Colisiones a baja velocidad y lesiones del raquis cervical: nexo causal
La perspectiva del médico valorador
Dr. D. Antonio Hernando Lorenzo
herloren@telefónica.net
Médico Especialista en Medicina Intensiva y Cardiología.
Magister en Valoración del Daño Corporal.
Profesor de Biomecánica de Lesiones A.H.L.

DIAGNOSTICO MEDICO
DX ETIOLOGICO
DX CLINICO
JUICIO CLINICO
A.H.L.

DIAGNOSTICO MEDICO
Criterios de Duke para Endocarditis Infecciosa Criterios Mayores: A. Hemocultivos positivos para Endocarditis Infecciosa (IE)
1- Microorganismos típicos compatibles con IE con al menos 2 hemocultivos separados, como los siguientes:
Streptococcus viridans, Streptococcus bovis, o grupo HACEK*, o
Staphylococcus aureus o enterococo adquirido en la comunidad, en ausencia de un foco primario,
2- Microorganismos compatibles con IE en hemocultivos persistentemente positivos definidos como:
2 muestras de hemocultivos positivos tomados en forma separada por >12 horas, o
Todos de 3 o la mayoría de 4 hemocultivos separados (con la 1ª y la última muestra separados por 1 hora)
B. Evidencia de compromiso endocárdico
1- Ecocardiograma positivo para IE definido como:
· Masas intracardíacas oscilantes (vegetaciones) en válvulas o estructuras adyacentes, en dirección del jet
de regurgitación, o en material implantado en ausencia de una explicación anatómica alternativa, o
· Abscesos, o
· Nueva dehiscencia parcial de válvula protésica, o
2- Nueva regurgitación valvular (empeoramiento o cambio de un soplo preexistente insuficiente)
Criterios Menores: - Predisposición: cardiopatía predisponente o uso de drogas endovenosas
- Fiebre: temperatura > 38,0° C (100,4° F)
- Fenómenos vasculares: embolia arterial mayor, infartos pulmonares sépticos, aneurisma micótico, hemorragia
intracraneal, hemorragia conjuntival, y lesiones de Janeway
- Fenómenos inmunológicos: glomerulonefritis, nódulos de Osler, manchas de Roth, y factor reumatoide
- Evidencia microbiológica: hemocultivos positivos pero no encontrado como criterio mayor más arriba o
evidencia serológica de infección activa con organismos compatibles con IE
- Hallazgos ecocardiográficos: compatible con IE pero no encontrado como criterio mayor más arriba
Criterios clínicos para endocarditis infecciosa requiere:
• Dos criterios mayores, o
• Uno mayor y tres criterios menores, o
• Cinco criterios menores
A.H.L.

A.H.L.

23 de Abril de 2015 A.H.L.


. BIOMECANICA de LESIONES ESGUINCE CERVICAL (WHIPLASH)
Variables:
Accidente (Tipo, Deformaciones, Coste reparación -?-) Información
Tramitador
Vehículos (Pesos, marca, modelo, seg. pasiva,
-cint. seg., airbag, reposacabezas-, etc.) Información
Reconstrucción por Ingeniero
Ocupantes (Sexo, edad, posición, estado anterior, etc.) Información médica + pruebas complementarias
Reconstrucción Médica
oç
A.H.L.

. BIOMECANICA de LESIONES ESGUINCE CERVICAL (WHIPLASH)
Variables:
Ocupantes (Sexo, edad, posición, estado anterior, etc.) Información médica + pruebas complementarias
Reconstrucción Médica
MANIFESTACIONES CLINICAS:
Sistema Nervioso Central (cefaleas, nistagmus, desprendimiento vítreo,
afectación arteria vertebral, etc.)
O. R. L. : Vértigos, Sínd. Laberínticos, Fístula canales, Acúfenos, etc
Patología nerviosa periférica ( N. espinal largo, hernia/protusión discal )
Muscular : Esguince lumbar
Síndromes Psíquicos : Depresión, Alt. memoria, sueño, “Fibromialgia”
Otros …(ej. rotura meniscal)
A.H.L.

• Tipo, modelo de automóvil
• Cambio de velocidad (Delta-V) : (Síntomas “breves”)
• Aceleración (Síntomas “duraderos”)
• Género (Femenino: X2)
• Talla (Alta y en mujeres)
• Relación de Pesos de vehículos (“Proyectil” y “Diana”)
• Forma de Pulso (-Alto y Corto-)
• Diseño de Asiento y Reposacabezas
• Uso de Airbag
• Tipo de Colisión: Posterior (>) , Lateral, Frontal
• Barra de remolque (Valor de NC mas alto)
• Patología previa, Accidente Previo
RIESGO DE WAD : FACTORES

A.H.L.
Investigar la correlación entre riesgo de “WAD”,
calculado según datos de seguros de la vida real,
y entre valores de pruebas de ensayo con maniquíes



•El síndrome medular central es una forma de lesión medular incompleta, caracterizada por la disfuncionalidad en brazos y manos y una mayor funcionalidad en las piernas. Parece una paraplejia inversa ya que los brazos y manos quedan paralizados mientras que las extremidades inferiores funcionan correctamente. Habitualmente el daño se produce en la zona cervical o en las partes altas de la región torácica de la médula espinal. Esta enfermedad está asociada con isquemias, hemorragias o necrosis que afectan a la parte central del cordón espinal (las largas fibras que transportan la información directamente desde el córtex cerebral). Las fibras destinadas a los movimientos de las piernas están situadas en la zona más externa del cordón espinal. Este síndrome puede aparecer durante la recuperación de un shock espinal debido a una prolongada hinchazón alrededor o cerca de las vértebras, causando presión en la médula. Los síntomas pueden ser permanentes o pasajeros. (Hiperextensión con estenosis de canal medular, ej. Espondiloartrosis)


“Si todo te da igual,…
estás haciendo mal las cuentas”
Albert Einstein

A.H.L.
UTILIDADES DE LA BIOMECANICA En colisiones a baja velocidad, determinar “umbral lesivo mínimo” y… NEXO
CAUSAL
0
2
4
6
8
10
12
14
16
18
0 20 40 60 80 100
Time (ms)
Ac
ce
lera
tio
n (
g)
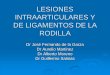
25 km/h, 8 g mean
16 km/h, 5 g mean
10 km/h, 4 g mean
10 km/h, 3 g mean
- Pulso de severidad alta ΔV = 25 km/h
- Pulso de severidad moderada ΔV = 16 km/h (Más representativo)
- Pulso de severidad baja ΔV = 10 km/h



Delta-V : Cambio de velocidad tras la colisión
Post Pre
V1= Velocidad Final
V1= Velocidad Inicial
m2 m1
V2= Velocidad Final
V2= Velocidad Inicial
A.H.L.

Ilustración de los vectores del Delta-V para 2 vehículos que colisionan
A.H.L.

Delta-V : Cambio de velocidad tras la colisión
Post Pre
V = V1 = V2
Considerando una Colisión Inelástica Ej. Bolas de Plastilina
Quedan “pegados” tras la colisión. Van al misma velocidad
A.H.L.

Delta-V : Cambio de velocidad tras la colisión
Considerando una Colisión Inelástica Ej. Bolas de Plastilina
Quedan “pegados” tras la colisión. Van al misma velocidad
A.H.L.

Delta-V : Cambio de velocidad tras la colisión
A.H.L.

Colisión Elástica Pura: Bolas de Billar - Efecto (CR)
Las colisiones reales tienen un componente Elástico
Coeficiente de Restitución (CR) 0 : Inelástica Pura 1: Elástica Pura
Habitual en colisiones reales a baja velocidad : CR = 0,4
Cuando se quedan “empotrados” : CR = 0,1 A.H.L.

(1) (2)
1.500 Kg.
30.000 Kg.
V= 60 Kms/h
V= 60 Kms/h
= 115 Kms/h
= 5 Kms/h
MORTAL
LEVE
A.H.L.

A.H.L.
COLISION POR ALCANCE POSTERIOR

A.H.L.
COLISION POR ALCANCE POSTERIOR

A.H.L.

El Tp se definió como el tiempo cuando la aceleración pasó de (+) a (-) después
que hubiese ocurrido el 90% del delta-V.
La aceleración media se calculó como delta-V(en Tp)/Tp.
Para un cambio de velocidad dado, una aceleración media mas alta por lo tanto
corresponde a una duración mas corta del pulso de colisión A.H.L.







El Solapamiento Total Potencialmente MAS LESIVO








Freno: Toyota Corolla (15-45 mm, Ford Mondeo : 120 mm)




A.H.L.

A.H.L.
“ALCANCES A BAJA VELOCIDAD” REPORT ON A FULL-SIZE CRASH TEST – JUNE 2005
Technical Paper CT2\2005\
CONCLUSIONS
An impact velocity of 11.1 mph gave rise to a delta v (Dv) of 5.97 mph for the target
vehicle. This is within 0.3 mph of a theoretical common post-impact velocity and
validates our methodology when investigating collisions of this nature.
Accelerometer readings for the target vehicle show a linear rise to maximum
acceleration in 0.11 seconds and a total collision time of 0.22 seconds.
Accelerometers attached to the head and chest of the target vehicle driver recorded
significant accelerations in all three axial directions. The highest accelerations
occurred in the forward (8.3g) and upward (-8.9g) directions. They were of similar
magnitude and occurred at the same time thus indicating that they were probably part
of the same acceleration mechanism acting on the head of the driver.
During this time the head of the driver was accelerating from a position lagging
behind the chest towards a position in front of the chest. To achieve this, the head
would require a significantly higher acceleration than the target vehicle.
The maximum acceleration acting on the head of the driver was 11.9g. This was
primarily the resultant of the maximum accelerations in the forward and upward
directions.

A.H.L.
“ALCANCES A BAJA VELOCIDAD” REPORT ON A FULL-SIZE CRASH TEST – JUNE 2005
Technical Paper CT2\2005\
It is believed that a key feature contributing to injury in this type of low speed, rear-end
impact is the distance between the head of the driver and the head restraint at the time
of impact.
If the head were resting on the head rest at the time of the impact, the lag between the
head and chest would be minimised and the magnitude of the subsequent acceleration
phase when the head accelerates past the chest would be reduced.
Adaptive head rests that move into position behind the head at the moment of impact
are thought to have made a significant contribution to the reduction in whiplash
injuries in vehicles where they are installed.
The occupants of the target vehicle and in particular the driver, experienced some
symptoms following the collision. From these symptoms it is reasonable to conclude
that this impact was in the region of a threshold.
By this it is meant that an impact velocity slightly greater than that experienced would
have led to more serious symptoms and possibly injury that would require the
attention of a medical practitioner.
The results of this crash test support the opinion that a general threshold for whiplash
type injury is 5mph.

Viano and Gargan documented the head restraint position of 1,915 vehicles at an intersection. They found that only 10% of the occupants had the head restraint in the proper
position to avoid hyperextension.
Only ¼ of the adjustable head restraints were in the “up” position.
Viano DC, Gargan MF. Headrest position during normal driving: implication to neck injury risk in rear crashes. Accident Analysis and Prevention 1996;28(6):665-674.
Improper Head Restraint Positioning
Proper Head Restraint
Positioning
A.H.L.

. BIOMECANICA de LESIONES
ESGUINCE CERVICAL (WHIPLASH)
A.H.L.

. BIOMECANICA de LESIONES
ESGUINCE CERVICAL
PREVENCION - Reposacabezas activos
A.H.L.

Investigación y Reconstrucción de Accidentes
TRAMITADOR
ABOGADO
BIOMECANICA
Ingeniería
Medicina
Otros
A.H.L.

A.H.L.

¡¡ Muchas Gracias !!
A.H.L.

¡¡ Muchas Gracias !!
Y para acabar
de complicarlo, …
A.H.L.

¡¡ Muchas Gracias !!
A.H.L.

Applications and limitations of Forensic Biomechanics: A Bayesian perspective Michael D. Freeman Forensic and Legal Medicine, Feb. 2010, Vol. 17, No. 2, Pag. 67-77
A.H.L.

A.H.L.

A.H.L.

Risk to suffer whiplash by pulse angle
and impact direction related to gender A.H.L.

A.H.L.

A.H.L.

A.H.L.

ARTROSIS CERVICAL
A.H.L.
Degeneración del disco – pérdida de agua-
Disco jóven

Inversión
de Lordosis
Curvatura
Normal
A.H.L.

BIOMECANICA del TRAUMA
·
·
LESIONES CERVICALES
ALCANCE RADIOLOGIA
A.H.L.
Cervical curvature in acute
whiplash injuries:
prospective comparative study
with asymptomatic subjects
Injury, 29, (10), 775-778, Dec. 1998
Matsumoto M. y cols.

Abstract
The present study was undertaken to evaluate if MRI within 2 days of a motor vehicle
accident could reveal pathology of importance for understanding long-term disability
after whiplash necksprain injuries. As part of a prospective study cervical and
cerebral MRI was performed on 40 neck sprain patients with whiplash injury after car
accidents. The imaging was done within 2 days of the injury to make sure that any
neck muscle bleeding, oedema or other soft tissue injuries could be detected. The
MRI findings from the patients were both correlated to reported symptoms 6 months
after the accident and compared to a control group of 20 volunteers. The MRI of both
brain and neck revealed no significant differences between the patients and the
control group. When the patients were grouped according to the main MRI findings at
intake and compared according to the development of subjective symptoms reported
by the patients, the only significant difference was more headaches at 6 months in
the groups with disk pathology or spondylosis when compared to the group with no
pathology. In conclusion, MRI within 2 days of the whiplash neck-sprain injury could
not detect pathology connected to the injury nor predict symptom development and
outcome.
Injury, Vol. 28, No. 5–6, June–July 1997, 331–335
MRI of cerebrum and cervical columna
within two days after whiplash neck sprain injury
Grethe Borchgrevink y cols.
A.H.L.

.
Cesáreo Trueba Davalillo,
Daniel Alcázar de la Torre,
José M. Villazón
A.H.L.

. BIOMECANICA de LESIONES
ESGUINCE CERVICAL
A.H.L.

. BIOMECANICA de LESIONES
ESGUINCE CERVICAL
LIMITACIONES
DIAGNOSTICAS
Estudio incompleto
RX convencional
Estudios complementarios
A-P Lateral Oblícua 45º
A.H.L.

. BIOMECANICA de LESIONES ESGUINCE CERVICAL
LIMITACIONES
DIAGNOSTICAS
Estudio incompleto
RX convencional
Estudios complementarios
Oblícua 45º
A.H.L.

A.H.L.

LESIONES POR HIPEREXTENSIÓN: Son posibles por un mecanismo “de latigazo”. La Rx puede ser normal, por la reducción inmediata después del impacto. Ensanchamiento de la parte anterior del espacio intervertebral y la disminución del posterior, con prominencia de tejidos blandos sospecha
La avulsión asociada debe diferenciarse de fractura en lágrima, (el fragmento suelto tiene > diámetro transverso, que vertical) En casos graves hay luxación transitoria, con rotura de las estructuras de soporte y déficit neurológico variable. Lesión ligamentosa, de disco o partes blandas, - RM sagital -

A.H.L.

A.H.L.

A.H.L.

A.H.L.

Applications and limitations of Forensic Biomechanics: A Bayesian perspective Michael D. Freeman Forensic and Legal Medicine, Feb. 2010, Vol. 17, No. 2, Pag. 67-77
A.H.L.

EEUU:
28-834/105 /año (Cassidy/2000 – Ostremski/89)
Mujer: 20-24 años
Molestias Crónicas 6% (Schrader/96)
66% (Nunis/83)
TRASTORNOS ASOCIADOS AL “LATIGAZO CERVICAL”
A.H.L.

• Dolor (cuello, hombro, espalda, cadera)
• Mareos, vértigo
• Parestesias
• Síntomas cognitivos/psicológicos
• Otros, …
TRASTORNOS ASOCIADOS AL “LATIGAZO CERVICAL”
A.H.L.

"... La prevalencia
de dolor articular
cervical zygapofisario
fue 60%."
Las carillas
mas frecuentemente
lesionadas
fueron a nivel C2/C3
y C5/C6.
Wallis BJ, Lord SM, Bogduk N.
Resolution of psychological distress of
whiplash patients following treatment
by radiofrequency neurotomy: a
randomised, double-blind, placebo-
controlled trial.
Pain 1997;73:15-22.
C2/3, C3
C3/4, C4/5, C4
C6/7, C6, C7
C2/3, C3/4, C3
C4/5, C5/6, C4, C5
C4/5, C5/6, C4
C7/T1, C7
Patrones de Dolor Referido
A.H.L.

Neck and back injuries
• Myofascial
• Fractures and dislocations
• Disc herniation
• Spinal cord compression
• Spondylosis
• Radiculopathy
• Facet joint syndrome
• Increased development of spondylosis
Headaches
• Muscle contraction headache
• Greater occipital neuralgia
• Temporomandibular joint injury
• Migraine
• Third occipital headache
Dizziness
• Vestibular dysfunction
• Brainstem dysfunction
• Cervical origin
• Barré-Lieou syndrome
• Hyperventilation syndrome
Visual symptoms
• Convergence insufficiency
• Oculomotor palsies
• Abnormalities of smooth pursuit
and saccades
• Horner syndrome
• Vitreous detachment
Rare sequelae
• Torticollis
• Tremor
• Transient global amnesia
• Esophageal perforation and
descending mediastinitis
• Hypoglossal nerve palsy
• Superior laryngeal nerve paralysis
• Long thoracic neuropathy
• Spinal accessory neuropathy
• Cervical epidural hematoma
• Internal carotid
and vertebral artery dissection
• Symptomatic Chiari malformation
Paresthesias
• Trigger points
• Thoracic outlet syndrome
• Brachial plexus injury
• Cervical radiculopathy
• Facet joint syndrome
• Carpal tunnel syndrome
• Ulnar neuropathy at the elbow
Weakness
• Radiculopathy
• Brachial plexopathy
• Entrapment neuropathy
• Reflex inhibition of muscle contraction
by painful cutaneous stimulation
Cognitive, somatic,
and psychological sequelae
• Memory, attention,
and concentration impairment
• Nervousness and irritability
• Sleep disturbances
• Fatigability
• Depression
• Personality change
• Compensation neurosis
Sequelae of Whiplash Injuries
A.H.L.

BASE ORGANICA
• Carillas Articulares
• Ligamentos
• Discos Intervertebrales
• Arterias Vertebrales
• Ganglios de Raíces Dorsales
• Músculos
• ↑Presión LCR
TRASTORNOS ASOCIADOS AL “LATIGAZO CERVICAL”
A.H.L.

A.H.L.

A.H.L.

DOLOR CRONICO
• Orgánico (Lord/96, Sterling/06)
• Autoperpetuación
(Trastorno Adaptativo) – Ferrari/01
TRASTORNOS ASOCIADOS AL “LATIGAZO CERVICAL”
A.H.L.

BASE ORGANICA (A FAVOR)
• ↓ 31-75% (Dispositivos «Anti-Whiplash»)
(Farmer/03, Jakobsson/04, Viano/01)
• Peor recuperación con síntomas iniciales graves
(Williams/07, Scholten-Peeters/03)
TRASTORNOS ASOCIADOS AL “LATIGAZO CERVICAL”
A.H.L.

CARILLAS Y LIGAMENTO CAPSULAR
(Aprill/92, Barnsley/94)
• Pruebas diagnósticas (bloqueo de carillas)
• Tratamientos
(Neurotomía por Radiofrecuencia) – Lord/96
A.H.L.

1. Posición Normal 2. La Columna se endereza
3. Extensión de Cabeza 4. Rebote
Fases de un Alcance Posterior
A.H.L.

Columna Cervical Normal
A.H.L.

• Curvartura Normal, Suave, de la columna
• Cada articulación contribuye igualmente al movimiento
Extensión Normal de Columna Cervical
A.H.L.

Flexión y Extensión Normales
El movimiento normal de
la columna resulta de
pequeños movimientos
en cada articulación.
El movimiento normal de
cada articulación está
limitado a sólo pocos
grados de movimiento.
A.H.L.

0 milisegundos
En el momento del impacto,
el asiento del coche
comienza a moverse y el
ocupante todavía no se ha
acelerado hacia delante.
Movimiento durante una colisión
A.H.L.

Cuando el respaldo del coche
empuja el torso hacia delante,
la columna se mueve
adelante produciendo un
enderezamiento de la
columna torácica y cervical
La cabeza permanece
estacionaria
La columna
se endereza
A.H.L.
Movimiento durante una colisión
50 milisegundos
El respaldo empuja
el torso adelante

Esta diferencia en el
movimiento entre el cuello y
el torso produce una curva
con forma de S, en que casi
todo el doblaje de la
columna cervical ocurre en
la columna cervical baja.
Este doblaje rápido en sólo
unas pocas articulaciones,
puede producir daño
ligamentoso en la columna
cervical baja.
En este momento de la colisión, el asiento del
coche está empujando rápidamente el torso del
ocupante hacia delante, mientras que la cabeza
permanece quieta debido a la inercia
A.H.L.
El respaldo empuja
el torso adelante
La columna
toma una
forma de S
Movimiento durante una colisión 75 milisegundos

75 milisegundos 50 milisegundos
La columna se endereza Curva en forma de S
Movimiento Productor de Lesión
A.H.L.

Sobre los 150 milisegundos, el torso
ha empujado a hacia delante sobre la
parte inferior del cuello que fuerza a la
cabeza hacia atrñas sobre el
reposacabeza.
Dependiendo de la gravedad de la
colisión, lps ligamentos de la parte
anterior de la columna pueden
lesionarse durante esta fase
de la colisión.
La cabeza rota atrás
A.H.L.
Movimiento durante una colisión
El respaldo empuja
el torso adelante
150 milisegundos

Finalmente, la cabeza y el torso
son lanzados hacia delante
por la fuerza del asiento del coche
Cabeza lanzada adelante
Fuerza desde
El asiento del coche
A.H.L.
Movimiento durante una colisión
200 milisegundos

1 A.H.L.

A.H.L.
“ESGUINCE CERVICAL”

A.H.L.
“ESGUINCE CERVICAL”

A.H.L.
“ESGUINCE CERVICAL”

A.H.L.
“ESGUINCE CERVICAL”

A.H.L.

A.H.L.
“ESGUINCE CERVICAL”

A.H.L.
“ESGUINCE CERVICAL”

Vertebral Body Facet Joints
Intervertebral Disc Spinous Process
Facets
Normal Gliding Motion
Articulaciones de las Carillas Cervicales
A.H.L.
Apófisis espinosas
Apófisis espinosas Disco Intervertebral
Carillas Articulares
Cuerpo Vertebral Movimiento Normal
de Deslizamiento
Carillas

Facet joint
X-ray of facet joint.
The arrows show the
normal gliding motion of
these joints.
A.H.L.
Articulación de Carillas
RX de Carilla Articular
Las flechas muestran el movimiento normal
de deslizamiento de estas articulaciones
Carilla Articular

Pellizco
de carillas
Torso movement forward
Torso moving forward
Tearing of
ligaments
and disc
Facet Joint
Reflectors
Stretch
of facet
capsule
A.H.L.
Movimiento Anormal de carillas
Movimiento del torso
hacia delante
Desgarro
de ligamentos
y disco
Carilla
Articular
Compresión
de cápsula
articular
Movimiento del torso
hacia delante
Reflectores

Vertebral Motion During Impact
En vez de un movimiento
suave, la columna cervical
experimenta simultáneas
compresión y estiramiento.
Esto puede causar desgarro
en la parte anterior
de la columna
y pinzamiento en las
articulaciones de carillas
A.H.L.
Movimiento Vertebral durante el Impacto

El movimiento rápido del cuello
durante una colisión,
puede causar distintas lesiones
- muchas de las cuales son
imposibles de ver en RX o RMN. -
1. Lesiones del anillo
2. Arrancamientos de la
zaona marginal
3. Desgarros del LLAt
4. Apófisis Uncinadas
5. Fracturas Subcondrales
Articulares
6. Pilar Articular
7. Apófisis Articulares
8. Desgarro de Ligamento
Zonas de Lesión
A.H.L.

El dolor por las articulaciones
facetarias inflamadas, se
transmite por ramas mediales
del ramus dorsal.
La estimulación de los nervios
facetarios, a menudo produce
dolor referido
Articulaciones
Facetarias
Rama Medial
Ramus Dorsal
Apófisis Espinosa
Médula espinal
Nervios de las Articulaciones Facetarias
A.H.L.

CARILLAS Y LIGAMENTO CAPSULAR
ANATOMIA De C2 a C7 Articulación Sinovial – Cápsula Articular (Lig.) Inervación – Ramas Mediales de Ramo Primario Dorsal Mecanoreceptores – Nociceptores (amielínicos) Fibras Aδ y C Reaccionan a Sustancia P Péptido – Gen Calcitonina Neuropéptidos, Neurotransmisores y Neuromoduladores Nociceptivos
A.H.L.

A.H.L.

CARILLAS Y LIGAMENTO CAPSULAR
MECANISMOS LESIVOS Y TOLERANCIA • Pellizco Sinovial • Tensión excesiva de Cápsula → Rotación sobre CG elevado (“latigazo”) Tensiones (Estiramiento 29-40%) - N= <10% Giro de cabeza ↑ Tensión x 2 (latigazo) → Elongación de la Cápsula Activación de Receptores sí Tensión >10% (RATAS) Respuestas inflamatorias en la médula Lesión del Colágeno (Respuestas electrofisiológicas, inmunológicas)
A.H.L.

LIGAMENTOS Y DISCO
Desgarro
EVIDENCIA CLINICA DE LESION
Ligamentosas
• RMN – Lesiones Discales
- Mecanoreceptores + Nocireceptores (Kaale/05, Krakenes/06) • ↓ Movilidad Cervical y Propiocepción (Panjabi/06)
Desgarro
Parcial LCP
A.H.L.

LIGAMENTOS Y DISCO
ANATOMIA LLCA, LLCP, L. Capsular L. Interespinoso, L. Supraespinoso, L. Flavum - Elastina) Occipital-C1 y C1-C2 Lig. Alar, Lig. Transversos ↑ Colágeno, ↓ Elastina
- Estabilidad. Absorción E. - Sentido de Posición de Articulación
A.H.L.

Ligamentos de la columna cervical
Ligamentos
capsulares
de carillas
A.H.L. A.H.L.

LIGAMENTOS Y DISCO
MECANISMO LESIVO Y TOLERANCIA
En “Alcance” -- (LLCA en C5-C6)
Fibras Anulares del Disco
Tensiones Fisiológicas ↑ (Panjabi/04)
Con Aceleraciones < que en colisión frontal
5g (A), 6,5g (L), 8g (F)
↑ Riesgo (de C3-C4 a C7-D1)
Lig. Alar (≥ 8g) A.H.L.

ARTERIA VERTEBRAL
EVIDENCIA CLINICA DE LESION
• Espasmo o Estenosis → Altera Flujo
• SINTOMAS – (Reddy/02, Seric/00)
• Desgarros de Intima – (Rotación)
Art. C1-C2 (Taneichi/05, Chung/02)
• Perfusión Inadecuada de Tronco Cerebral A.H.L.

DISECCION VERTEBRAL (Segmento V3)
A.H.L.

ARTERIA VERTEBRAL
ANATOMIA
• Viscoelástica
– Adventicia – Colágeno
– Media – Músculo Liso y Fibras Elásticas
Entra en C6 – Sale en C1
Va en un Túnel Fibroso
A.H.L.

ARTERIA VERTEBRAL
MECANISMO LESIVO Y TOLERANCIA
• Extensión + Rotación Col. Cervical Alta (Chung/02, Davis(83) Elongación y ↓ Calibre (efecto Poisson) Pinzamiento o Compresión - Pueden causar desgarro intimal Elongación – 30mm (A), 17,5mm (L) con cabeza rotada 1340mm/s (a) y 610mm/s (L) Pico de Elongación – A los 85 m.
A.H.L.

GANGLIO RAIZ DORSAL Y RAIZ DORSAL
Ganglio Dorsal – Nervios Sensitivos
Procesamiento Dolor Central Alterado
Procesamiento Sensitivo Local Alterado
Aumento de Sensibilidad al Dolor (Hiperalgesia)
(Greening/05, Banic/04, Koelbaek/99)
A.H.L.

GANGLIO RAIZ DORSAL Y RAIZ DORSAL
ANATOMIA Anterior Nervios Espinales – Raíz Posterior Raíz Dorsal – Sensitiva Raíz Anterior – Eferente Ganglio de Raíz Dorsal – Sensible a Presión Las raíces nerviosas no tienen vaina Epineural gruesa → Sensibles a Presión
A.H.L.

GANGLIO RAIZ DORSAL Y RAIZ DORSAL
MECANISMO LESIVO Y TOLERANCIA Movimientos Cuello → Cambios de Volumen en Canal Medular Plexos Venosos Vertebrales Interno y Externo En «Latigazo» → Gradientes de Presión Transitorios Dentro y Fuera del Canal Medular (Aldman/86) Afectan a Raíces y Ganglios → Síntomas Experimentos – Lesión Celular Membrana en Ganglios Cadáver Estudios – Hemorragia Intersticial Ganglios de Raíz Dorsal
A.H.L.

GANGLIO RAIZ DORSAL Y RAIZ DORSAL
MECANISMO LESIVO Y TOLERANCIA
• NIC (Böstrom/00)
Relaciona Movilidad Cabeza-Cuello y
Magnitud de Presión en Canal Medular
• Aceleración y Velocidad Horizontal Cabeza y Tronco
Un NIC bajo – riesgo bajo lesión cervical duradera
(Kraft/03) A.H.L.

Vista Lateral Vista Desde arriba
Médula Espinal
Ligamento
Facetario
Raíces
Carilla
Articular
A.H.L.

A.H.L.

A.H.L.

GANGLIO RAIZ DORSAL Y RAIZ DORSAL
MECANISMO LESIVO Y TOLERANCIA • Deformación de Raíces • Compresión de Raíces en agujeros ↓ 20% ф Agujeros Intervertebrales de C4-C7 en Extensión Alcance: A=8g → ↓ 1,8mm ф en C5-C6 (Panjabi, Tominaga/06) RATAS: Cargas Transitorias en Raíces Dorales – Dolor Degeneración Walleriana Alteración Transporte Iónico Cargas → Alteración Funcional
A.H.L.

A.H.L.

A.H.L.

MUSCULO
Dolor Muscular o Miofascial (Evans/92)
No hay evidencia de lesión muscular directa (CPK)
Puede jugar papel indirecto
(Modulador del Dolor de otras estructuras)
A.H.L.

MUSCULO
ANATOMIA
Mayoría del volumen del cuello
Superficiales: ECM o Trapecio – Dolor en «latigazo», (cráneo, hombro)
Profundos: Esplenio, Escalenos, Semiespinal,
Largo (Vértebras)
Muy Profundos: Multifidus (Cápsula Facetaria)
A.H.L.

A.H.L.

MUSCULO
MECANISMO LESIVO Y TOLERANCIA
• Lesión directa por contracciones excéntricas
• Elongaciones musculares
(ECM en fase de retracción del «latigazo»)
• Impactos a δ-V de 8 Km/h → pico de tensión hasta 15% en ECM y hasta 50% en músculos posteriores
• Umbral para lesión muscular → (5-20%)
POR TANTO PUEDE HABER LESION MUSCULAR EN ALCANCES
A.H.L.

A.H.L.

A.H.L.

A.H.L.

MUSCULO
INTERACCIONES CON OTRAS ZONAS ANATOMICAS
1. Los músculos se unen directamente a la cápsula articular (Siegmund/08, Anderson/05)
2. La activación muscular afecta a las cargas y tensiones de otras estructuras anatómicas
3. El control neuromuscular alterado → dolor crónico por activación muscular inadecuada
Puede aumentar la compresión intervertebral y alterar la cinética invertervertebral → compresión axial
A.H.L.

Bibliografía
• Barnsley L, Lord SM, Wallis BJ, Bogduk N. The prevalence of chronic cervical zygapophysial joint pain after whiplash. Spine 1995;20:20-25.
• Bogduk N. Post whiplash syndrome. Australian Family Physician 1994;23:2303-2307.
• Brault JR, Wheeler JB, Siegmund GP, Brault EJ. Clinical response of human subjects to rear-end automobile collisions. Archives of Physical Medicine and Rehabilitation 1998;79:72-80.
• Eichberger A, Darok M, Steffan H, Leinzinger PE, et al. Pressure measurements in the spinal canal of post-mortem human subjects during rear-end impact and correlation of results to the Neck Injury Criterion (NIC). Traffic Safety and Auto Engineering Stream of the World Congress on Whiplash-Associated Disorders, 1999:345-359.
• Farmer CM, Wells JK, Werner JV. Relationship of head restraint positioning to driver neck injury in rear-end crashes. Traffic Safety and Auto Engineering Stream of the World Congress on Whiplash-Associated Disorders, 1999:70-89.
A.H.L.

• Fukui S, Ohseto K, Shiotani M et al. Referred pain distribution of the cervical zygapophysial joints and cervical dorsal rami. Pain 1996;68:79-83.
• Grauer JN, Panjabi MM, Cholewicki J, Nibu K, Dvorak J. Whiplash produces an s-shaped curvature of the neck with hyperextension at lower levels. Spine 1997;22:2489-2494.
• Insurance Institute for Highway Safety, Press Release, April 7, 1998.
• Insurance Institute for Highway Safety, Status Report, 1997. 32(4).
• Insurance Institute for Highway Safety, Status Report, 1999. 34(5).
• Kaneoka K, Ono K, Inami S, Hayashi K. Motion analysis of cervical vertebrae during simulated whiplash loading. Traffic Safety and Auto Engineering Stream of the World Congress on Whiplash-Associated Disorders 1999:152-160.
• Kornhauser M. Delta-V thresholds for cervical spine injury. 1996, SAE 960093.
• Kumar S, Narayan Y, Amell T. Role of awareness in head-neck acceleration in low velocity rearend impacts. Compendium of papers presented at the Traffic Safety and Auto Engineering Stream, World Congress on Whiplash-Associated Disorders 1999;276-296.
• Lord SM, Barnsley L, Wallis BJ, Bogduk N. Chronic cervical zygapophysial joint pain after whiplash: a placebo-controlled prevalence study. Spine 1996;21(15):1737-1745.
A.H.L.

Lord SM, Barnsley L, Wallis BJ, et al. Percutaneous radio-frequency neurotomy for chronic cervical zygapophysial joint pain. New England Journal of Medicine 1996;335(23):1721-1726.
Matsushita T, Sato TB, Hirabayashi K, et al. X-ray study of the human neck motion due to head inertia loading. 38th Stapp Car Crash Conference 1994; SAE 942208.
Ono K, Kaneoka K, Wittek A, Kajzer J. Cervical injury mechanism based on the analysis of human cervical vertebral motion and head-neck-torso kinematics during low speed rear impacts. Society of Automotive Engineers, 41st STAPP Car Crash Conference Proceedings 1997; SAE 973340.
Ortengren T, Hansson HA, Lovsund P, et al. Membrane leakage in spinal ganglion nerve cells induced by experimental whiplash extension motion: a study in pigs. Journal of Neurotrauma 1996;13(3):171-180.
Robbins MC. Lack of relationship between vehicle damage and occupant injury. SAE 970494.
Siegmund GP, Brault JR, Wheeler JB. The relationship between clinical and kinematic responses from human subject testing in rear-end automobile collisions. Traffic Safety and Auto Engineering Stream of the World Congress on Whiplash-Associated Disorders, 1999:181-207.
Siegmund GP, King DJ, Lawrence, JM, et al. Head/neck kinematic response of human subjects in low-speed rear-end collisions. Society of Automotive Engineers, 41st STAPP Car Crash Conference Proceedings 1997; SAE 973341.
… A.H.L.

Szabo TJ, Welcher JB. Human subject kinematics and electromyographic activity during low speed rear impacts. 40th Stapp Car Crash Conference, SAE 962432.
van den Kroonenberg A, Philippens M, Cappon H, et al. Human head-neck response during low-speed rear end impacts. 42nd Stapp Car Crash Conference Proceedings (P-227), 1998. SAE 983158.
Viano DC, Gargan MF. Headrest position during normal driving: implication to neck injury risk in rear crashes. Accident Analysis and Prevention 1996;28(6):665-674.
Wallis BJ, Bogduk N. Faking a profile: can naïve subjects simulate whiplash responses? Pain 1996;66:223-227.
Wallis BJ, Lord SM, Barnsley L, Bogduk N. Pain and psychologic symptoms of Australian patients with whiplash. Spine 1996;21(7):804-810.
Wallis BJ, Lord SM, Barnsley L, Bogduk N.The psychological profiles of patients with whiplash-associated headache. Cephalgia 1998;18:101-105.
Wallis BJ, Lord SM, Bogduk N. Resolution of psychological distress of whiplash patients following treatment by radiofrequency neurotomy: a randomised, double-blind, placebo-controlled trial. Pain 1997;73:15-22.
Yoganandan N, Pintar FA, Cusick JF. Biomechanical analyses of whiplash injuries using experimental model. Traffic Safety and Auto Engineering Stream of the World Congress on Whiplash-Associated Disorders 1999:325-343.
A.H.L.

Apadac
1 Jornadas de Sinalização
Segurança Rodoviária e D a n o C o r p o r a l
148
¡¡ Muchas Gracias !!
herloren@telefónica.net
Antonio E. Hernando Lorenzo
Recommended