EVIDENCIA CIENTÍFICAPRÁCTICAS CENTRADAS EN LA RUTINA FAMILIAR Y EL ENTORNO FAMILIARROBIN MCWILLIAM, PH.D.THE RAM GROUP
XIII Congreso Internacional ORITEL, Asunción, Paraguay, 11/19/15

OUTLINEWhat is “evidence
based”?Ecomap Routines-Based
InterviewParticipation-Based GoalsPrimary Service
ProviderSupport-Based Home VisitsCollaborative Consultation to
Child Care

WHAT IS “EVIDENCE BASED”
• “Evidence based medicine is the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients. The practice of evidence based medicine means integrating individual clinical experience with the best available external clinical evidence from systematic research.” (p. 71)• Sackett, Rosenberg, Gray, Haynes, & Richardson (1996). BMJ
FROM EDUCATION
•“Any concept or strategy that is derived from or informed by objective evidence—most commonly, educational research or metrics of school, teacher, and student performance.”•The Glossary of Education Reform: http://edglossary.org/evidence-based/
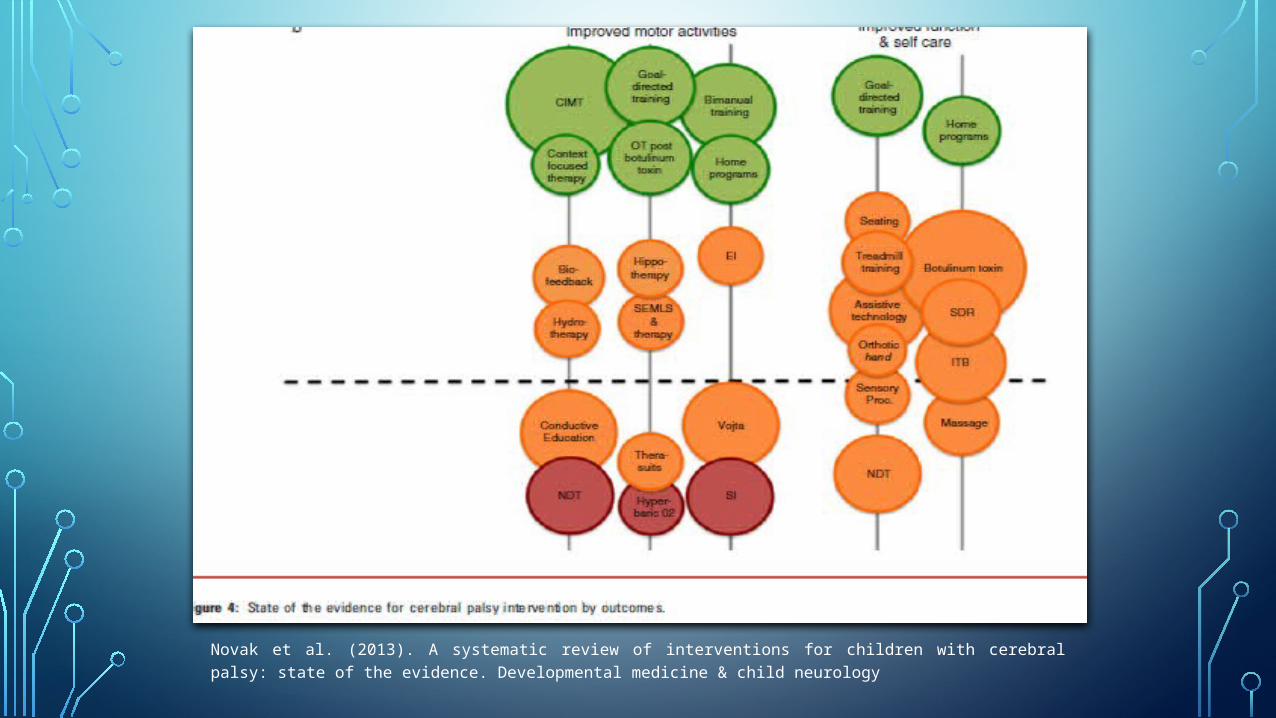
Novak et al. (2013). A systematic review of interventions for children with cerebral palsy: state of the evidence. Developmental medicine & child neurology



Two Designs1. Experimental
group comparison
2. Single-subject experimental
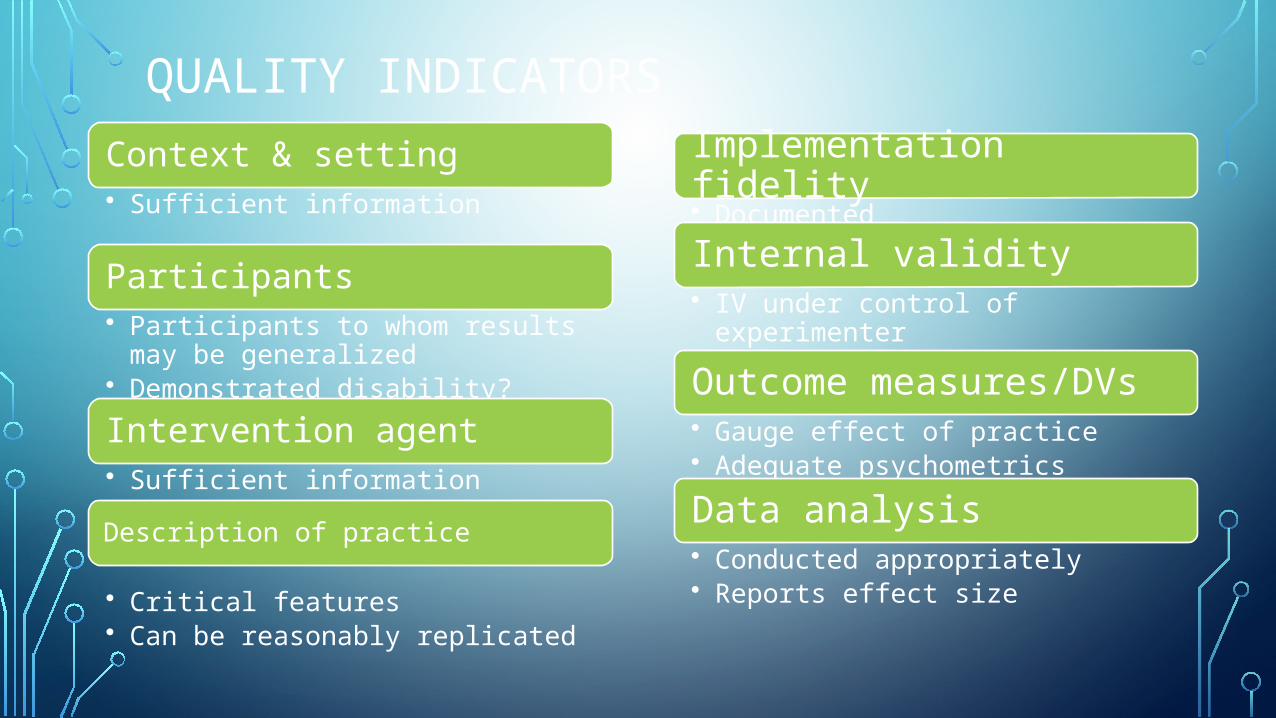
QUALITY INDICATORSContext & setting• Sufficient information
Participants• Participants to whom results may
be generalized• Demonstrated disability?Intervention agent• Sufficient informationDescription of practice
• Critical features• Can be reasonably replicated
Implementation fidelity• DocumentedInternal validity• IV under control of experimenter• Control and comparison
conditions/phasesOutcome measures/DVs• Gauge effect of practice• Adequate psychometricsData analysis• Conducted appropriately• Reports effect size

CLASSIFICATION•On basis of quantity, effects, & methodological soundness
1. Evidence-based practices2. Potentially EBPs3. Mixed effects4. Insufficient evidence5. Negative effects
CONCLUSION ABOUT EBPS
•Only look at well conducted studies•Enough participants, research groups, or studies•Sufficiently positive effects
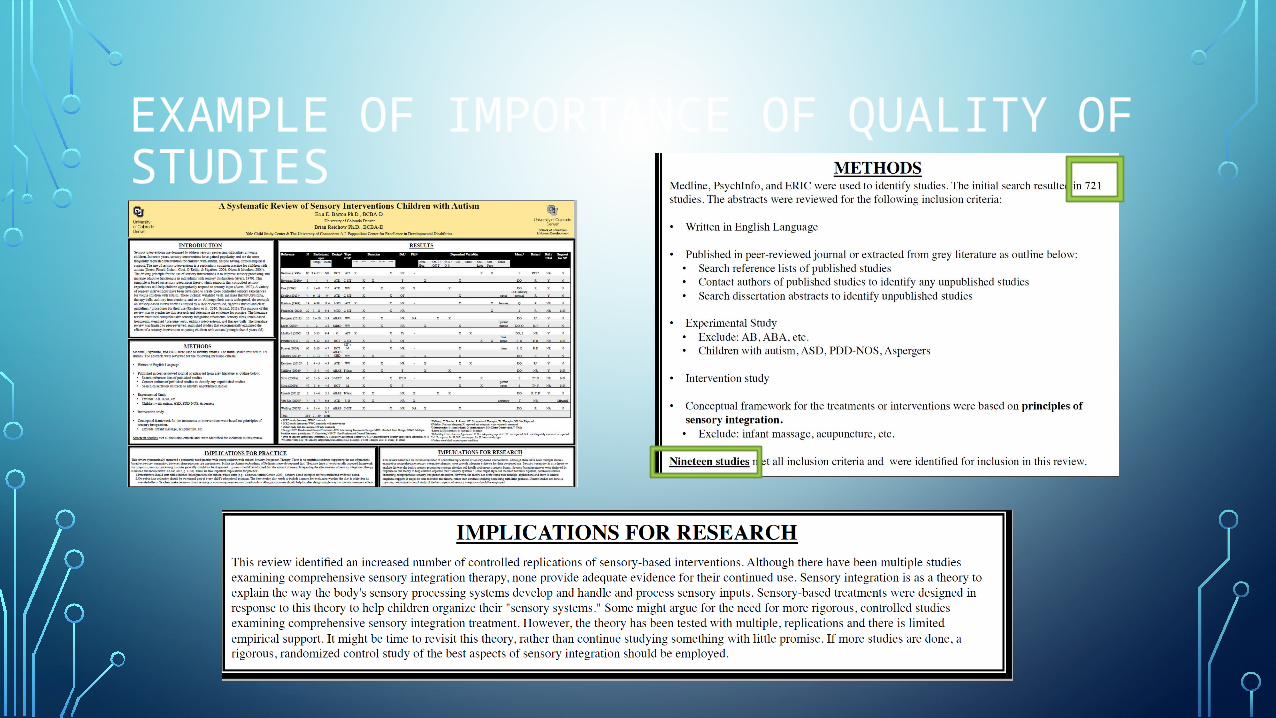
EXAMPLE OF IMPORTANCE OF QUALITY OF STUDIES
R. A. McWilliam (2015) 14
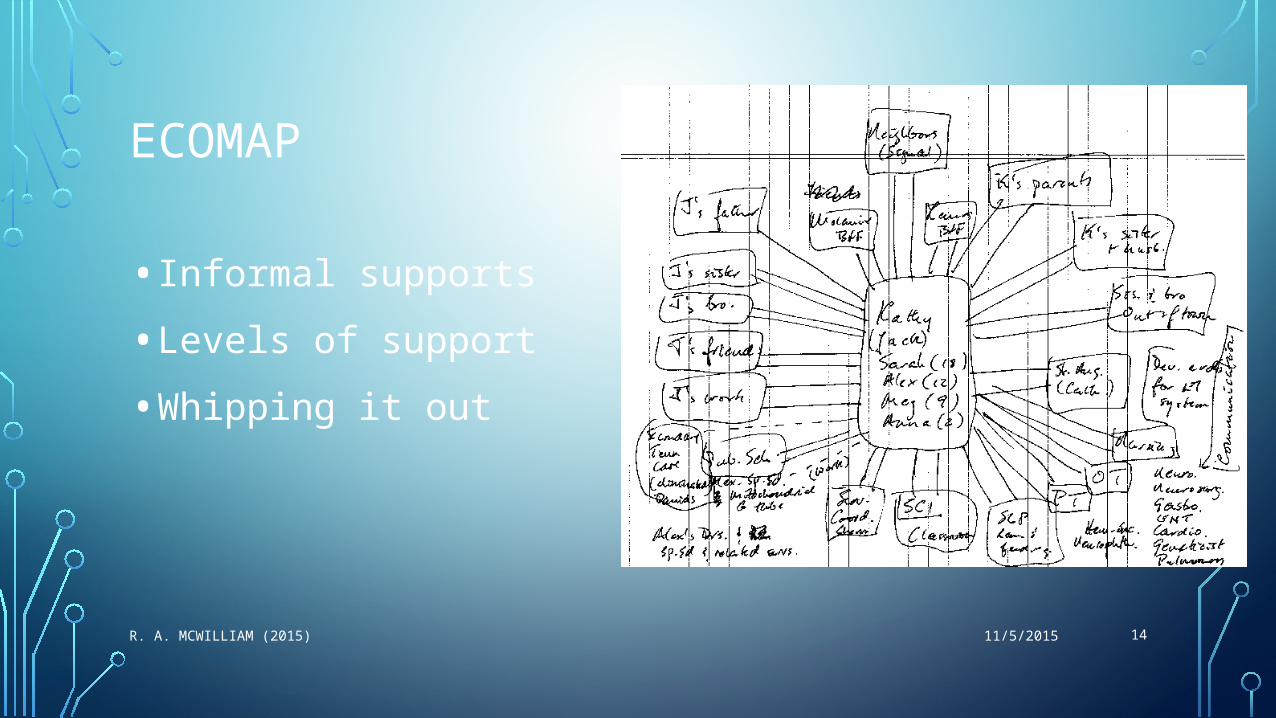
ECOMAP
• Informal supports• Levels of support•Whipping it out
11/5/2015

EVIDENCE BASE
•From Garbarino (1983)• Lab animals exposed to shock do not how symptoms of stress
when they are with members of their own species, but they do when exposed alone (Cassel, 1974)•Gorillas develop patterns of child abuse and neglect when left
to rear their babies in isolation but do not do so when they remain in the company of their group (Nadler, 1979; Rock, 1978)

•Studies of both lower animals and humans show higher rates of illness and death among those who have experienced disruptions of social relationships (Cassel, 1976)• Inmates in concentration camps coped better when they had a family member or at least someone perceived as a fellow (Eitinger, 1964)

•Blood samples from workers at stressful work sites show fewer biochemical indications of stress when the workplace is an interpersonally supportive setting (French, 1973).•Women with medically at-risk pregnancies suffer only 1/3 the complications at birth if they are well connected socially, with more friends and relatives in frequent contact (Nuckolls, Cassel, & Kaplan, 1972)

• Networks change over the lifespan, with size and strength being more or less important at critical times (Wrzus et al., 2013)• Review of literature revealed association between challenging
child characteristics and mothers’ inclination to seek social support, with mothers under more stress being more prone to pursue social support (Boyd, 2002)• For mothers with children with autism, informal support more
effective buffer against stress than formal support.• Parents with support related better to their children.• Low levels of support most powerful predictors of depression and
anxiety in mothers.

ROUTINES-BASED INTERVIEW
•Semi-structured, positive needs assessment•In-depth investigation into child and family functioning in routines•Includes emotional questions•Ends with family’s choosing goals

EVIDENCE BASE
• RBI part of a package, called RBEI, on which Hwang et al. (2013) conducted RCT: PEDI-C showed that the RBEI group had a faster progress rate in self-care functions and independence in social functions in the first 3 months of intervention and at the 6-month follow-up. • Boavida, Aguiar, & McWilliam (2014) studied 80 professionals
and showed that training on RBI resuted in large positive effects (> 3 SD) for quality ratings of objectives.

STUDIESS
•McWilliam, Casey, & Sims found that RBI-based IFSPs produced more functional goals.•McWilliam & Jenkins found parents had more positive views of their planning process when RBI conducted by their service provider than by dedicated service coordinator.
PARTICIPATION-BASED GOALS
• Functional child goals (skills needed for engagement in routines) written to emphasize child’s participation in routines, plus goal attainment criteria related to performance in context• Frederico will participate in outings and dinner by telling adult
what he sees. We will know he can do this when he names four objects or people when he’s in the car, four in the community, or four at dinner in one day for 5 consecutive days.

EVIDENCE BASE
•Urie Bronfenbrenner , 1974), “Is Early Intervention Effective?”•Referred to effect of increasing or decreasing a child’s participation in activities
•Cataldo & Risley (1970s): Participation in Planned Activities (PLA-Check) Engagement

• McWilliam, Trivette, & Dunst (1985): Engagement varies by routine and by setting• Dunst, Holbert, & McWilliam (1986); McWilliam, Casey, & Sims (2000s): Engagement
related to use of incidental teaching• McWilliam, Scarborough, & Ho (1990s): Teachers’ affect related to children’s
engagement• Campbell’s studies show practitioners’ desires, beliefs, and practices diverge from
family-centered and participation-based early intervention• Participation-based services: “provider role of promoting children’s participation in
family/community activities and routines” (Fleming, Sawyer, & Campbell, 2011). Unfortunately, practitioners did not articulate this as an important activity of EI.
PRIMARY SERVICE PROVIDER
• García Grau, Martinez, & McWilliam (2015): The more professionals, the lower the family quality of life• EI program service intensity had direct negative effects on self-
efficacy beliefs and parent and family well-being (Dunst, Hamby, & Brookfield, 2007)• Managerial and team resources required are high, but potential
payoffs for children, families, and therapists’ development are considerable (King et al., 2009)

SUPPORT-BASED HOME VISITS
•Home visitor is a comprehensive service provider•Checks on emotional, material, and informational•Family consultation about objectives, routines, family goals•Tools: Vanderbilt Home Visit Script, Matrix, Next-Steps Form, SBHV Checklist, Advanced Checklist

EVIDENCE BASE
•History of descriptive studies documenting nonrecommended practices (McBride & Peterson, 1997)•Home-based programs effective (e.g., Feldman et al., 1993)•Numerous studies now on HB treatments with children with autism, but roles of parents, professionals, and even children are all over the map
COACHING
• The new big thing: Everyone now an expert on coaching (e.g., FriOedman, Woods, & Salisbury, 2012): Operational definitions. In 2010, Salisbury, Woods, & Copeland called it collab consult.• Many studies have documented the effectiveness of training caregivers to
implement interventions, with resultant successes with children (e.g., Oono et al., 2013; Roberts & Kaiser, 2015)• 2 hrs therapy/week vs. 3.9 hrs services to caregivers: Treatment = greater gains
in social interaction skills; no diffs in standard language assessments. Caregiver skills associated with changes in children’s interaction skills (Casenhiser et al., 2013)

NOT TURNING PARENTS INTO TEACHERS/THERAPISTS•Mothers demonstrated positive, linear relationship between personal strain and number of hour spent delivering early intervention to their children (Schwichtenberg & Poehlmann, 2007).•OTOH, parent-coaching version of ESDM reported no increase in parenting stresss, whereas community group experienced increase (Estes et al., 2013).

EARLY CARE, EDUCATION, AND CHILD DEVELOPMENT (PHILLIPS & LOWENSTEIN, 2011)1. Parents most important influence, but ECE has impacts
in interaction with family effects2. Quality of adult-child interactions in ECE most potent
source of variation in child outcomes (with exposure amount)
3. Children in poverty most vulnerable to variation in ECE settings

PARENT-MEDIATED INTERVENTION: FROM DISABILITY AND REHABILITATION (MCCONNEL ET AL., 2014)• Study of 538 families raising children with disabilities in Alberta• Parents more likely to implement therapeutic regimens when
“enfolded” into other daily routines• “Finding a slot” to implement therapy = sacrificing personal leisure,
participation in paid work, time spent with family• “As a general rule, children do well when their families do well, and
families do well when they have the resources they need to juggle work and family and care demands.”
CHECKLIST TRAINING
• Performance checklists describe implementation with fidelity•Used to provide focused feedback on observed behavior•Used to monitor quality and fidelity• 8-40 items including fairly objective and fairly subjective items,
but all behaviorally stated• Scored yes (seen), no (not seen), partially seen, no opportunity
EVIDENCE BASE
• Increasingly used in medicine to reduce errors (e.g., Parsons et al., 2014)• Issue of who’s available cuts across disciplines (e.g., Lilaonitkul et al., 2015—anesthesiology)• Implementation: WHO Surgical Safety Checklist (e.g., in Chisinau, Moldova; Kwok et al., 2013)

RBM CHECKLISTS
• RBI Implementation Checklist• Support-Based Home Visiting Checklist• Advanced Home-Visiting Checklist• Integrated-Therapy Checklist• Incidental Teaching Checklist• Etc.

CONCLUSION
RBM
Ecomaps
RBI
Participation-Based Goals
Primary/ Comprehen-sive Service Provider
Support-
Based HVs
CC2CC
Checklist
Training

OUTCOMES
Family Quality of Life
Goal Attainm
ent
Functioning in
Routines
Recommended