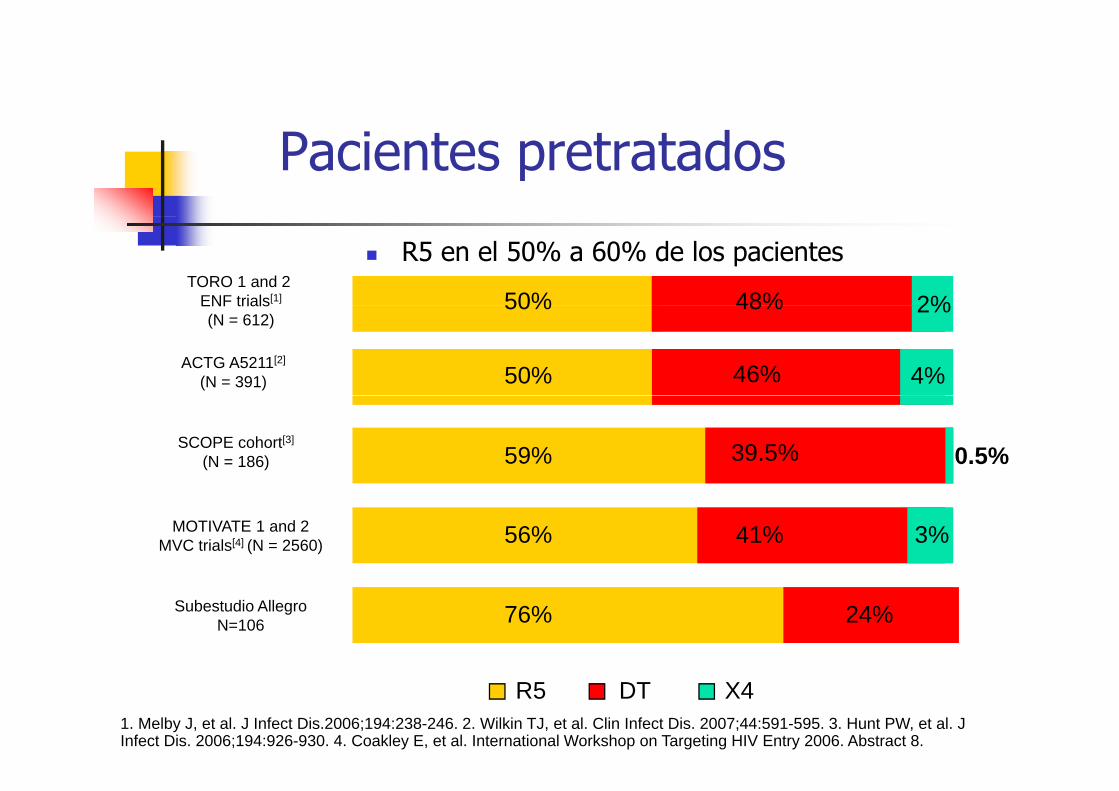
Pacientes pretratados
50%TORO 1 and 2
ENF trials[1] 48% 2%
R5 en el 50% a 60% de los pacientes
50%
50%
ENF trials(N = 612)
ACTG A5211[2]
(N = 391)
48%
46% 4%
2%
59%SCOPE cohort[3]
(N = 186) 39.5% 0.5%
56% 41%MOTIVATE 1 and 2 MVC trials[4] (N = 2560) 3%
76% 24%Subestudio AllegroN=106
1. Melby J, et al. J Infect Dis.2006;194:238-246. 2. Wilkin TJ, et al. Clin Infect Dis. 2007;44:591-595. 3. Hunt PW, et al. J Infect Dis. 2006;194:926-930. 4. Coakley E, et al. International Workshop on Targeting HIV Entry 2006. Abstract 8.
R5 DT X4
Contenidos
Tropismo del VIH: ImportanciaTropismo del VIH: ImportanciaCómo se puede determinar el tropismoControversias en 2009:
Existen alternativas a Trofile?Existen alternativas a Trofile?Que hacer con pacientes con CV Indetectable (simplificación toxicidad )Indetectable (simplificación, toxicidad,...)
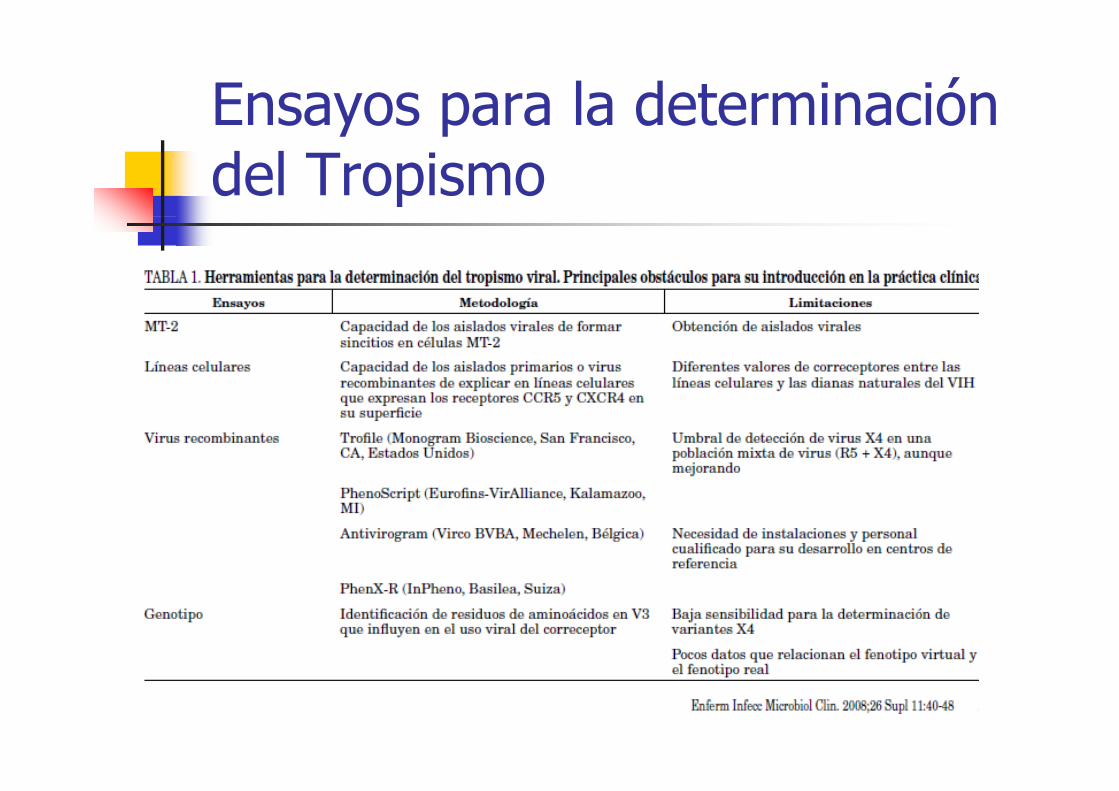
Ensayos para la determinación y pdel Tropismo
Ensayos para la determinación y pdel Tropismo
Fenotipo:Enhanced Sensitivity Trofile Assay (ESTA)TropiTest (ISCIII)TropiTest (ISCIII)
Genotipo:Secuenciación de V3:
Secuenciación de poblacionesSecuenciación masiva de genomas (UDS)
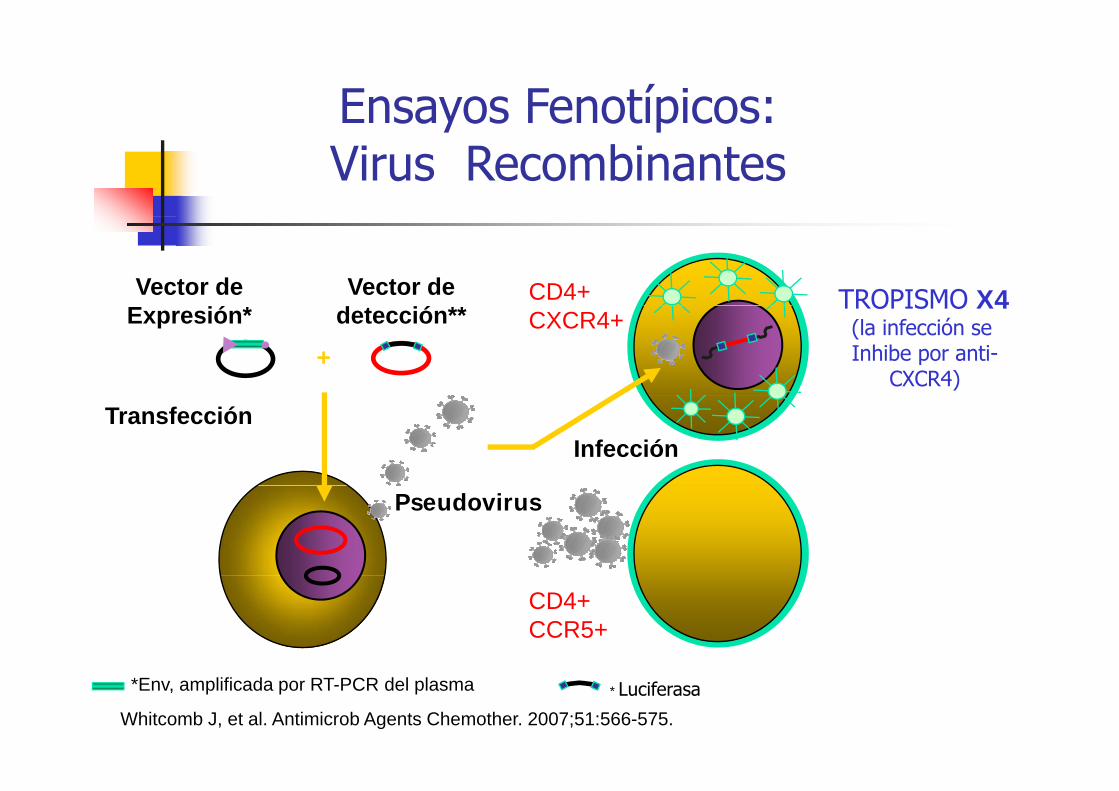
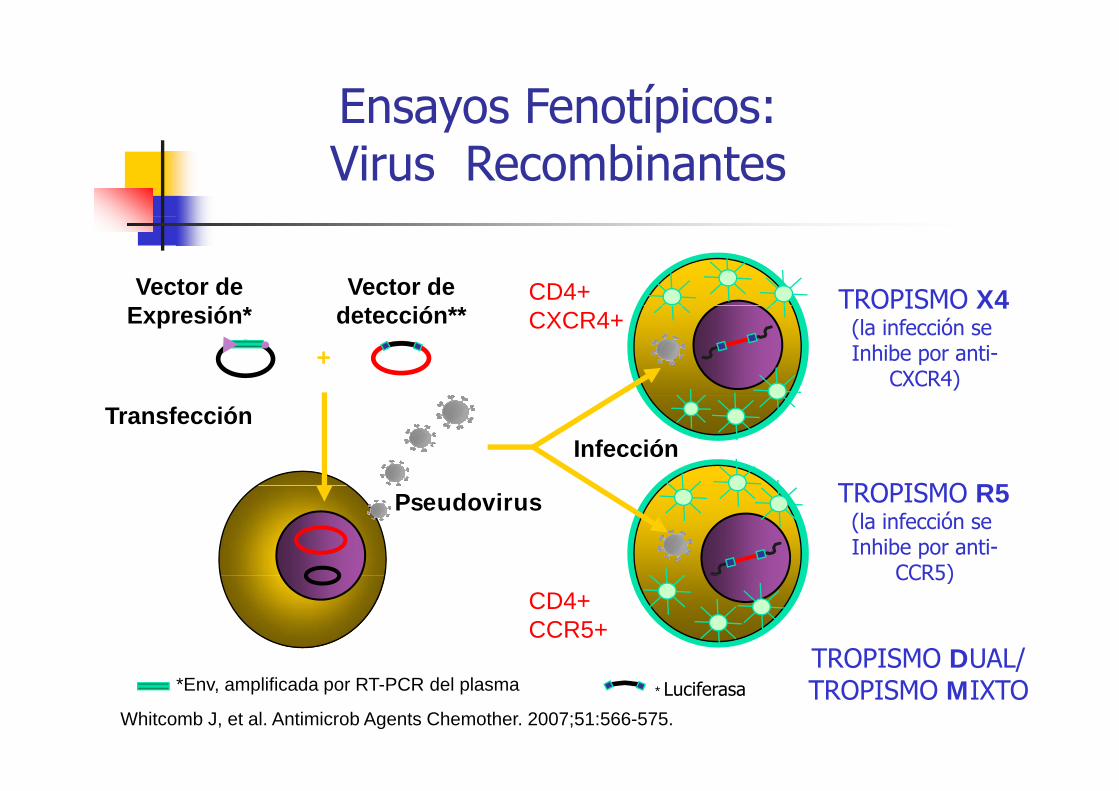
Ensayos Fenotípicos: y pVirus Recombinantes
CD4+Vector de Vector de TROPISMO X4CXCR4+
++++
detección**Expresión* TROPISMO X4(la infección se Inhibe por anti-
CXCR4)
InfecciónTransfección
Pseudovirus
CD4+CCR5+
*Env, amplificada por RT-PCR del plasma
Whitcomb J, et al. Antimicrob Agents Chemother. 2007;51:566-575.* Luciferasa
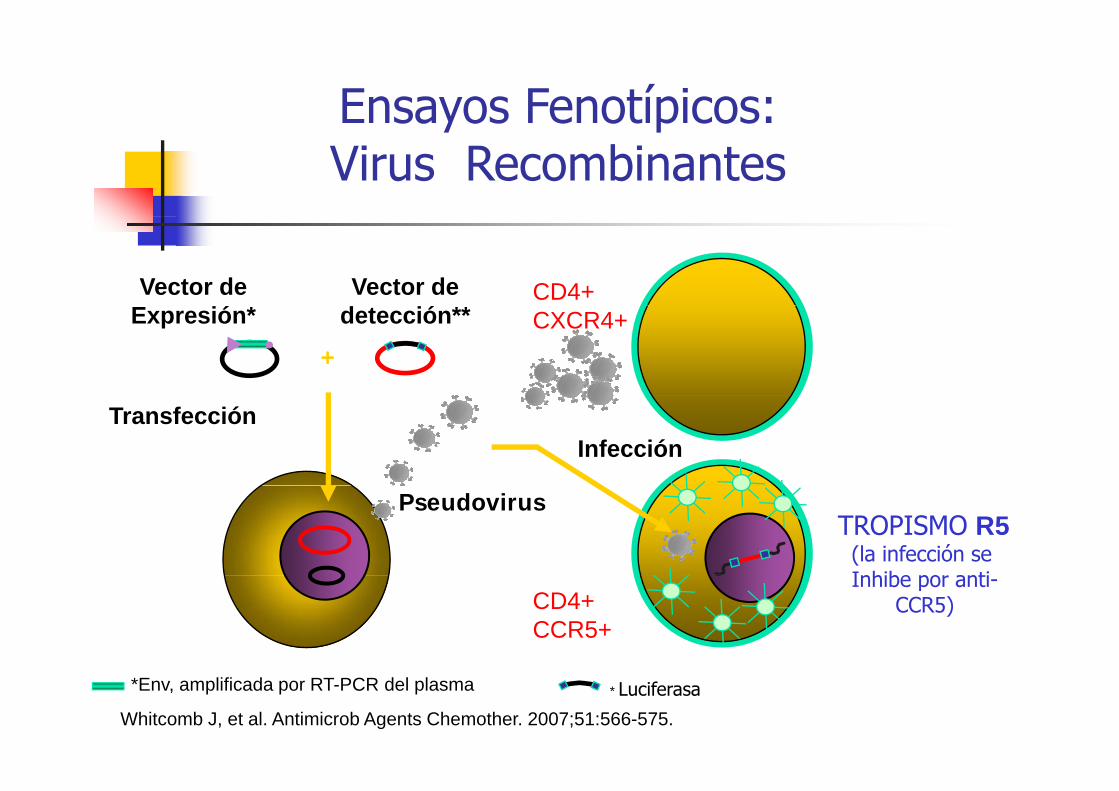
Ensayos Fenotípicos: y pVirus Recombinantes
CD4+Vector de Vector de CXCR4+
++++
detección**Expresión*
InfecciónTransfección
PseudovirusTROPISMO R5
(la infección se Inhibe po anti
CD4+CCR5+
Inhibe por anti-CCR5)
*Env, amplificada por RT-PCR del plasma
Whitcomb J, et al. Antimicrob Agents Chemother. 2007;51:566-575.* Luciferasa
Ensayos Fenotípicos: y pVirus Recombinantes
CD4+Vector de Vector de TROPISMO X4CXCR4+
++++
detección**Expresión* TROPISMO X4(la infección se Inhibe por anti-
CXCR4)
InfecciónTransfección
TROPISMO R5Pseudovirus TROPISMO R5(la infección se Inhibe por anti-
CCR5)CD4+CCR5+
CCR5)
TROPISMO DUAL/*Env, amplificada por RT-PCR del plasma
Whitcomb J, et al. Antimicrob Agents Chemother. 2007;51:566-575.* Luciferasa
TROPISMO DUAL/TROPISMO MIXTO
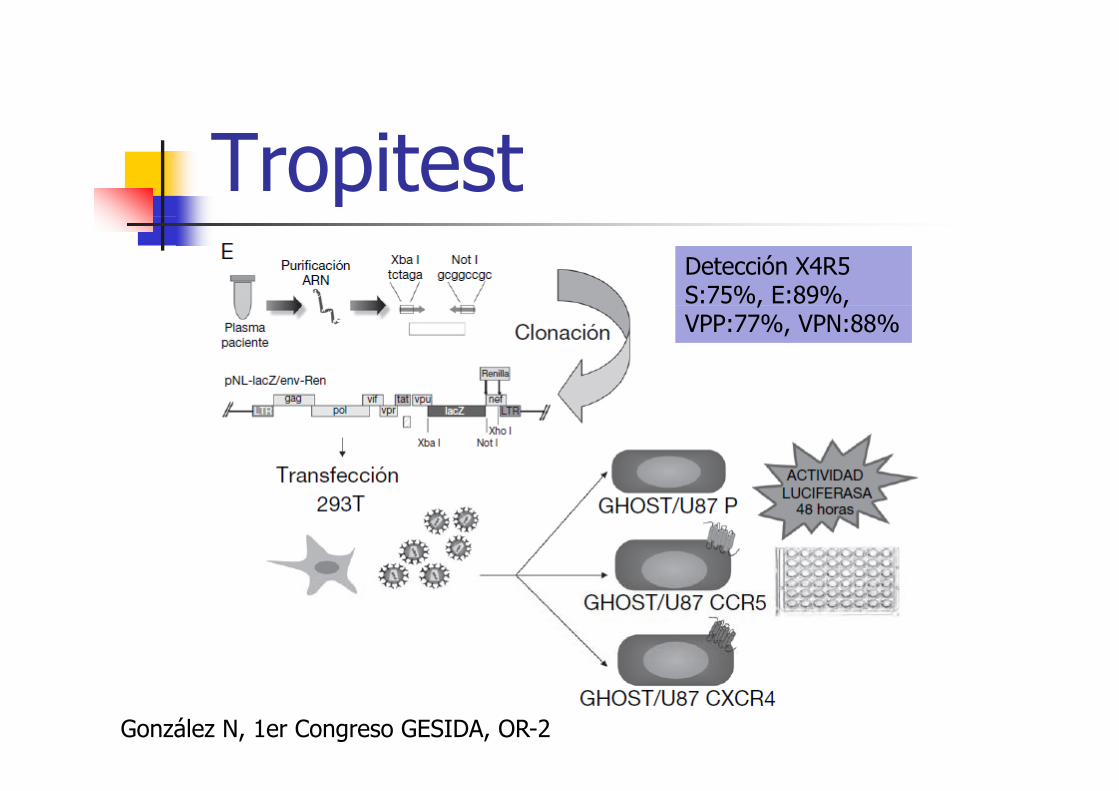
TropitestDetección X4R5S:75%, E:89%, , ,VPP:77%, VPN:88%
González N, 1er Congreso GESIDA, OR-2
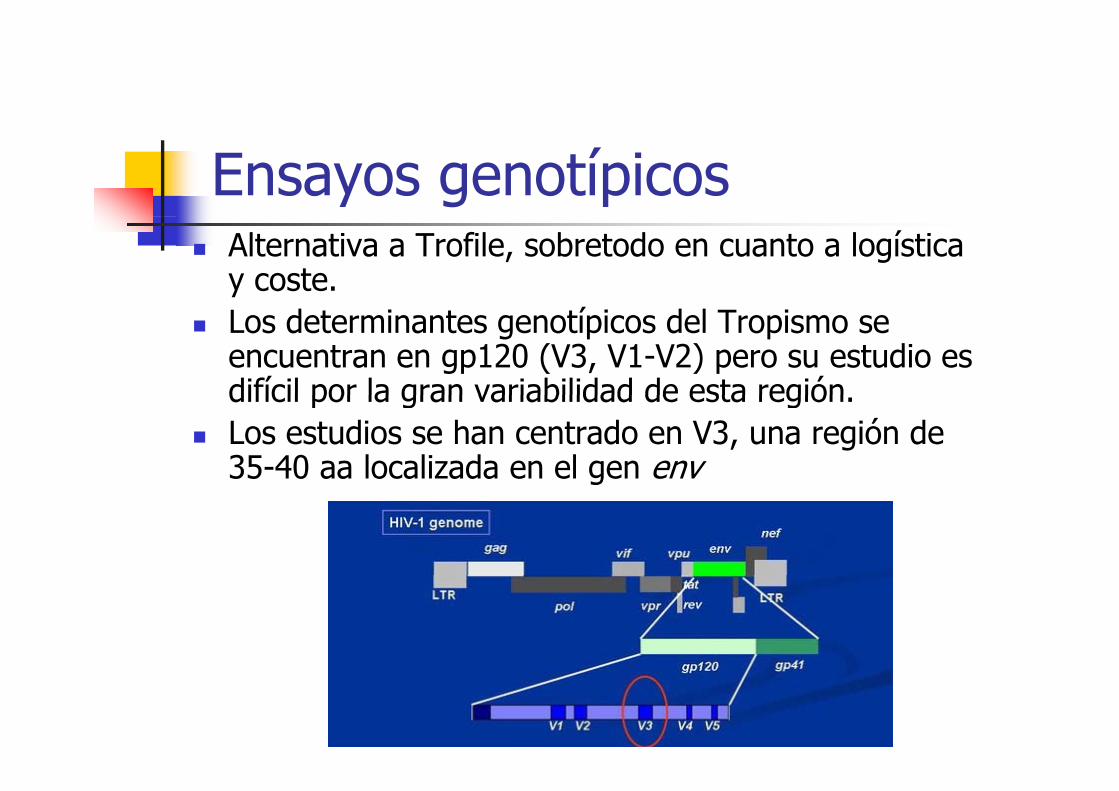
Ensayos genotípicosAlternativa a Trofile, sobretodo en cuanto a logística y coste.Los determinantes genotípicos del Tropismo se encuentran en gp120 (V3, V1-V2) pero su estudio es difícil por la gran variabilidad de esta regióndifícil por la gran variabilidad de esta región.Los estudios se han centrado en V3, una región de 35-40 aa localizada en el gen env
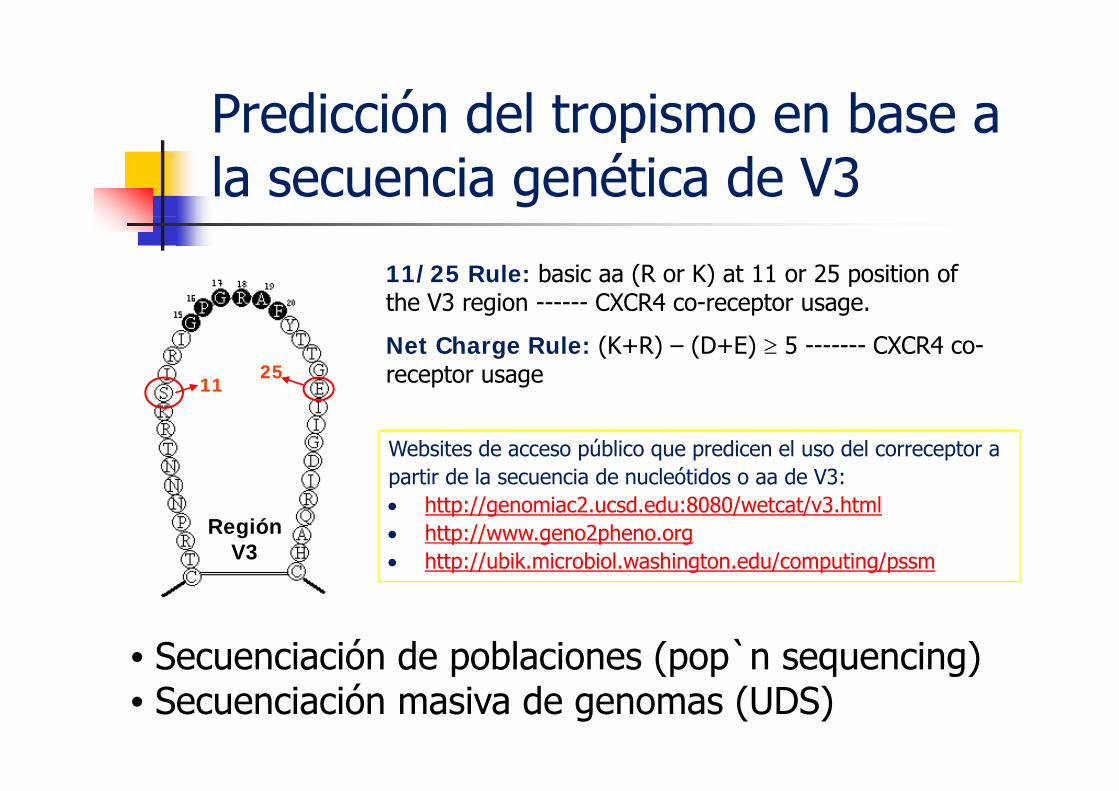
Predicción del tropismo en base aPredicción del tropismo en base a la secuencia genética de V3
11/25 Rule: basic aa (R or K) at 11 or 25 position of the V3 region ------ CXCR4 co-receptor usagethe V3 region CXCR4 co receptor usage.
Net Charge Rule: (K+R) – (D+E) ≥ 5 ------- CXCR4 co-receptor usage11
25
Websites de acceso público que predicen el uso del correceptor a partir de la secuencia de nucleótidos o aa de V3:p• http://genomiac2.ucsd.edu:8080/wetcat/v3.html• http://www.geno2pheno.org• http://ubik.microbiol.washington.edu/computing/pssm
Región V3
• Secuenciación de poblaciones (pop`n sequencing)Secuenciación de poblaciones (pop n sequencing)• Secuenciación masiva de genomas (UDS)
Contenidos
Tropismo del VIH: ImportanciaTropismo del VIH: ImportanciaCómo se puede determinar el tropismoControversias en 2009:
Existen alternativas a Trofile?Existen alternativas a Trofile?Que hacer con pacientes con CV Indetectable (simplificación toxicidad )Indetectable (simplificación, toxicidad,...)
Therapy outcomes of casesreclassified as D/M by ESTAreclassified as D/M by ESTA
(N= 48)
N t ll ti t ith D/M b ESTA f il d!Not all patients with D/M by ESTA failed!
At 48 weeks 45 % had HIV RNA < 50 copies
no quantitative data on proportion of X4 are available
Swenson et al, CROI 2009, Abstract 680
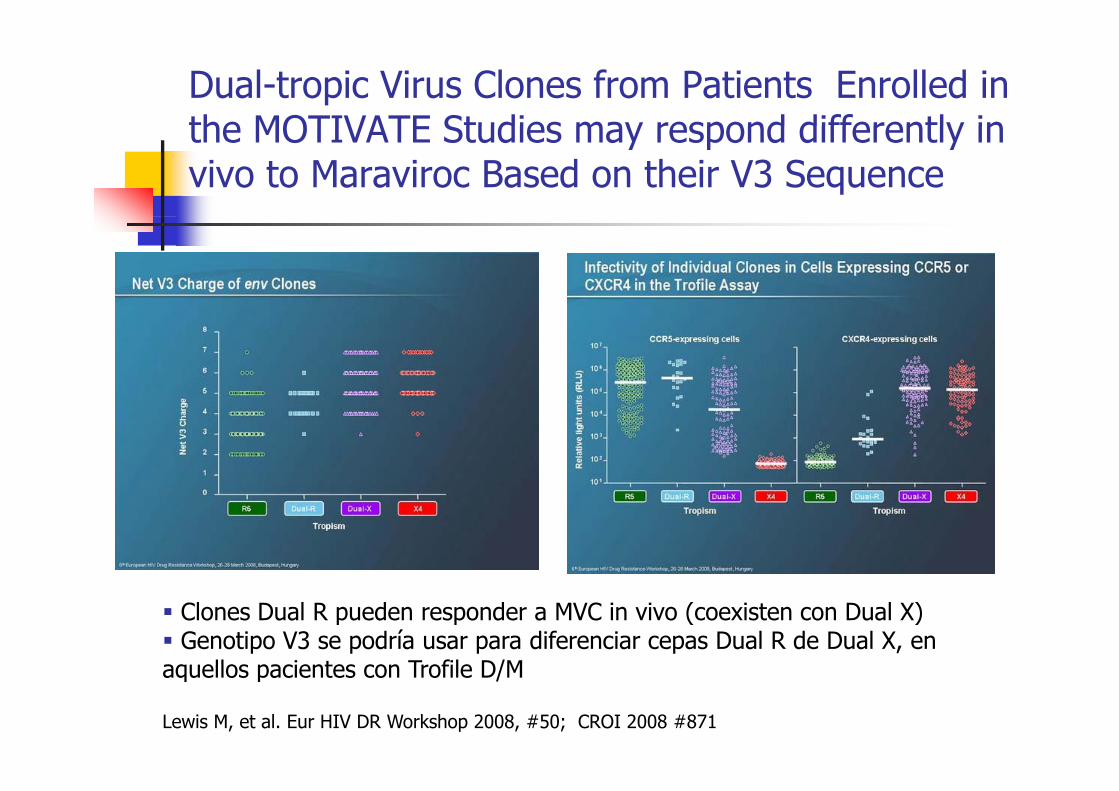
Dual-tropic Virus Clones from Patients Enrolled in the MOTIVATE Studies may respond differently inthe MOTIVATE Studies may respond differently in vivo to Maraviroc Based on their V3 Sequence
Clones Dual R pueden responder a MVC in vivo (coexisten con Dual X) Genotipo V3 se podría usar para diferenciar cepas Dual R de Dual X, en
aquellos pacientes con Trofile D/M
Lewis M, et al. Eur HIV DR Workshop 2008, #50; CROI 2008 #871
aquellos pacientes con Trofile D/M
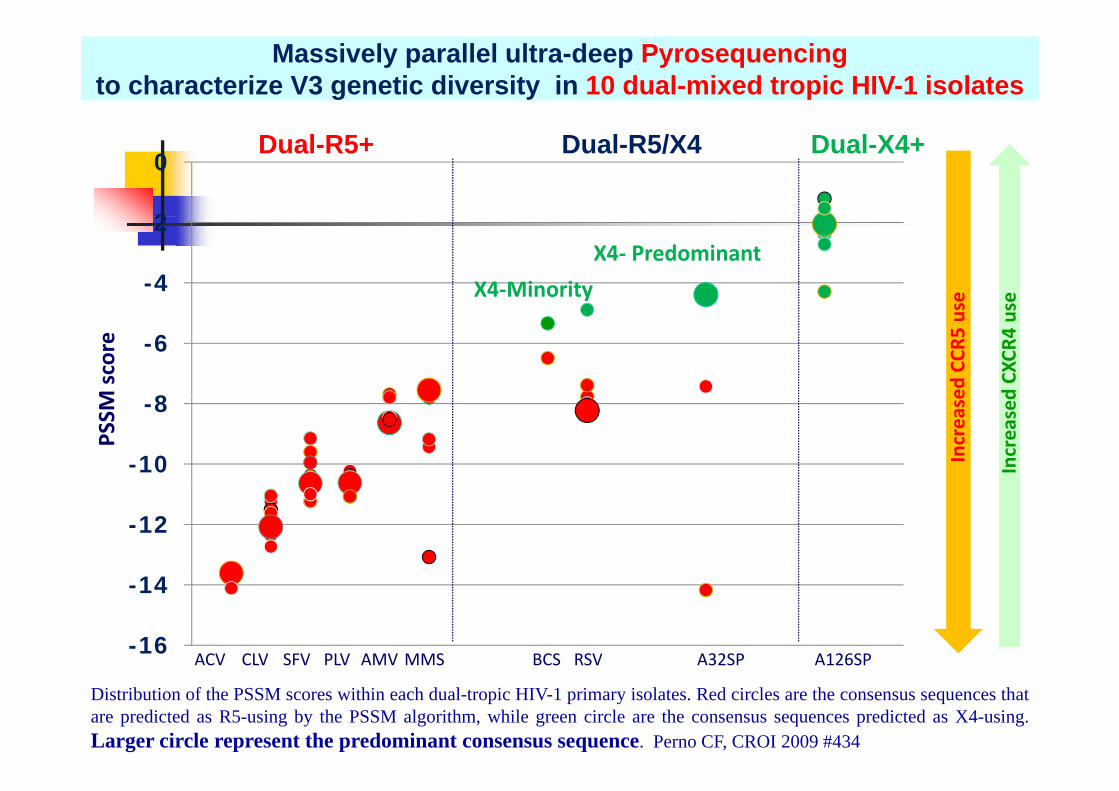
Massively parallel ultra-deep Pyrosequencingto characterize V3 genetic diversity in 10 dual-mixed tropic HIV-1 isolates
2
0Dual-R5+ Dual-X4+Dual-R5/X4
-4
-2
X4‐Minority
X4‐ Predominant
se se
8
-6
M score
ed CCR
5 us
d CX
CR4 us
-10
-8
PSSM
Increase
Increased
-12
-16
-14
ACV CLV SFV PLV AMV MMS BCS RSV A32SP A126SPACV CLV SFV PLV AMV MMS BCS RSV A32SP A126SP
Distribution of the PSSM scores within each dual-tropic HIV-1 primary isolates. Red circles are the consensus sequences thatare predicted as R5-using by the PSSM algorithm, while green circle are the consensus sequences predicted as X4-using.Larger circle represent the predominant consensus sequence. Perno CF, CROI 2009 #434
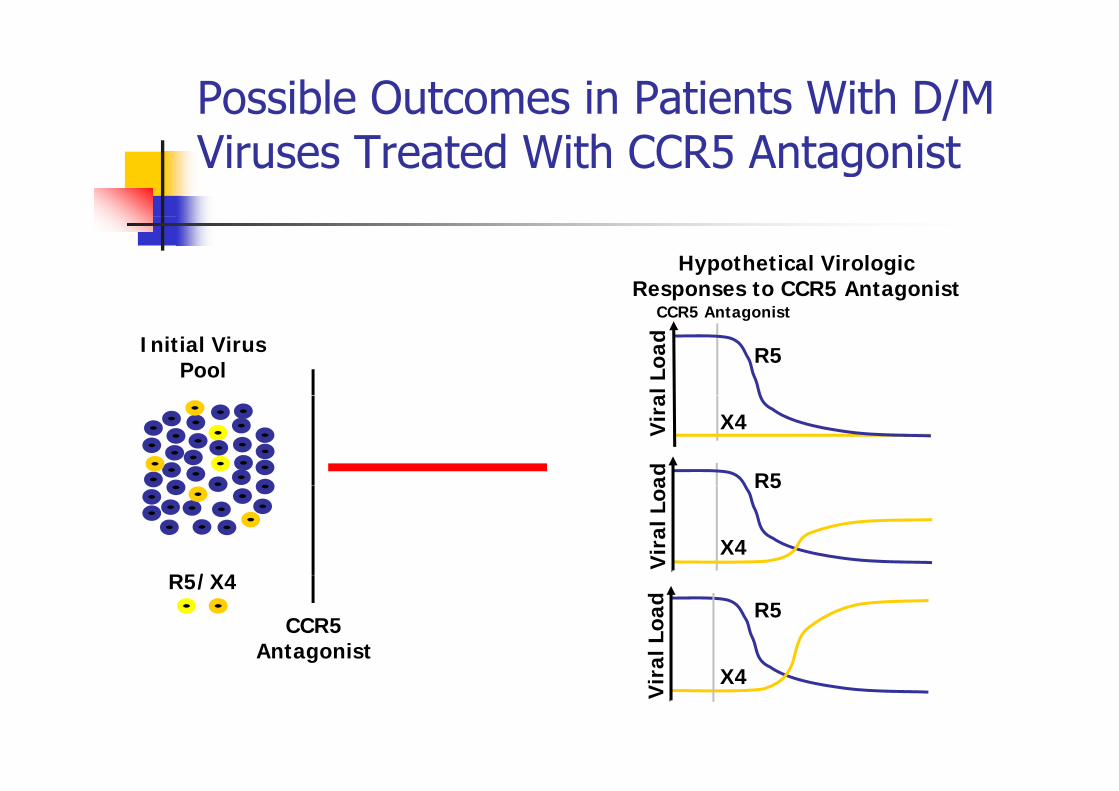
Possible Outcomes in Patients With D/M Viruses Treated With CCR5 Antagonist
Hypothetical Virologic Responses to CCR5 Antagonist
CC i
Initial Virus Pool
al L
oad
R5
CCR5 Antagonist
Vir
a
X4
ad R5
R5/X4
Vir
al L
oa
R5
X4
R5/X4
CCR5Antagonist al
Loa
d R5
Vir
aX4
ConclusionsLevel III Expert opinion: Of the available
ESTA h f d ll iassays, ESTA has performed well in predicting activity of CCR5-antagonists in
ti t ith R5 ltpatients with an R5 resultLevel III Expert opinion: However, use of this assay may exclude a number of experienced patients with low level X4 who could benefit from CCR5 antagonist treatment
Clinical management of HIV-1 tropism testing: development of European guidelines 7th Eur DRW, 2009
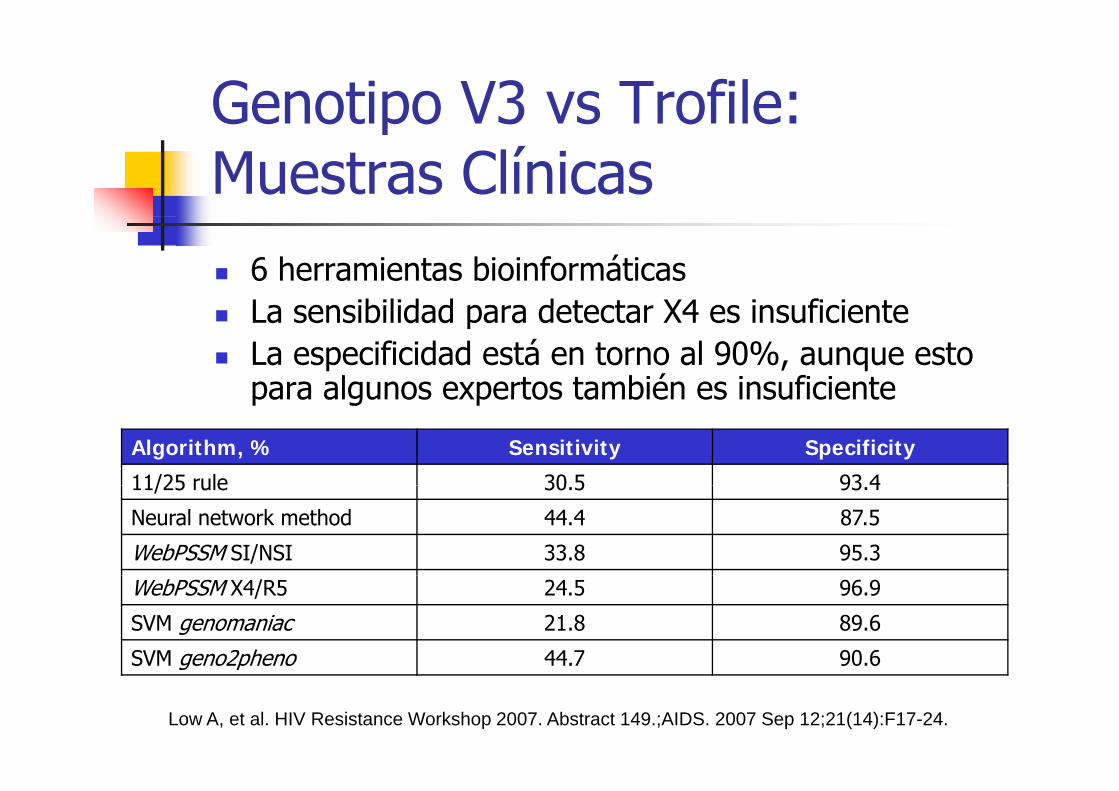
Genotipo V3 vs Trofile: pMuestras Clínicas
6 herramientas bioinformáticasLa sensibilidad para detectar X4 es insuficienteLa sensibilidad para detectar X4 es insuficiente La especificidad está en torno al 90%, aunque esto para algunos expertos también es insuficiente
Algorithm, % Sensitivity Specificity
11/25 rule 30 5 93 4
para algunos expertos también es insuficiente
11/25 rule 30.5 93.4
Neural network method 44.4 87.5
WebPSSM SI/NSI 33.8 95.3
WebPSSM X4/R5 24.5 96.9
SVM genomaniac 21.8 89.6
SVM geno2pheno 44.7 90.6SVM geno2pheno 44.7 90.6
Low A, et al. HIV Resistance Workshop 2007. Abstract 149.;AIDS. 2007 Sep 12;21(14):F17-24.
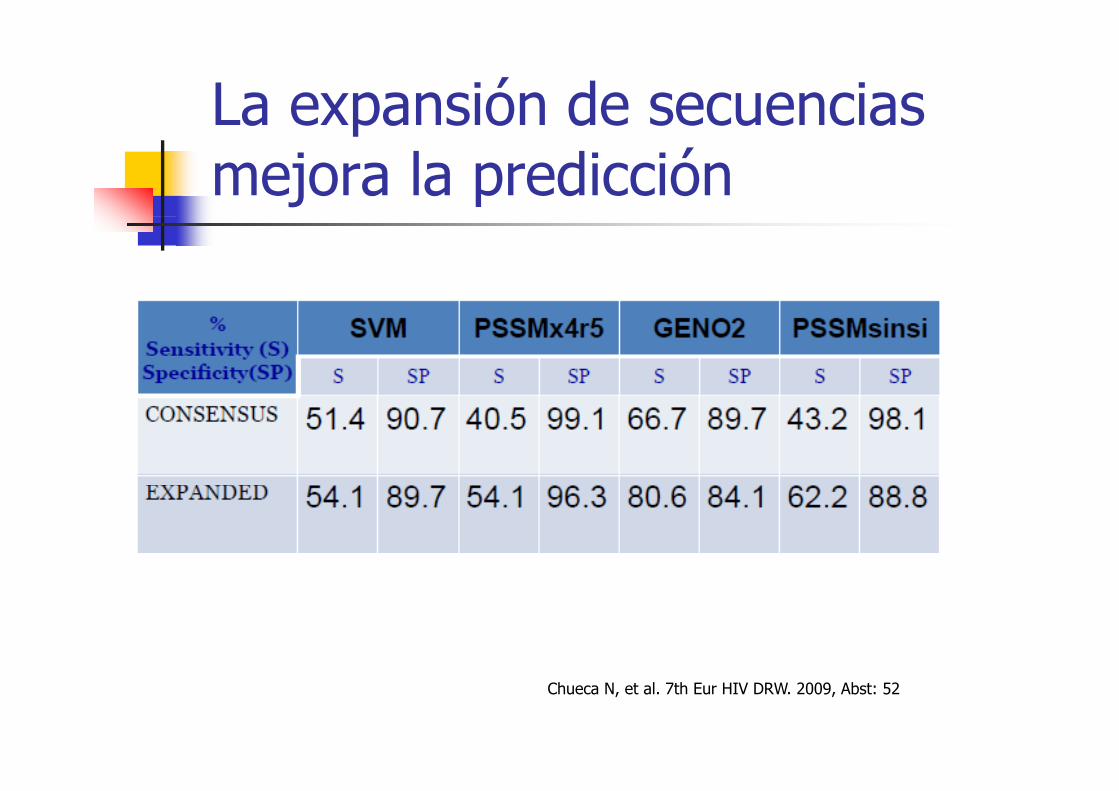
La expansión de secuencias pmejora la predicción
Chueca N, et al. 7th Eur HIV DRW. 2009, Abst: 52
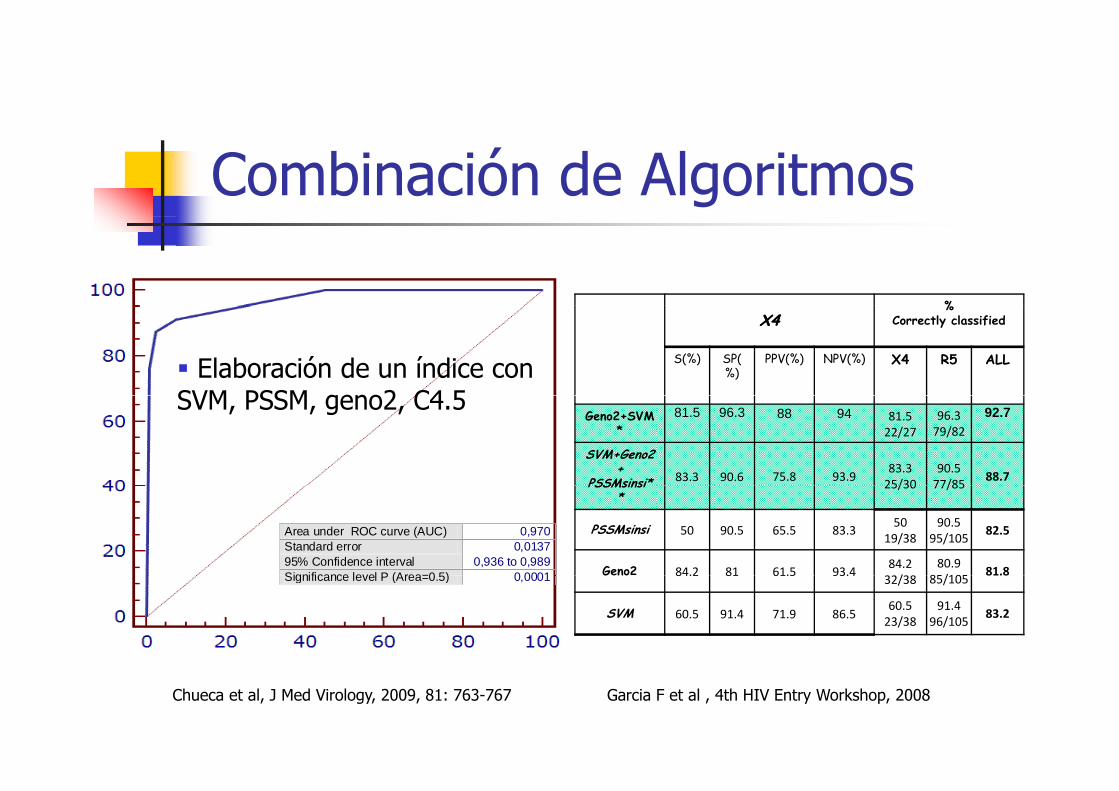
Combinación de Algoritmos
%
Elaboración de un índice con SVM PSSM geno2 C4 5
X4X4%
Correctly classified
S(%) SP(%)
PPV(%) NPV(%) X4 R5 ALL
SVM, PSSM, geno2, C4.5Geno2+SVM
*81.5 96.3 88 94 81.5
22/2796.379/82
92.7
SVM+Geno2+
PSSMsinsi* 83.3 90.6 75.8 93.983.325/30
90.577/85
88.7
Area under ROC curve (AUC) 0,970Standard error 0,013795% Confidence interval 0,936 to 0,989Significance level P (Area=0 5) 0 0001
PSSMsinsi*
25/30 77/85
PSSMsinsi 50 90.5 65.5 83.350
19/3890.5
95/10582.5
Geno2 84.2 81 61.5 93.484.2/
80.985/105
81.8Significance level P (Area=0.5) 0,0001
Geno 84.2 81 61.5 93.432/38 85/105
81.8
SVM 60.5 91.4 71.9 86.560.523/38
91.496/105
83.2
Chueca et al, J Med Virology, 2009, 81: 763-767 Garcia F et al , 4th HIV Entry Workshop, 2008
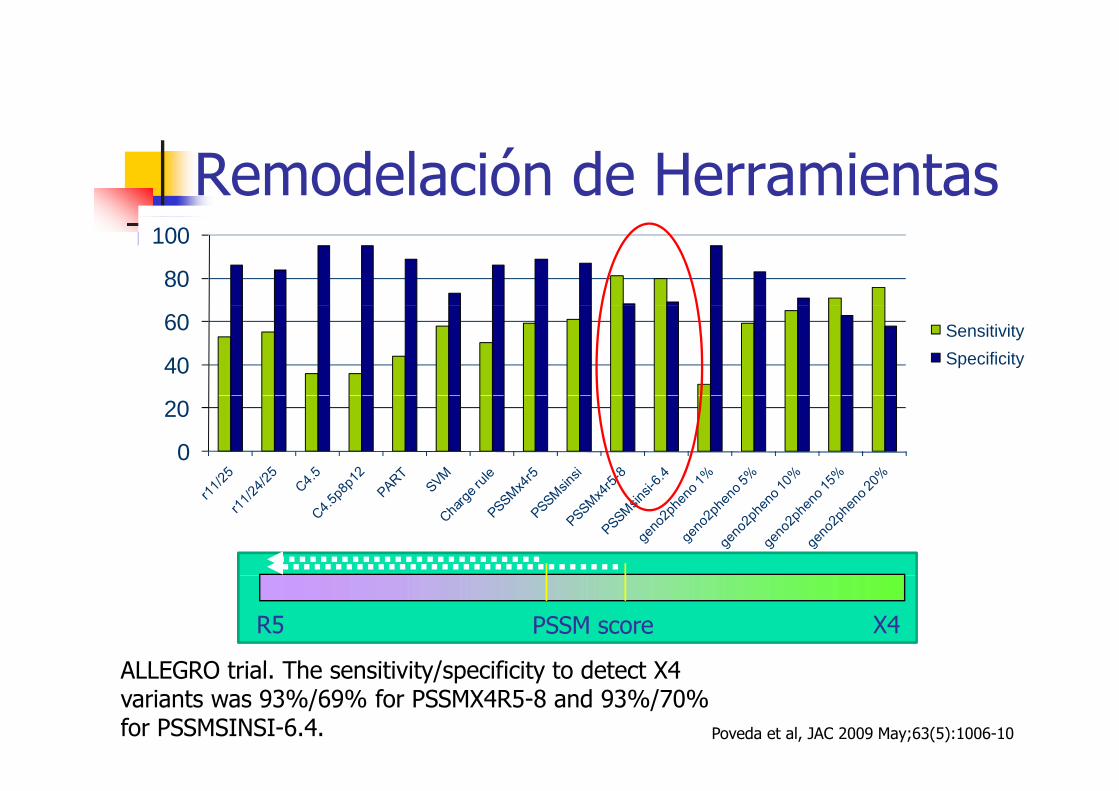
Remodelación de Herramientas
80
100
40
60 SensitivitySpecificity
0
20
PSSM scoreR5 X4
ALLEGRO t i l Th iti it / ifi it t d t t X4
Poveda et al, JAC 2009 May;63(5):1006-10
ALLEGRO trial. The sensitivity/specificity to detect X4 variants was 93%/69% for PSSMX4R5-8 and 93%/70% for PSSMSINSI-6.4.
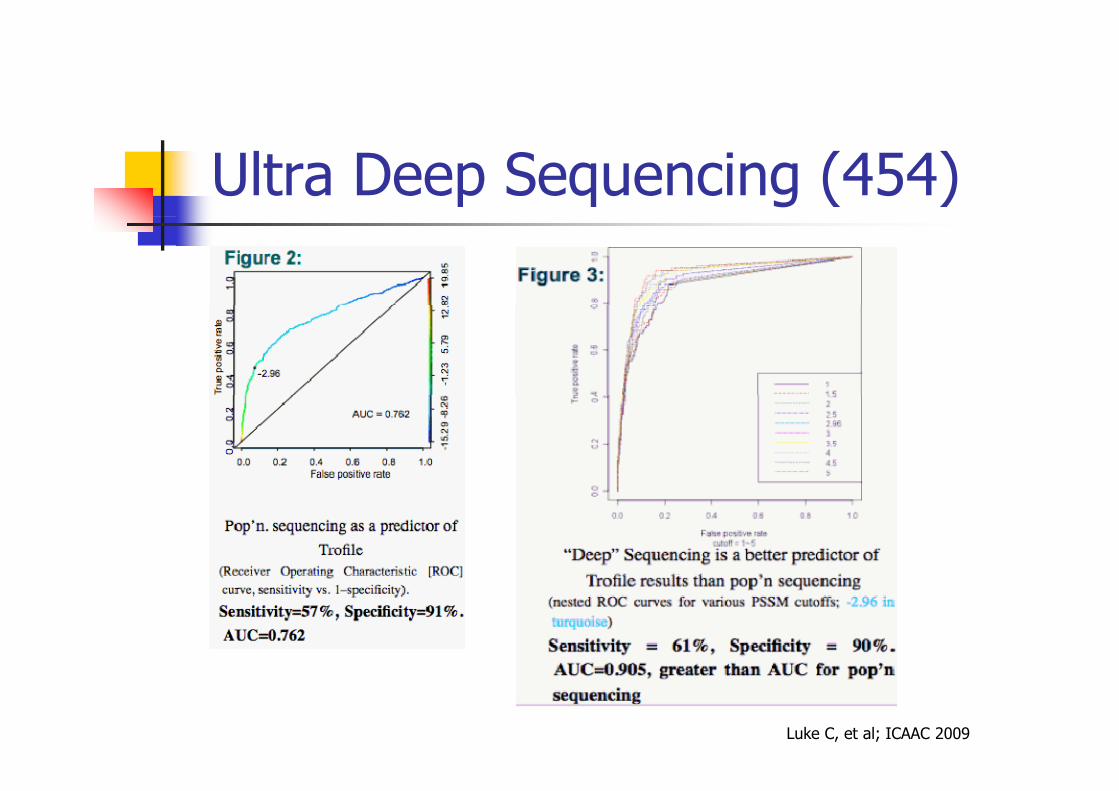
Ultra Deep Sequencing (454)
Luke C, et al; ICAAC 2009
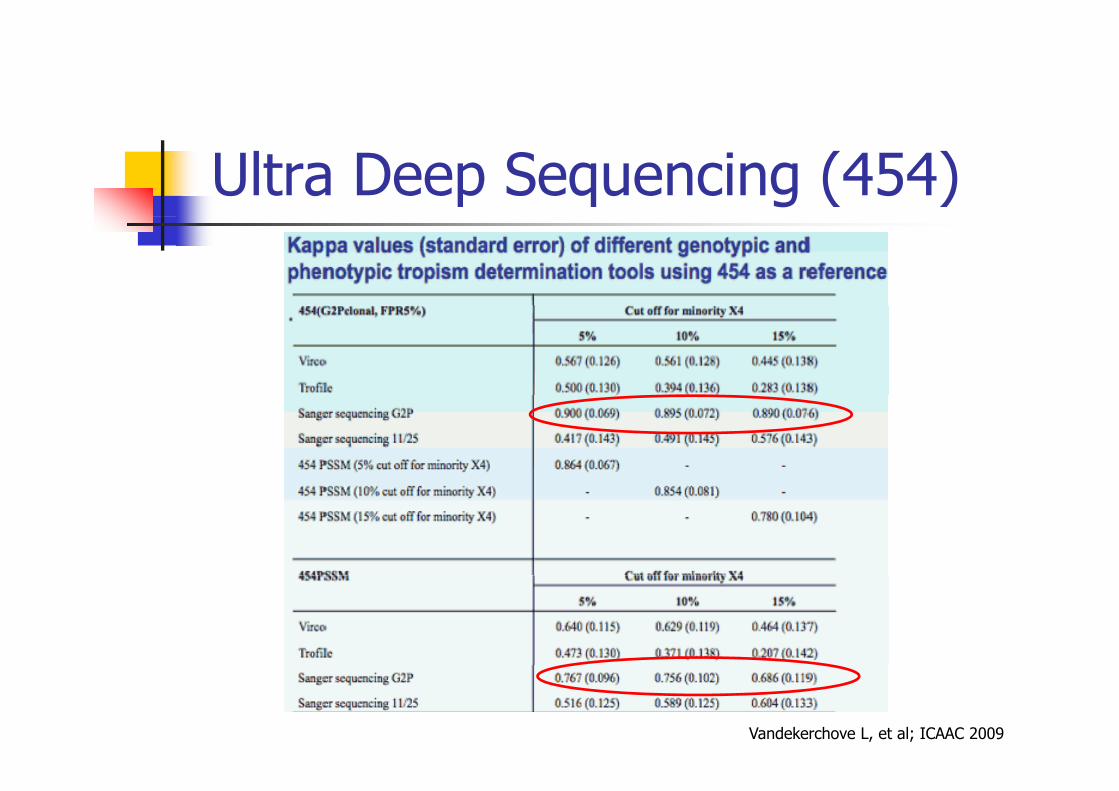
Ultra Deep Sequencing (454)
Vandekerchove L, et al; ICAAC 2009
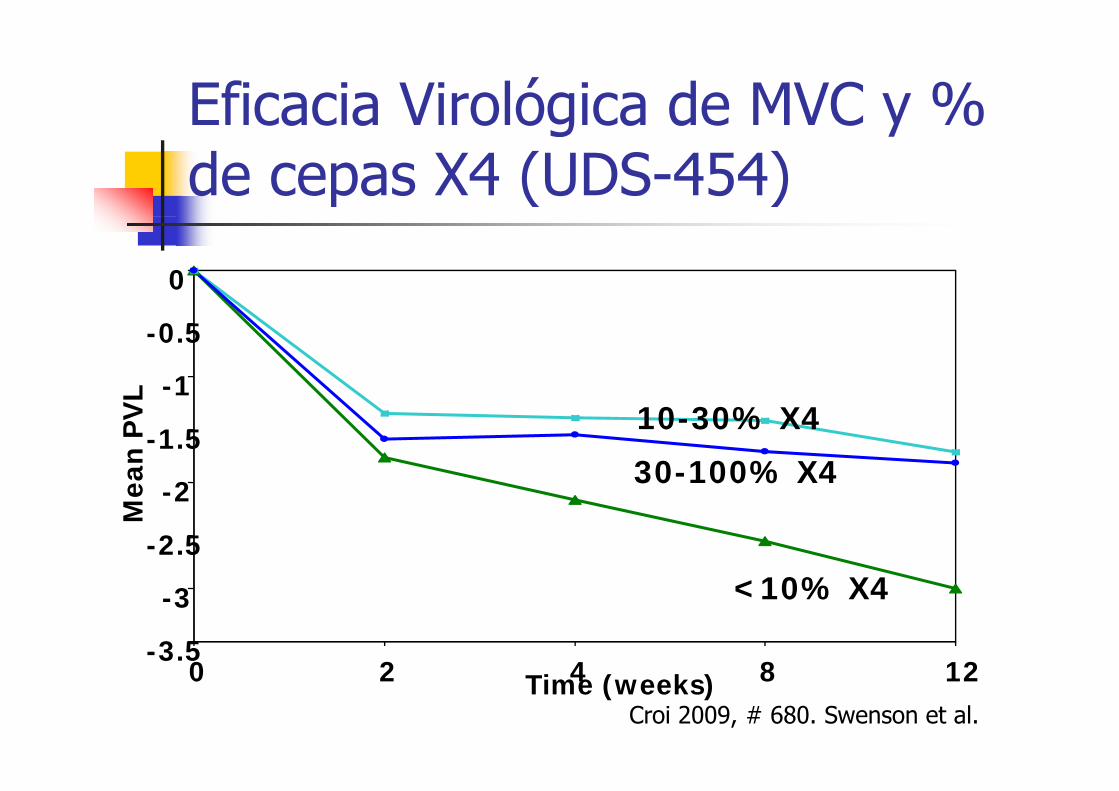
Eficacia Virológica de MVC y % g yde cepas X4 (UDS-454)
0
-1
-0.5
L
10-30% X4
30-100% X42
-1.5
ean
PV
L
-2.5
-2
Me
<10% X4
-3.5
-3
0 2 4 8 120 2 4 8 12Time (weeks)Croi 2009, # 680. Swenson et al.
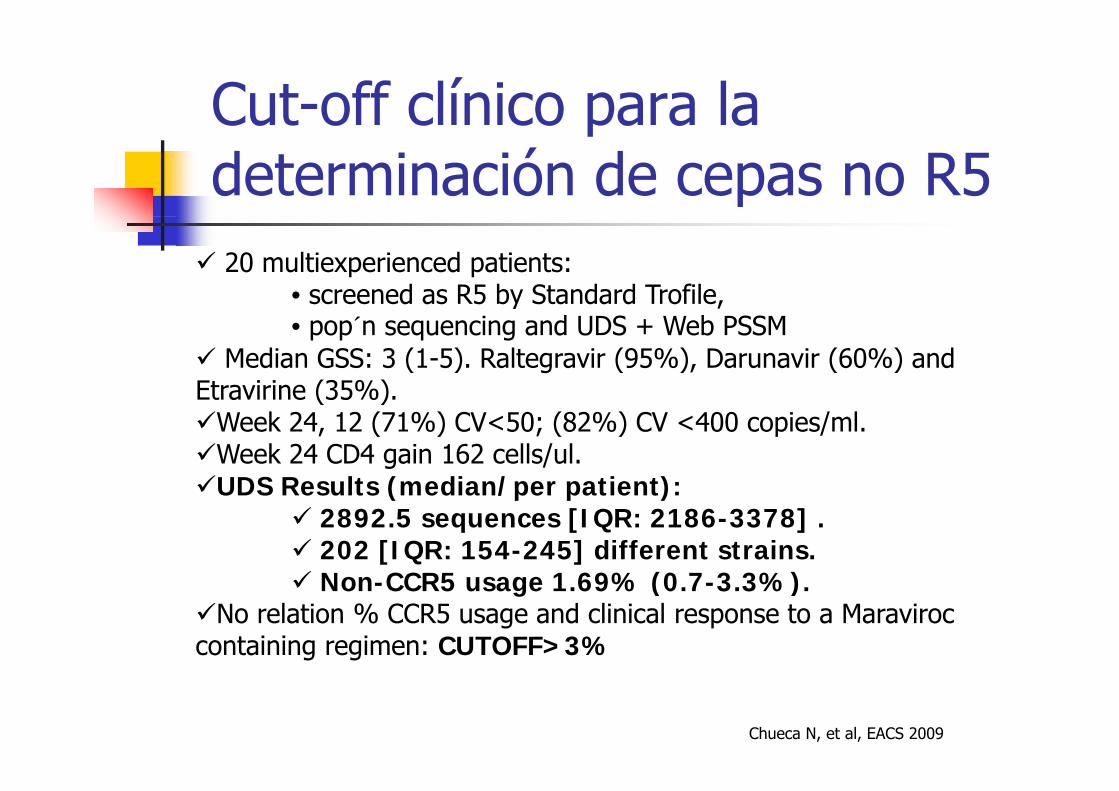
Cut-off clínico para la pdeterminación de cepas no R520 multiexperienced patients:
• screened as R5 by Standard Trofile, y ,• pop´n sequencing and UDS + Web PSSM
Median GSS: 3 (1-5). Raltegravir (95%), Darunavir (60%) and Etravirine (35%)Etravirine (35%).
Week 24, 12 (71%) CV<50; (82%) CV <400 copies/ml. Week 24 CD4 gain 162 cells/ul.UDS Results (median/per patient):UDS Results (median/per patient):
2892.5 sequences [IQR: 2186-3378] .202 [IQR: 154-245] different strains.N CCR5 1 69% (0 7 3 3%)Non-CCR5 usage 1.69% (0.7-3.3%).
No relation % CCR5 usage and clinical response to a Maraviroc containing regimen: CUTOFF>3%
Chueca N, et al, EACS 2009
Volver a empezar?Correlación V3/Respuesta clínica
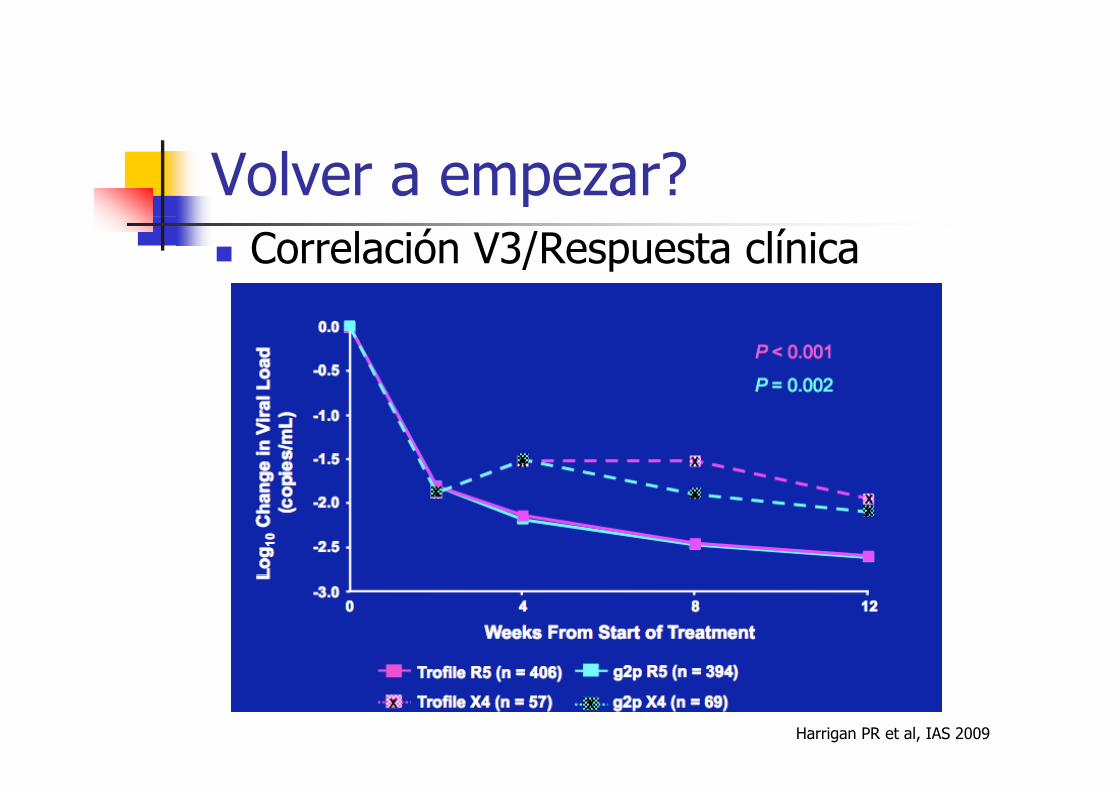
Volver a empezar?Correlación V3/Respuesta clínica
Harrigan PR et al, IAS 2009
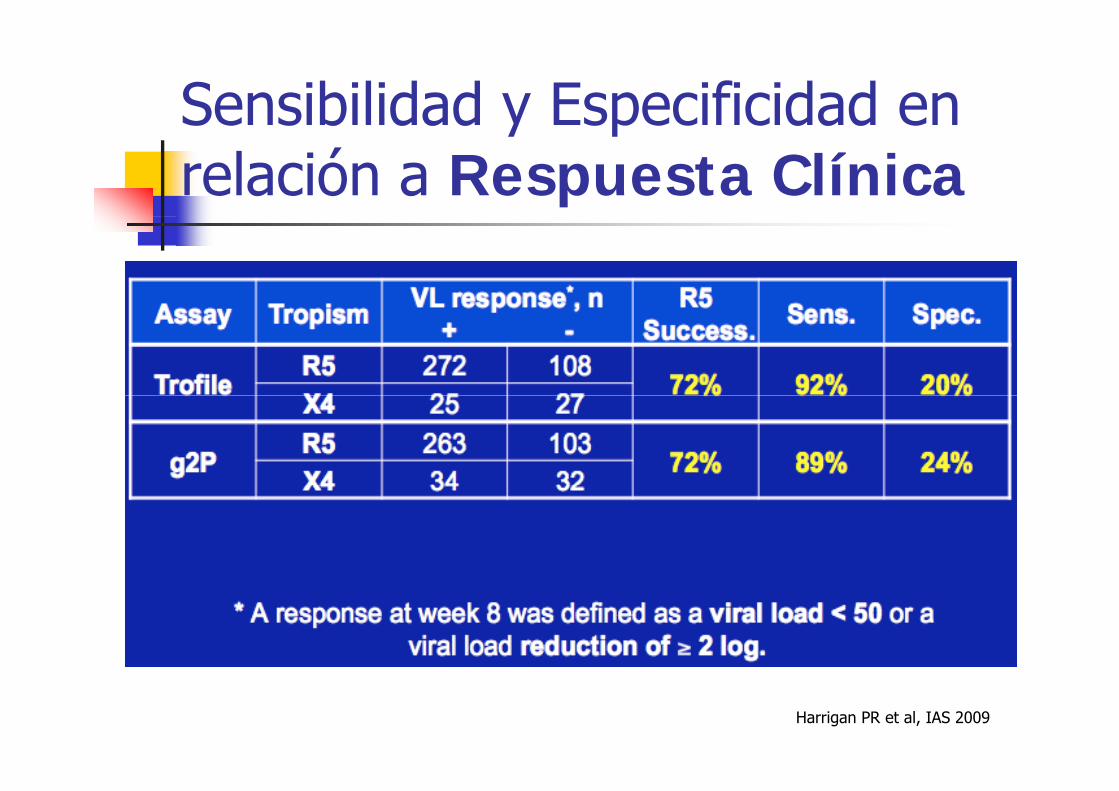
Sensibilidad y Especificidad en y prelación a Respuesta Clínica
Harrigan PR et al, IAS 2009
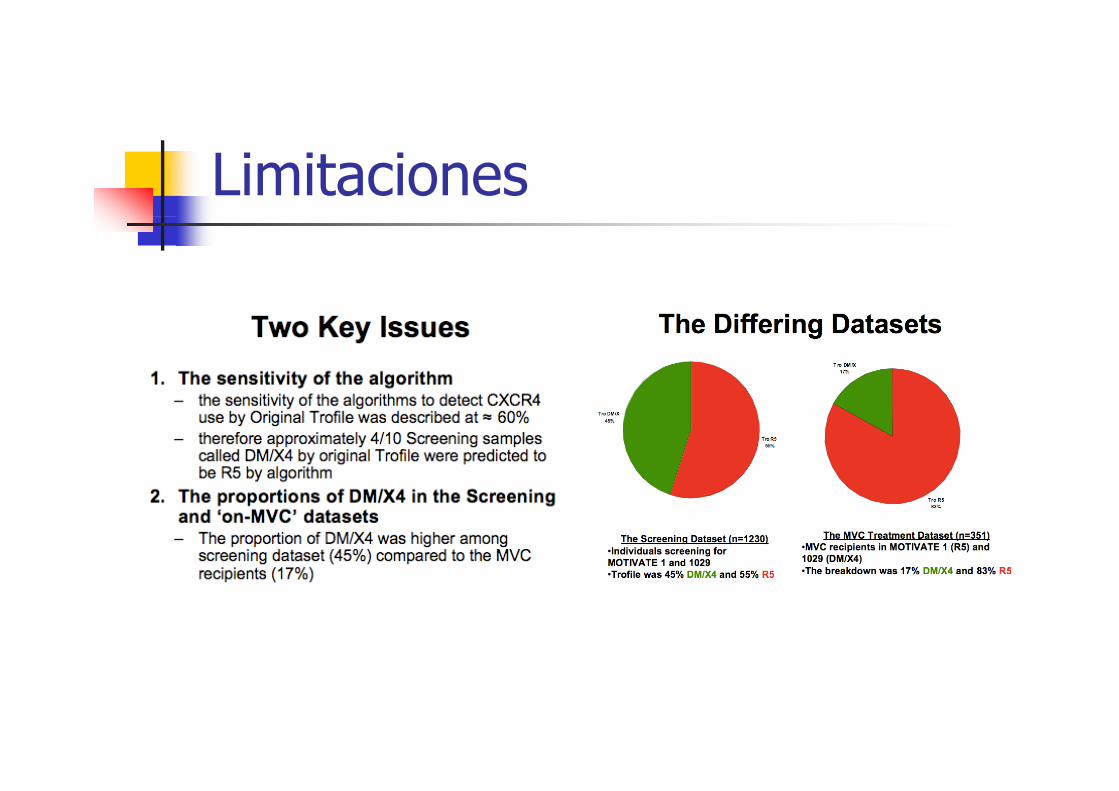
Limitaciones
Berlin Maraviroc Cohort
Week 12 (n=63)Week 12 (n 63)75% were successfully treatedSuccessful treatment was defined as VL <50 or VL-decline of at least 3 log10 levelsSubgroup: only genotypic tropism result available
N=23N=2318 patients (78%) were successfully treated
Week 24 (N=59)Still 75% were successfully treated
Obermeier M, et al,. 7th Eur HIVDR, 2009
Estudio UveTresV3: 75 muestras; 63 muestras ESTA. N CCR5 V3 18% ESTA 21%Non CCR5: V3-18%; ESTA-21%. No reportables: V3-3%; ESTA-13%. 12 pacientes estudio piloto UveTres12 pacientes estudio piloto UveTres,
V3-R5. ESTA NR: 2; ESTA DM-1. Mediana de 3 fármacos activosMediana de 3 fármacos activos3 pac. S4, 5 S12, 2 S24.Sólo 2 pacientes no se encuentran indetectablesSólo 2 pacientes no se encuentran indetectables
1 en semana 4, descenso de 2.91 Log1 24 CV 70 i / l1 en semana 24, CV=70 copias/ml.
Alvarez M, et al. SAEI 2009 (enviado)
Conclusions
Level III Expert opinion:p p
G2P V3 loop based genotyping is increasingly used i di ias a tropism prediction test.
The e is g o ing e idence fo a good co elationThere is growing evidence for a good correlation between tropism prediction based on V3 loop genotyping and therapy outcome (G2P), however g yp g py ( ),the number of cases evaluated is still limited.
Clinical management of HIV-1 tropism testing: development of European guidelines 7th Eur DRW, 2009
ContenidosTropismo del VIH: ImportanciaCó d d t i l t iCómo se puede determinar el tropismoControversias en 2009:
Podemos usar ya el genotipo V3? Es mejor UDS?UDS?Que hacer con pacientes con CV Indetectable (simplificación toxicidad )Indetectable (simplificación, toxicidad,...)
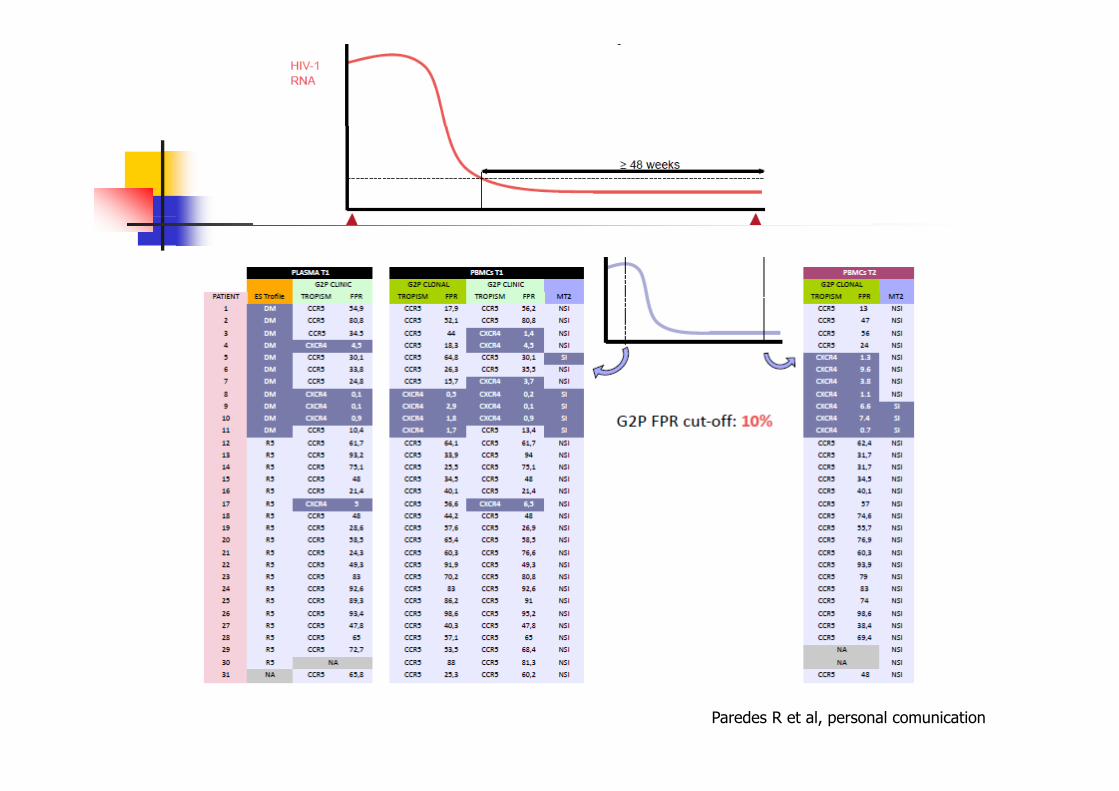
Paredes R et al, personal comunication
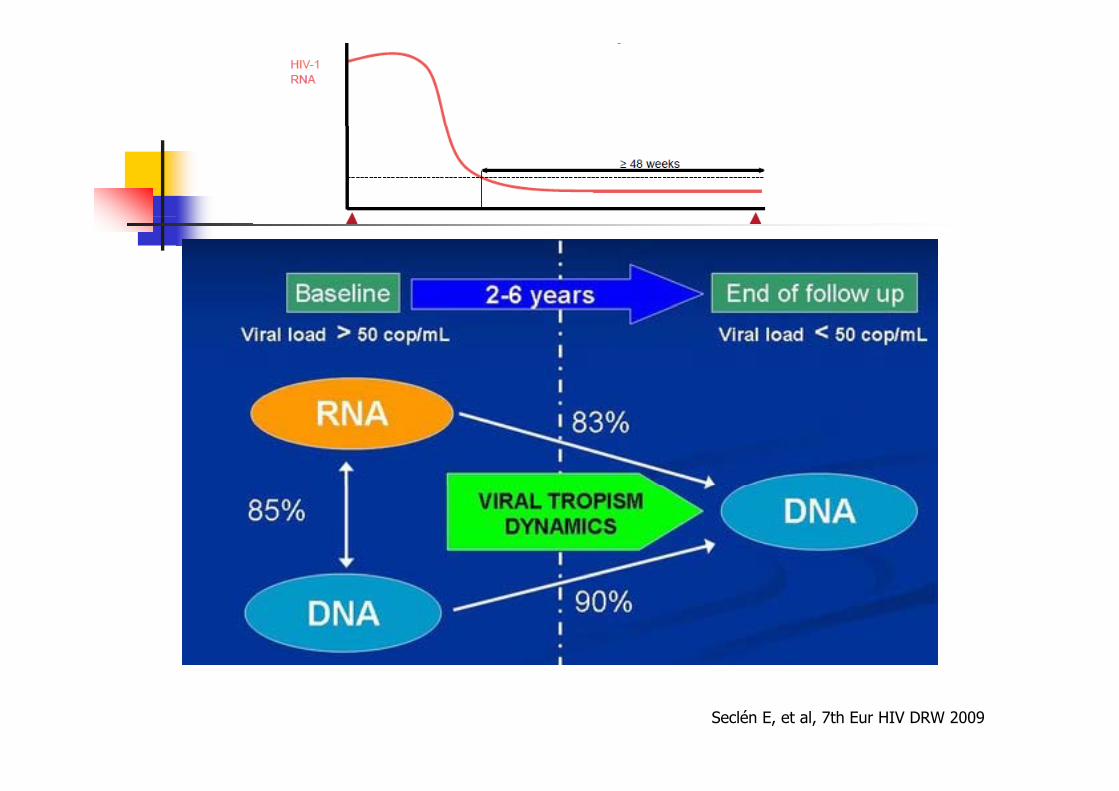
Seclén E, et al, 7th Eur HIV DRW 2009
Conclusions
Level III Expert opinion: If switch to Maraviroc is planned in patients with HIV RNA <50 copies/ml
retrospective testing of the latest sample with HIV RNA > 1000 may be consideredAlternatively, genotypic testing from proviral DNA may be consideredHowever, no clinical study data on Maraviroc efficacy in this setting are available
Clinical management of HIV-1 tropism testing: development of European guidelines 7th Eur DRW, 2009
“Take home message”
Fenotipo: útil en determinadas situaciones, en función al tipo de paciente y el tipo de régimen.paciente y el tipo de régimen.
La hipersensibilidad para X4, sin posibilidad de cuantificar y sin puntos de cortede cuantificar, y sin puntos de corte clínicos, es su principal defecto.
“Take home message”
El genotipo ha demostrado su utilidad, íespecialmente en regímenes en los que MVC
va acompañado de fármacos activos:Facilidad, coste y tiempo a resultados inclinan la balanza a favor del genotipo.
ó áLos estudios de validación que se están llevando a cabo son el principal argumento para su introducción en la rutina asistencialintroducción en la rutina asistencialSu detección en ADN proviral en pacientes con CV indetectable puede ser utilizado para apoyar laindetectable puede ser utilizado para apoyar la toma de decisiones clínicas.
Agradecimientos
Natalia Chueca, Pepi López, Marta Alvarez,Natalia Chueca, Pepi López, Marta Alvarez, Vicente Guillot, Alex Peña (HUSC, Granada)Eva Poveda (H. Carlos III), Roger Paredes (IrsiCaixa), Victoria Sánchez (H. Elche)Pfizer y a los investigadores y pacientes Estudio ALLEGRO, Estudio Granada UDS y Estudio UVETRES

![TI - unican.es · (IV) {isc1.m}:x [ n ]=!∞ k = −∞ x [ k ] δ [n − k ] ≡!∞ k = −∞ p k [n ]. p k [n ] ada x [k ] instante k. a p k [ n ] es v k [n ]= x [k ] h[n −](https://img.pdfslide.es/doc/110x75/5e89c15993604a6d474be7b4/ti-iv-isc1mx-n-a-k-aa-x-k-n-a-k-aa-k-aa.jpg)