Hernia diafragmática congénita y capacidad física, una evaluación
longitudinal
Leontien C.C. Toussaint-Duyster, Monique H.M. van der Cammen-van Zijp,
Johan C. de Jongste, Dick Tibboel, Rene M.H. Wijnen, Saskia J. Gischler, Joost van
Rosmalen,
Hanneke IJsselstijn
Resumen
Objetivo: Los niños con hernia diafragmática congénita (HDC) sufren de morbilidad
pulmonar a largo plazo. Faltan datos longitudinales acerca de la capacidad para el
ejercicio en estos niños. Nuestra hipótesis fue que la capacidad para el ejercicio estaría
disminuida en los niños con HDC y que se deteriora con el tiempo. Evaluamos la
capacidad para el ejercicio y sus determinantes en pacientes con HDC
longitudinalmente hasta los 12 años de edad.
Diseño: Estudio prospectivo longitudinal de seguimiento hasta los 12 años de edad.
Pacientes: Ciento catorce niños con HDC nacidos entre 1999 y 2012.
Métodos: La capacidad para el ejercicio fue evaluada utilizando el protocolo de Bruce a
las edades de 5, 8, y 12 años. El parámetro para el primer resultado fue el score de
desviación estándar (SDS) del máximo tiempo de resistencia. Los datos fueron
analizados utilizando modelos lineares mixtos.
Resultados: Un total de 107niños (30 tratados con membrana de oxigenación
extracorpórea [ECMO] realizaron 131 pruebas de ejercicio confiables. A las edades de 5,
8, y 12 años, el tiempo medio SDS de resistencia (IC 95%) fue -0.44 (-0.65 a -0.24); -1.01
(-1.23 a – 0.78); -1.10 (-1.40—0.80), respectivamente, todo menor a 0 (p< 0.001). La
capacidad para el ejercicio cayó significativamente en el tiempo sin importar el
tratamiento con ECMO (5-12 años: non- ECMO p= 0.015; ECMO p= 0.006). La duración
de la estadía hospitalaria inicial y la capacidad de difusión corregida para el volumen
alveolar estuvieron asociadas con el tiempo SDS de resistencia (p< 0.001 y p= 0.039).
Conclusiones: En pacientes HDC la capacidad para el ejercicio se deteriora entre los 5 y
12 años de edad, independiente de tratamiento con ECMO. Los pacientes con HDC
pueden beneficiarse de evaluaciones a largo plazo de la capacidad para el ejercicio con
intervención oportuna.
Palabras claves
Niño, hernia diafragmática congénita, capacidad para ejercicio, oxigenación con
membrana extracorpórea, seguimiento, edad escolar

1- INTRODUCCIÓN
La hernia diafragmática congénita (HDC) se produce en 1 cada 3000-4000
nacimientos (1). Pese a que HDC es todavía una anomalía con riesgo de vida, las
tasas de sobrevida han aumentado en las décadas pasadas (2). Los avances en el
manejo quirúrgico y neonatal, así como la implementación de un protocolo
europeo estandarizado de tratamiento neonatal en Noviembre de 2007 (3) (Tabla 1
del suplemento online), han contribuido significativamente a tasas de sobrevida
más altas (2) que mostraron ser sostenibles en el tiempo y en muchos centros
alrededor del mundo. Con el aumento de sobrevida, más niños pueden sufrir de
morbilidades a largo plazo, incluyendo síntomas pulmonares. Los factores que
pueden contribuir a la morbilidad pulmonar a largo plazo son la hipoplasia
pulmonar con obstrucción persistente al flujo de aire (4, 5), daño pulmonar
iatrogénico debido a la ventilación mecánica (4), y cambios microestructurales en el
pulmón (6). Estas anormalidades pulmonares pueden llevar a capacidad para el
ejercicio disminuida en el largo plazo y afectar el desarrollo más tarde en la vida.
Mientras que varios estudios encontraron capacidad para ejercicio disminuida en
pacientes HDC en la edad escolar (7-11), unos pocos otros estudios mostraron
capacidad para el ejercicio normal en pacientes HDC en edad escolar (5, 12) y
adultos (13, 14). Estos estudios tienen mayormente un diseño transversal, pequeños
tamaños muestrales, e incluyeron pacientes nacidos antes de que estuviera
disponible un protocolo estandarizado de tratamiento postnatal. Una evaluación
longitudinal de la capacidad para el ejercicio en pacientes con HDC no ha sido
realizada hasta la fecha.
Por lo tanto, el objetivo del presente estudio fue evaluar longitudinalmente la
capacidad para el ejercicio a las edades de 5, 8, y 12 años en una gran cohorte de
pacientes HDC tratados con o sin ECMO. Secundariamente, tratamos de encontrar
determinantes clínicos de la capacidad para el ejercicio. Más aún, evaluamos si la
implementación del protocolo de tratamiento estandarizado postnatal influyó en la
capacidad para el ejercicio.

2- MATERIAL Y MÉTODOS
2.1 Pacientes, procedimientos y diseño del estudio
Incluimos todos los pacientes con HDC nacidos entre Enero 1999 y Mayo 2012 que
se unieron a nuestro programa prospectivo, multidisciplinario de seguimiento el
Hospital de Niños Erasmus MC- Sophia. Este programa acuerda con el estándar
actual de cuidado de niños nacidos con anomalías congénitas mayores, incluyendo
tratamiento con ECMO si es necesario. En este programa, los niños y sus padres son
seguidos por un equipo multidisciplinario, y ocho evaluaciones estandarizadas se
realizan entre las edades de 0.5 y 17 años (10, 15).
Excluimos los datos de pacientes cuya HDC fue diagnosticada después de los siete
días de edad, aquellos con defectos diafragmáticos paraesofágicos, aquellos con
una eventración diafragmática, y aquellos con discapacidades psicomotoras que no
podían realizar una prueba de ejercicio máximo cardiopulmonar. Hasta Noviembre
2 TABLA 1 Características de los pacientes
Antecedentes Edad gestacional (semanas) Peso al nacer (kg) Varón (%) Etnia Holandés (%) Otro (%) Hernia izquierda (%) Parche (%) Diás de VM Días sin VM a Tipo de VM inicial Convencional Alta frecuencia No VM Sin dato Días en UCI Días de Hospital inicial DBP (%) No Leve Moderada Severa Sin dato Cardiopatía congénita b Tratamiento PDES a Días sin VM en los primeros 28 días de vida
b Cardiopatía congenital: : Defecto septal ventricular (n = 1), Defecto septal atrial (n = 2), Defecto septal ventricular y septal atrial (n = 1),
Doble tracto de salida de ventrículo derecho+ transposición de los grandes vasos+ Foramen oval abierto+ Ductus abierto (n = 1), Ductus Botalli
abierto + Foramen Oval abierto + Insuficiencia tricuspidea y mitral (n = 1), Ductus Botalli abierto + Defecto Septal Atrial con cirugía (n = 2),
válvula pulmonar displásica e insuficiencia tricuspidea (n = 1).
Datos presentados como media ± desviación standard , mediana (rango interquartilo) o número (porcentaje), según corresponda. ECMO =
Oxygenación con membrane extracorpórea, Tratamiento PDE5 = tratamienot con inhibidor de phosphodiesterasa tipo 5.

de 2007, el tratamiento con ECMO fue aplicado en casos de fallo respiratorio severo
reversible usando los criterios de ingreso reportados por Stolar y otros (16).
Después de Noviembre 2007, los niños fueron tratados acorde al consenso de
protocolo de tratamiento del Consorcio EURO CDH (3) que incluyó criterios para
ECMO similares (Tabla 1 del suplemento online).
Un pediatra y un cirujano pediátrico realizaron el examen físico estandarizado. La
capacidad para el ejercicio fue evaluada por un terapista físico experto. Información
estandarizada (tipo y frecuencia de participación en deportes distinto de gimnasia)
fue registrada como participación en deportes. Previo a la prueba de ejercicio, los
padres estimaron el nivel de capacidad de sus hijos como superior, igual o menor
que la de los niños de su misma edad. Las características perinatales y demográficas
fueron obtenidas de los registros médicos.
El Comité de Ética Médica del Erasmus MC determinó que las reglas establecidas en
el Acta de Investigación Médica en Sujetos Humanos no aplicaban para esta
propuesta de investigación (MEC- 2016- 111). Los padres de todos los niños fueron
informados de rutina acerca del estudio y proveyeron permiso para utilizar los
datos con fines de investigación.
2.2 Medidas
2.2.1 Datos basales
Fueron registrados los siguientes datos basales: sexo, edad, edad gestacional (EG),
peso de nacimiento (PN), raza, lado de la hernia, tipo de reparación, duración de
ventilación mecánica, días libres de ventilación en los primeros 28 días de vida, tipo
de ventilación mecánica inicial, duración de la estadía en cuidados intensivos (UCI),
duración de la internación inicial, presencia de enfermedad pulmonar crónica
(EPOC) (17), anomalías cardíacas congénitas, tratamiento con inhibidor de
fosfodiesterasa tipo 5, y participación en deportes. Además, evaluamos función
pulmonar. El volumen espiratorio forzado en 1 segundo (VEF1) fue determinado con
un espirómetro electrónico (Masterscreen PFT, Carefusion, San Diego, CA) después
de la inhalación de 400 µg de salbutamol (18) y expresado como valor absoluto y
como SDS (19). La capacidad pulmonar total (CPT) fue determinada por
pletismografía corporal total (Masterscreen Body Pletismography, Carefusion, San
Diego, CA) y expresada en valor absoluto y score de percentilo. La capacidad de
difusión corregida para volumen alveolar (KCO) fue medida utilizando un analizador
multigas (Masterscreen PFT, Carefusion, San Diego, CA) por el método de
respiración única. Los scores de percentilos para volúmenes pulmonares y
capacidad de difusión obtenida por ecuaciones de referencia de Koopman et al (20)
fueron transformados en SDS empleando una transformación inversa normal.
2.2.2 Capacidad de ejercicio

Todos los niños realizaron una prueba de capacidad máxima de ejercicio
cardiopulmonar después de examinar la función pulmonar, es decir, 1-2 horas
después de inhalar salbutamol, si aplicaba. Por lo tanto, evaluamos sólo función
pulmonar después de broncodilatación (BD). La prueba máxima de ejercicio
cardiopulmonar fue realizada sobre cinta a motor (En Mill; Enraf Nonius, Rotterdam,
Netherlands), programada para aumentos en ángulo de inclinación y velocidad
acordes al protocolo de Bruce 21, 22). Los niños fueron instados a trabajar hasta
quedar exhaustos. El mayor tiempo de resistencia (en minutos, con un decimal)
sirvió como criterio para la capacidad de ejercicio, con el SDS basado en los valores
de referencia de los niños holandeses sanos (21, 22). La frecuencia cardíaca y la
saturación transcutánea de oxígeno fueron monitoreados antes y durante la prueba
con un oxímetro de pulso (MARS (MOtion Artifact Reduction System), tipo 2001;
Respironics Novametrix, Murrysville, PA). La frecuencia cardíaca de ≥ 185 por min
(23) o la pérdida de coordinación debido a excesiva fatiga se tomó como
desempeño máximo.
2.3 Análisis estadístico
Las diferencias en datos basales entre “participantes en el programa de
seguimiento” y “no- participantes en el programa de seguimiento” y los niños
“tratados con ECMO neonatal” y “no tratados con ECMO neonatal”) fueron
evaluadas empleando tests Mann- Whitney U para variables continuas y chi
cuadrado para variables categóricas. T-test de una muestra fueron empleados para
probar si los datos de capacidad de ejercicio que se distribuían normalmente
diferían de las normas poblacionales (SDS= 0). Para testear si la capacidad de
ejercicio difería entre pacientes ECMO- HCD y No ECMO, se aplicaron t-tests de
muestras independientes. La evaluación longitudinal de los tiempos de resistencia a
los 5, 8, y 12 años de edad fue realizada utilizando modelos mixtos lineares, que
pueden representar correlaciones intra-sujeto y permiten valores perdidos en la
variable dependiente (24). Para investigar si las características perinatales y
demográficas tuvieron una influencia significativa en el SDS de tiempo de
resistencia, consideramos la siguiente lista de datos basales en el modelo mixto
linear como co-variables: EG, tratamiento ECMO, utilización de un protocolo
estandarizado de tratamiento (después de Noviembre de 2007), reparación con
parche, duración de la estadía hospitalaria inicial, días libre de VM en los primeros
28 días de vida, tipo de VM inicial, malformación cardíaca congénita, y participación
en deportes. Empleamos un enfoque paso a paso hacia atrás para seleccionar co-
variables de esta lista de datos basales. Efectos de interacción de dos vías fueron
agregados al modelo resultante si el efecto de interacción era estadísticamente
significativo. Los resultados de los modelos lineares mixtos son reportados
empleando medias marginales estimadas, que son los valores predictivos de la
variable dependiente ajustada por el efecto de las co-variables. Para investigar si los

parámetros de la función pulmonar (FEV1, TLC, KCO) tuvieron una influencia
significativa sobre el SDS del tiempo de resistencia, sólo se emplearon los datos de
capacidad de ejercicio a los 8 y 12 años, ya que la función pulmonar no fue medida
a la edad de 5. Por lo tanto, modelos mixtos lineares separados fueron
desarrollados con la lista mencionada más arriba de los datos basales y FEV1, TLC,
KCO como co-variables a los 8 y 12 años de edad. Multicolinearidad fue determinada
utilizando factores de inflación de la varianza (VIFs). VIFs ≤ 5.0 fueron considerados
aceptables, mientras que valores más altos fueron tomados como signos de
multicolinearidad. La correlación de rango de Spearman fue usada para testear si
los niveles de capacidad de ejercicio estimados por los padres estaban asociados
con el SDS de tiempo de resistencia medido.
Los análisis se realizaron con SPSS 21.0 (IBM, Chicago, IL), y todos los tests
estadísticos emplearon un nivel de significación doble de 0.05.
3 RESULTADOS
3.1 Pacientes
Entre Enero 1999 y Julio 2012, 234 niños nacieron con HDC en el Hospital de Niños
Erasmus MC- Sophia. Sesenta y cinco (27.7%) fallecieron antes del egreso
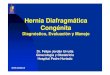
hospitalario (Figura 1). Cincuenta y cinco (32.4%) de los 169 sobrevivientes fueron
excluidos por varias razones (Figura 1). Entonces, 114 (67.1%) realizaron el
protocolo Bruce (220 mediciones). Excluimos los resultados de 29 mediciones
(13.8%) debido a que no se alcanzó el máximo desempeño (Figura 1). El análisis
para este estudio abarcó 191 pruebas confiables realizadas por 107 niños (62.9% de
todos los sobrevivientes) de los cuales 30 (28.0%) recibieron tratamiento con ECMO.
Las características de los pacientes son presentadas en la Tabla 1. La duración de
VM, días libres de ventilación en los primeros 28 días de vida, internación en UCI y
duración de la estadía inicial hospitalaria fueron significativamente diferentes en
niños con y sin ECMO. También la presencia de EPOC, tratamiento con inhibidor de
fosfodiesterasa tipo 5, y FEV1 después de BD (a los 8 años de edad) fueron
significativamente diferentes entre estos grupos (Tabla 1). No hubo diferencias en
las características de base, excepto etnicidad (p= 0.001) y PN (p= 0.030), entre
participantes y no participantes de nuestro programa de seguimiento (datos no
mostrados).
3.2 Capacidad de ejercicio
El SDS medio marginal estimado (IC 95%) de tiempo de resistencia estuvo
significativamente debajo de la norma en todas las edades<<<<<<<<<<<. 5
años:-0.44 (-0.65 a -0.24); 8 años: - 1.01 (-1.23 a – 0.78); 12 años: -1.10 (-1.40 a -
0.80) (todos p <0.001) (Tabla 3). La media (DS) de FC en el máximo ejercicio fue 191

(9.0) latidos por minuto y la media (RIQ) de saturación de Oxígeno transcutáneo en
el ejercicio máximo fue 98% (96-99). La capacidad de ejercicio decreció
significativamente desde las edades de 5 a 8 años (p< 0.001) y desde 5 a 12 años
(p<0.001) (Tabla 2 del suplemento online).
3.3 Pacientes HDC ECMO versus Pacientes HDC no-ECMO
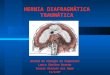
La capacidad para el ejercicio difirió significativamente entre pacientes tratados con
ECMO y los no tratados con ECMO (diferencia media (IC 95%) 0.421 (0.117 a 0.724,
p= 0.007), particularmente a la edad de 8 (p= 0.036). La capacidad para ejercicio
declinó significativamente en pacientes tratados con ECMO desde los 5 a los 8 años
(p= 0.001) y desde los 5 a los 12 años (p= 0.006). Esta declinación también se vio en
pacientes no tratados con ECMO; desde los 5 a 8 años (p= 0.008) y 5 a 12 años (p=
0.015) (Tabla 3, Figura 2, Tabla 2 del suplemento online).
3.4 Asociaciones entre capacidad de ejercicio y datos basales
La capacidad para el ejercicio estuvo significativamente asociada en forma negativa
con la duración inicial de la estadía hospitalaria (coeficiente estimado (IC 95%) -
0.006 (-0.009ª 0.003), p< 0.001) y positivamente con KCO (coeficiente estimado (IC
95%) 0.27 (0.01 a 0.53), p= 0.039). No se encontraron otras asociaciones
significativas entre la capacidad para ejercicio y el momento de la prueba, EG, uso
de un nuevo protocolo de tratamiento, reparación con parche, días sin VM en los
primeros 28 días de vida, tipo de VM inicial, malformación cardíaca congénita, FEV1,
TLC, y participación en deportes (Tabla 3 del suplemento online). Pese a que la
capacidad de ejercicio difirió significativamente entre pacientes tratados con ECMO
y no-tratados- con menor capacidad de ejercicio en pacientes ECMO- ECMO no
tuvo efecto significativo en el deterioro de la capacidad de ejercicio: no se encontró
efecto de interacción entre ECMO y el momento de de examen de la capacidad
para ejercicio (p= 0.363). Para ambos grupos se observó la misma tendencia de
deterioro (Figura 2).
Todos los VIFs fueron ≤3.1.
3.5 Capacidad de ejercicio estimada por padres
Los niveles de capacidad para el ejercicio estimados por los padres se
correlacionaron positivamente con el SDS de tiempo de resistencia medido (r=
0.420, p< 0.001)
4 DISCUSIÓN
Evaluamos longitudinalmente la capacidad máxima para ejercicio en niños con HDC
en edades de 5 a 12 años. La capacidad para ejercicio fue significativamente inferior
a la norma en todas las edades, y declinó significativamente en el tiempo- no sólo

en niños tratados con ECMO sino también en aquellos que no requirieron ECMO. La
duración de la hospitalización inicial y la capacidad de difusión de los pulmones
estuvieron asociadas con la capacidad para el ejercicio.
El tratamiento de neonatos con HDC es un desafío y las estrategias terapéuticas
han cambiado a través de las décadas. Esto ha resultado en disminución de las
tasas de mortalidad (2, 25), y desarrollo de estrategias de protección del pulmón,
por ejemplo, ventilación gentil con hipercapnia permisiva (26). Por lo tanto, es difícil
comparar los datos de nuestra población con los de aquellos que sobrevivieron
hace 20 años (8, 12- 14, 27, 28).

FIGURA 1 Flujograma de selección de la población. a Aberración Cromosómica (n = 2), síndrome de Cohen (n = 1), síndrome de Loeys-Dietz (n = 1), síndrome de Simpson-Golabi-Behmel (n = 3), síndrome de Wolf-Hirschhorn (n = 1), autismo (n = 3). bHemiplejia (n = 3), aorta-estenosis (n = 1), cánula traqueal (n = 1), severo EPOC (n = 1), razones organizacionales (n = 2), ansiedad (n = 1). cPérdida de coordinación (n = 7), ansiedad (n = 7), rechazo (n = 2), no desempeño máximo (n = 10), cordones de calzado sueltos (n = 1), insuficiente lenguaje holandés (n = 1), dolor muscular de pantorrillas (n = 1). HDC: hernia diafragmática congénita; ECMO = oxigenación con membrana extracorpórea
Previamente encontramos capacidad para ejercicio disminuida en niños de 5 años con
HDC, independiente de haber sido tratados con ECMO (10). En otro estudio, en niños
con diferentes diagnósticos subyacentes, que habían sido todos tratados con ECMO,
mostramos que la capacidad máxima para el ejercicio estuvo debajo de la norma a los
Pacientes HDC ingresados entre Enero 1999- Mayo 2012 N=234
Fallecidos n= 65
Sobrevivientes con HDC N= 169
Perdidos para seguimiento o rechazos: n=14 Diagnóstico tardío: n=14 Eventración: n=14 Hernia paraesofágica: n=3 Retardo psicomotor/síndrome: 11 a
Incapacidad de realizar prueba de ejercicio: n=9 b
Pacientes HDC elegibles N= 114 niños (220 mediciones)
Excluidos: 29 pruebas de ejercicio no confiables
107 niños (191 pruebas de ejercicio confiables)
Sólo 5 años: n=35 Sólo 8 años: n=7
Sólo 12 años: n= 1 5 y 8 años: n= 30 5 y 12años: n= 2
8 y 12 años: n=12
5, 8 y 12 años: n=20
30 pacientes HDC tratados con ECMO (67 pruebas confiables de ejercicio)
77 pacientes HDC tratados sin ECMO (124 pruebas confiables de ejercicio)

5, 8, y 12 años y se deterioró a lo largo del tiempo (11). Muchos niños en aquella
cohorte habían nacido a principios de los ´90 (11). Pese a las diferencias en la población
en estudio, un curso similar de deterioro de la capacidad para el ejercicio fue
observado en el estudio actual. Estos hallazgos sugieren que la capacidad para el
ejercicio debería ser evaluada en la infancia y adolescencia, e inclusive en la adultez.
Persiste el interrogante, sin embargo, si la intervención oportuna indicada por el
resultado de la evaluación puede mejorar o al menos prevenir el deterioro. Estimular
que los niños adhieran a la actividad física podría ayudar a prevenir morbilidades
secundarias. Consejería pro-activa por parte de los profesionales y derivación temprana
a terapistas físicos puede ser muy útil.
TABLA 2 Características en las evaluaciones de Seguimiento
a Despúes de la evaluación el paciente fue derivado a terapia física pediátrica en su localidad para iniciar intervención bDespués de la evaluación se recomendó al paciente continuar la intervención con terapia física pediátrica en su comunidad. Los datos se presentan como mediana (rango intercuartilo) o número (porcentaje) según corresponda. ECMO: oxigenación con membrana
extracorpórea
La introducción del protocolo de tratamiento postnatal del Consorcio EURO CDH
llevó a un aumento de la sobrevida de niños nacidos con HDC (3). Este protocolo
fue implementado en nuestro departamento en Noviembre de 2007. La
estandarización del manejo postnatal ha resultado en menor mortalidad pero no en
menor prevalencia de EPOC (2). Esto sugiere que más pacientes con HDC que
desarrollan EPOC sobreviven, lo cual puede afectar la capacidad máxima de
ejercicio. Sin embargo, no pudimos demostrar un efecto significativo de la
introducción del protocolo en el tiempo máximo de resistencia. (Tablas 3 y 4 del
suplemento online). El efecto del mejor cuidado intensivo podría haber sido
contrabalanceado por una mayor prevalencia de sobrevivientes con EPOC.
Números más grandes de niños deberían ser estudiados a los 8 y 12 años para
demostrar un posible efecto de la implementación del protocolo de tratamiento en
la capacidad de ejercicio.
En Seguimiento 5 años de edad Participación deportiva (%) Derivación a TF a (%) Continúa en TF b (%) 8 años de edad SDS FEV 1 SDS TLC SDS KCO Participación deportiva (%) Derivación a TF a (%) Continúa en TF b (%) 12 años de edad SDS FEV 1 SDS TLC SDS KCO Participación deportiva (%) Derivación a TF a (%) Continúa en TF b (%)
0.180 0.717

Asumimos que los niños con la hipoplasia pulmonar más severa, podrían estar en
máximo riesgo para capacidad de ejercicio deficitaria. Inclusive, niños que han sido
tratados con ECMO tuvieron significativamente mayor obstrucción al flujo de aire y
menor SDS del tiempo de resistencia. Interesante, KCO estuvo significativamente
debajo de la norma en los niños tratados y no tratados con ECMO y estuvo
asociada positivamente con la capacidad de ejercicio, mientras que el tratamiento
con ECMO no estuvo asociado con la capacidad de ejercicio. Especulamos que los
cambios microestructurales de los pulmones, que han sido descriptos en adultos
jóvenes con HDC (6), pueden ya ocurrir a edad más joven. Futuros estudios
enfocados en la imagen de la estructura del pulmón pueden ser útiles para
identificar pacientes en riesgo de deterioro clínico y deficitaria tolerancia al
ejercicio. La asociación entre la duración de la estadía inicial en el hospital y la
capacidad para el ejercicio que hemos encontrado sugiere que los neonatos más
críticamente enfermos con los problemas pulmonares más severos son más
proclives a sufrir de morbilidad pulmonar persistente más tarde en la vida.
Además, especulamos que los padres de niños que han estado críticamente
enfermos en el período neonatal pueden considerar a sus hijos más vulnerables que
los padres de niños sanos. Por esta razón, y también porque la morbilidad
pulmonar persiste por años (4, 5), los padres pueden no estimular las actividades
físicas. Esto puede, a su vez, ponerlos en riesgo de problemas en el área motora
gruesa (29, 30) y consiguientemente menor participación en actividades físicas.
Smith et al encontraron problemas similares en niños nacidos muy pretérmino. La
capacidad de ejercicio reducida no pudo ser explicada por obstrucción al flujo de
aire. Por tanto, estos autores también plantearon la hipótesis de que los niños
nacidos muy PT eran desalentados y que la falta de actividad física podía tener un
rol (31). Pese a que en nuestro estudio el tratamiento con ECMO no tuvo influencia
significativa sobre la capacidad para ejercicio disminuida y su deterioro, asumimos
que la menor capacidad para el ejercicio en pacientes con HDC tratados con ECMO,
asumimos que la capacidad menor de ejercicio en pacientes HDC tratados con
ECMO podría ser explicada por el hecho de que estos pacientes son los niños más
críticamente enfermos en la edad neonatal con hipoplasia pulmonar más severa,
mayor obstrucción al flujo de aire, y menor participación en actividades físicas.

TABLE 3 Tiempo de Resistencia en pacientes HDC tratados con y sin ECMO
Los datos se presentan como media marginales estimadas (IC 95%) del SDS del tiempo de Resistencia. Significativamente debajo de la norma poblacional (SDS= 0): aP ≤ 0.001; bP = 0.004.
FIGURA 2 Cambio en la capacidad maxima de ejercicio en el tiempo en niños con HDC. Datos mostrados son las medias marginales estimadas a partir del análisis de modelo mixto linear con IC 95%. HDC: hernia diafragmática congénita; ECMO = oxigenación con membrana extracorpórea; SDS = score de desviación standard
Siguiendo este razonamiento, el deterioro en la capacidad de ejercicio entre las
edades 5 y 8, y su estabilización desde los 8 años, podría quizás ser parcialmente
explicada por la participación en deportes. A la edad de 8 y 12 alrededor de dos
tercios de los niños participaban en deportes versus sólo la mitad a la edad de 5.
Presumiblemente, los padres consideran a sus hijos en los primeros años de vida
más vulnerables y son reacios a estimular a sus hijos para actividades físicas diarias
y participación en deportes.
Las principales fortalezas de este estudio son el diseño longitudinal dentro de una
infraestructura de un programa de seguimiento estandarizado, la pequeña
proporción de niños perdidos para seguimiento y el relativamente grande tamaño
muestral para esta anomalía congénita rara. Algunas limitaciones deben ser
señaladas. No todos los niños participantes en el programa de seguimiento han
alcanzado aún la edad de 12 años. El número resultante de pocos niños evaluados a
los 12 años aumenta la probabilidad de error tipo II, pese a que los modelos mixtos
HDC sin ECMO HDC con ECMO
Edad (años)
T I E M P O De R E S I S T E N C I A S D S
años años años
Total pacientes HDC, n= 107 ECMO, n= 31 No-ECMO, n= 71

dan cuenta de datos faltantes al azar. Segundo, el manejo postnatal de HDC cambió
durante el período en estudio, lo cual podría haber influenciado nuestros resultados
en la medida que más niños con hipoplasia pulmonar severa sobrevivieron después
de la introducción del protocolo de tratamiento postnatal. No encontramos un
efecto significativo de la introducción del protocolo de tratamiento postnatal sobre
la capacidad de ejercicio (Tablas 3 y 4 del suplemento online), pero tamaños
muestrales mayores de niños de 8 y 12 años pueden ser necesarios para detectar
una diferencia significativa. Tercero, empleamos el tiempo de máxima resistencia en
lugar del consumo pico de oxígeno como medida de la capacidad para el ejercicio,
principalmente por razones de factibilidad. Utilizar una máscara puede llevar a
pérdida de colaboración y a resultados sub-máximos, especialmente en niños más
pequeños. Una fuerte correlación entre la máxima resistencia y el máximo consumo
de oxígeno ha sido reportada por Cummings y colaboradores (32). Además, dado
que nuestro sitio es una clínica de pacientes ambulatorios y no un establecimiento
de investigación, pensamos que la prueba de ejercicio cardiopulmonar (CPX), que
incluye análisis de gas respiratorio, es demasiado intensiva para ser realizada en
todos los pacientes HDC durante el seguimiento de rutina. En futuros proyectos de
investigación en nuestro departamento, CPX será evaluado en niños, y las
conclusiones acerca de la capacidad de ejercicio en pacientes HDC podrían
extenderse. Cuarto, no incluimos un grupo de controles sanos, Sin embargo,
empleamos datos recolectados de referencia recientemente establecidos en
nuestro propio centro (21, 22). Quinto, no tenemos datos de actividad física. La
actividad física reducida pudría ser una de las explicaciones para la reducida
capacidad de ejercicio en niños con HDC y es objeto de un proyecto de
investigación continua en nuestro centro. Finalmente, considerando la gran
cantidad de posibles determinantes de la capacidad de ejercicio, así como la
posibilidad de multicolinearidad tuvimos que ser críticos en cuanto a qué
parámetros de función pulmonar incluir como posibles determinantes en el modelo
mixto de análisis. En un estudio transversal de Peetsold et al (5), la capacidad para
el ejercicio y la función pulmonar fue medida en niños de edad escolar nacidos con
HDC y derivados a el Paediatric Surgical Centre de Amsterdam (Holanda) entre
1987 y 1999, y a nuestro centro entre 1988 y 1994. No mostraron asociaciones
entre VO2 máxima y parámetros de función pulmonar, excepto para FEV1 (R2= 0.27;
p= 0.001). En otro estudio de nuestro grupo de investigación ninguno de los
parámetros de función pulmonar, sino DLCO estuvo relacionado con el % pico VO2
predominante en pacientes HDC adultos jóvenes (14). Por lo tanto, como la
multilinearidad surgió entre los parámetros de función pulmonar en este estudio,
nosotros críticamente elegimos incluir sólo FEV1, TLC y KCO en el modelo mixto de
análisis.
Las diferencias significativas en etnicidad y PN entre los participantes y los no-
participantes en este estudio estuvo en línea con las expectativas. Encontramos un

porcentaje más alto de otras etnias distintas de la holandesa y menor PN en el
grupo no-participante. Los padres y niños holandeses nativos mostraron mayor
adherencia al seguimiento y al tratamiento que los padres de otras etnias (33). Las
diferencias en PN entre etnias son comunes (34). Sin embargo, continuaremos con
nuestras estrategias para aumentar la adherencia en padres y niños no-nativos en
nuestro programa de seguimiento. Las características de base que reflejan
severidad de la enfermedad no difirieron entre los participantes y no-participantes
(datos no mostrados). No parece haber sesgo de selección.
5 CONCLUSIÓN
Los pacientes HDC estuvieron en riesgo para capacidad de ejercicio disminuida en
la edad escolar. La capacidad disminuida para el ejercicio se deterioró con el
tiempo, no sólo en niños que requirieron tratamiento neonatal con ECMO sino
también en niños que no necesitaron ECMO. La capacidad de ejercicio estuvo
significativamente asociada negativamente con la duración de la estadia
hospitalaria inicial y positivamente con KCO. La estratificación de riesgo temprano
para capacidad para el ejercicio disminuida puede ser importante para ofrecer
intervención oportuna. Son necesarios mayores estudios para develar las causas de
la capacidad física disminuida. Recomendamos seguimiento a largo prolongado,
aconsejar por-activamente sobre actividades físicas y participación en deportes o
derivación a terapista físico.
REFERENCIAS
1.Ackerman KG, Pober BR. Congenital diaphragmatic hernia and pulmonary hypoplasia: new
insights from developmental biology and genetics. Am J Med Genet C Semin Med Genet.
2007;145C:105–108.
2. Van Den Hout L, Schaible T, Cohen-Overbeek TE, et al. Actual outcome in infants with
congenital diaphragmatic hernia: the role of a standardized postnatal treatment protocol. Fetal
Diagn Ther. 2011;29:55–63.
3. Reiss I, Schaible T, van den Hout L, et al. Standardized postnatal management of infants with
congenital diaphragmatic hernia in Europe: the CDH EURO Consortium consensus. Neonatology.
2010;98:354–364.
4. Spoel M, Laas R, Gischler SJ, et al. Diagnosis-related deterioration of lung function after
extracorporeal membrane oxygenation. Eur Respir J. 2012;40:1531–1537.
5. Peetsold MG, Heij HA, Nagelkerke AF, et al. Pulmonary function and exercise capacity in
survivors of congenital diaphragmatic hernia. Eur Respir J. 2009;34:1140–1147.
6. Spoel M, Marshall H, IJsselstijn H, et al. Pulmonary ventilation and micro-structural findings in
congenital diaphragmatic hernia. Pediatr Pulmonol. 2016;51:517–524.
7. Trachsel D, Selvadurai H, Adatia I, et al. Resting and exercise cardiorespiratory function in
survivors of congenital diaphragmatic hernia. Pediatr Pulmonol. 2006;41:522–529.
8. Zaccara A, Turchetta A, Calzolari A, et al. Maximal oxygen consumption and stress
performance in children operated on for congenital diaphragmatic hernia. J Pediatr Surg.
1996;31:1092-1094; discussion 1095.
9. Turchetta A, Fintini D, Cafiero G, et al. Physical activity, fitness, and dyspnea perception in
children with congenital diaphragmatic hernia. Pediatr Pulmonol. 2011;46:1000–1006.

10. Gischler SJ, van der Cammen-van Zijp MHM, Mazer P, et al. A prospective comparative
evaluation of persistent respiratory morbidity in esophageal atresia and congenital
diaphragmatic hernia survivors. J Pediatr Surg. 2009;44:1683–1690.
11. van der Cammen-van Zijp MH, Gischler SJ, Hop WC, de Jongste JC, Tibboel D, IJsselstijn H.
Deterioration of exercise capacity after neonatal extracorporeal membrane oxygenation. Eur
Respir J. 2011;38:1098–1104.
12. Marven SS, Smith CM, Claxton D, et al. Pulmonary function, exercise performance, and
growth in survivors of congenital diaphragmatic hernia. Arch Dis Child. 1998;78:137–142.
13. Peetsold MG, Vonk-Noordegraaf A, Heij HH, Gemke RJBJ. Pulmonary function and exercise
testing in adult survivors of congenital diaphragmatic hernia. Pediatr Pulmonol. 2007;42:325–
331.
14. van der Cammen-van Zijp MH, Spoel M, Laas R, et al. Exercise capacity, daily activity, and
severity of fatigue in term born young adults after neonatal respiratory failure. Scand J Med Sci
Sports. 2014;24:144–151.
15. Mazer P, Gischler SJ, Cammen-VAN Zijp VANDERMH, et al. Early developmental assessment
of children with major non-cardiac congenital anomalies predicts development at the age of 5
years. Dev Med Child Neurol. 2010;52:1154–1159.
16. Stolar CJ, Snedecor SM, Bartlett RH. Extracorporeal membrane oxygenation and neonatal
respiratory failure: experience fromthe extracorporeal life support organization. J Pediatr Surg.
1991;26:563–571.
17. Jobe AH, Bancalari EH. Controversies about the definition of bronchopulmonary dysplasia at
50 years. Acta Paediatr. 2017;106:692–693.
18. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J.
2005;26:319–338.
19. Quanjer PH, Stanojevic S, Cole TJ, et al. Multi-ethnic reference values for spirometry for the
3-95-yr age range: the global lung function 2012 equations. Eur Respir J. 2012;40:1324–1343.
20. Koopman M, Zanen P, Kruitwagen CL, van der Ent CK, Arets HG. Reference values for
paediatric pulmonary function testing: the Utrecht dataset. Respir Med. 2011;105:15–23.
21. van der Cammen-van Zijp MH, van den Berg-Emons RJ, Willemsen SP, Stam HJ, Tibboel D,
IJsselstijn H. Exercise capacity in Dutch children: new reference values for the Bruce treadmill
protocol. Scand J Med Sci Sports. 2010;20:e130–e136.
22. van der Cammen-van Zijp MHM, IJsselstijn H, Takken T, et al. Exercise testing of pre school
children using the Bruce treadmill protocol: new reference values. Eur J Appl Physiol.
2010;108:393–399.
23. Karila C, de Blic J, Waernessyckle S, Benoist MR, Scheinmann P. Cardiopulmonary exercise
testing in children − An individualized protocol for workload increase. Chest. 2001;120:81–87.
24. Fitzmaurice GM, Ware JH. Applied Longitudinal Analysis. Hoboken: John Wiley & Sons; 2004.
25. Barroso C, Correia-Pinto J. Thoracoscopic repair of congenital diaphragmatic hernia, review
of the results. Minerva Pediatr. 2017;70:281–288.
26. Wung JT, Sahni R,Moffitt ST, Lipsitz E, Stolar CJ. Congenital diaphragmatic hernia: survival
treated with very delayed surgery, spontaneous respiration, and no chest tube. J Pediatr Surg.
1995;30:406–409.
27. IJsselstijn H, Tibboel D, Hop WJ, Molenaar JC, de Jongste JC. Longterm pulmonary sequelae
in children with congenital diaphragmatic hernia. Am J Respir Crit Care Med. 1997;155:174–180.
28. Montgomery MFB, Freyschuss U, Mortensson W. Long-term-follow up of respiratory
function, maximal working capacity, and esophageal function. Pediatr Surg Int. 1995;10:519–522.
29. van der Cammen-van Zijp MHM, Janssen AJ, Raets MM, et al. Motor performance after
neonatal extracorporeal membrane oxygenation: a longitudinal evaluation. Pediatrics. 2014;134:
427–435.
30. Madderom MJ, Toussaint LCC, van der Cammen-van Zijp MHM, et al. Congenital
diaphragmatic hernia with(out) ECMO: impaired development at 8 years. Arch Dis Child Fetal
Neonatal Ed. 2013;98:316–322.

31. Smith LJ, van Asperen PP, McKay KO, Selvadurai H, Fitzgerald DA. Reduced exercise capacity
in children born very preterm. Pediatrics. 2008;122:287–293.
32. Cumming GR, Everatt D, Hastman L. Bruce treadmill test in children: normal values in a clinic
population. Am J Cardiol. 1978;41:69–75.
33. Dahhan N, Meijssen D, Chegary M, Bosman D, Wolf B. Ethnic diversity outpatient clinic in
paediatrics. BMC Health Serv Res. 2012;12:12.
34. Troe EJ, Raat H, Jaddoe VW, et al. Explaining differences in birthweight between ethnic
populations. The Generation R Study. BJOG. 2007;114:1557–1565.

Received: 4 May 2018 | Revised: 27 September 2018 | Accepted: 20 November 2018
DOI: 10.1002/ppul.24264
ORIGINAL ARTICLE: OUTCOMES
Congenital diaphragmatic hernia and exercise capacity, alongitudinal evaluation
Leontien C.C. Toussaint-Duyster MPPT1,2 |
Monique H.M. van der Cammen-van Zijp PhD1,2 | Johan C. de Jongste MD, PhD3 |
Dick Tibboel MD, PhD1 | Rene M.H. Wijnen MD, PhD1 |
Saskia J. Gischler MD, PhD1 | Joost van Rosmalen PhD4 |
Hanneke IJsselstijn MD, PhD1
1Department of Pediatric Surgery and
Intensive Care, Erasmus MC-Sophia Children's
Hospital, Rotterdam, the Netherlands
2Department of Orthopedics, Section of
Physical Therapy, Erasmus MC-Sophia
Children's Hospital, Rotterdam, the
Netherlands
3Department of Pediatrics, Division of
Respiratory Medicine, Erasmus MC-Sophia
Children's Hospital, Rotterdam, the
Netherlands
4Department of Biostatistics, Erasmus
Medical Center, Rotterdam, the Netherlands
Correspondence
Hanneke IJsselstijn, MD PhD, Intensive Care
and Department of Pediatric Surgery, Erasmus
MC—Sophia Children's Hospital, Rotterdam,
the Netherlands.
Email: [email protected]
Abstract
Objective:Childrenwith congenital diaphragmatic hernia (CDH) suffer from long-term
pulmonary morbidity. Longitudinal data of exercise capacity in these children are
lacking. We hypothesized that exercise capacity would be impaired in children with
CDH and deteriorates over time.We evaluated exercise capacity and its determinants
in CDH patients longitudinally until 12 years of age.
Design: Prospective longitudinal follow-up study in tertiary university hospital.
Patients:Onehundred and fourteen childrenwith CDHborn between 1999 and 2012.
Methods: Exercise capacity was evaluated using the Bruce treadmill-protocol at the
ages of 5, 8, and 12 years. Primary outcome parameter was standard deviation score
(SDS) of maximal endurance time. Data were analyzed by using linear mixed models.
Results:Atotal of 107children (30 treatedwithextracorporealmembraneoxygenation
[ECMO]) performed 191 reliable exercise tests. At ages 5, 8, and 12 years, the mean
(95%CI) SDSendurance timewas−0.44 (−0.65 to−0.24);−1.01 (−1.23 to−0.78);−1.10
(−1.40 to −0.80), respectively, all less than zero (P < 0.001). Exercise capacity declined
significantly over time irrespective of ECMO-treatment (5-12 years: non-ECMO
P = 0.015; ECMO P = 0.006). Duration of initial hospital stay and diffusion capacity
corrected for alveolar volumewere associatedwith SDSendurance time (P < 0.001 and
P = 0.039).
Conclusions: InCDHpatients exercise capacity deteriorates between5and12years of
age, irrespective of ECMO-treatment. CDH patients may benefit from long-term
assessments of exercise capacity with timely intervention.
K E YWORD S
child, congenital diaphragmatic hernia, exercise capacity, extracorporeal membrane
oxygenation, follow-up, school-age
This is an open access article under the terms of the Creative Commons Attribution-NonCommercial License, which permits use, distribution and reproduction in
any medium, provided the original work is properly cited and is not used for commercial purposes.
© 2019 The Authors. Pediatric Pulmonology Published by Wiley Periodicals, Inc.
Pediatric Pulmonology. 2019;1–9. wileyonlinelibrary.com/journal/ppul | 1

1 | INTRODUCTION
Congenital diaphragmatic hernia (CDH) occurs in 1 in 3000-4000
births.1 Although CDH is still a life-threatening anomaly, survival rates
have increased over the past decades.2 Advances in surgical and
neonatal management, as well as the implementation of a standardized
European neonatal treatment protocol in November 20073 (Table 1 of
the online supplement), have significantly contributed to higher survival
rates2 which turned out to be sustainable over time and inmany centers
around theworld.With the increased survival, more childrenmay suffer
from long-term morbidities, including pulmonary symptoms. Factors
that may contribute to long-term pulmonary morbidity are lung
hypoplasia with persistent airflow obstruction,4,5 iatrogenic lung
damage due to mechanical ventilation,4 and microstructural changes
in the lung.6 These pulmonary abnormalities may lead to decreased
exercise capacity on the long-term and affect development in later life.
While several studies found decreased exercise capacity in CDH
patients at school-age,7–11 a few other studies showed normal exercise
capacity in school-aged5,12 and inadultCDHpatients.13,14These studies
had mostly a cross-sectional study design, small sample sizes, and
included patients born before a standardized postnatal treatment
protocolbecameavailable.A longitudinalevaluationofexercisecapacity
in CDH patients has not been performed to date.
Therefore, the aim of the present study was to evaluate
longitudinally exercise capacity at the ages of 5, 8, and 12 years in a
large cohort of CDH patients treated with or without neonatal
extracorporeal membrane oxygenation (ECMO). Secondarily, we
aimed to find clinical determinants of exercise capacity. Furthermore,
we evaluated whether the implementation of a standardized postnatal
treatment protocol influenced exercise capacity.
TABLE 1 Patient characteristics
Background Total n = 107 ECMO n = 30 non-ECMO n = 77 P
Gestational age (weeks) 38.6 ± 1.9 39.0 ± 1.6 38.4 ± 2.1 0.105
Birth weight (kilograms) 3.0 ± 0.6 3.2 ± 0.4 3.0 ± 0.6 0.154
Male (%) 62 (57.9) 20 (66.7) 42 (54.5) 0.254
Ethnicity 0.331
Dutch (%) 88 (82.2) 23 (76.7) 65 (84.4)
Other (%) 19 (17.8) 7 (23.3) 12 (15.6)
Left-sided hernia (%) 93 (86.9) 27 (90.0) 66 (85.7) 0.555
Patch repair (%) 75 (70.1) 26 (86.7) 49 (63.6) 0.019
Days of mechanical ventilation 11 (6-22) 29 (16-48) 8 (5-16) <0.001
Ventilator-free daysa 17 (6-22) 0 (0-12) 20 (12-23) <0.001
Type of initial mechanical ventilation 0.811
CMV 45 (42.1) 12 (40.0) 33 (42.9)
HFO 59 (55.1) 17 (56.7) 42 (54.5)
No ventilation 1 (0.9) – 1 (1.3)
Missing 2 (1.9) 1 (3.3) 1 (1.3)
Days of ICU stay 20 (13-42) 52 (29-80) 16 (10-27) <0.001
Days of initial hospital stay 36 (20-61) 80 (36-102) 27 (27-50) <0.001
Bronchopulmonary dysplasia (%) <0.001
No 68 (63.6) 11 (36.7) 57 (74.0)
Mild 16 (15.0) 3 (10.0) 13 (16.9)
Moderate 4 (3.7) 3 (10.0) 1 (1.3)
Severe 17 (15.9) 13 (43.3) 4 (5.2)
Missing 2 (1.8) – 2 (2.6)
Congenital heart diseaseb 9 (8.8) 5 (16.7) 4 (5.2) 0.055
PDE5 treatment 13 (12.1) 9 (30.0) 3 (3.8) <0.001
aVentilator-free days in the first 28 days of life.bCongenital heart disease: Ventricle SeptumDefect (n = 1), Atrium SeptumDefect (n = 2), Ventricle SeptumDefect and Atrium SeptumDefect (n = 1), DoubleOutlet Right Ventricle + transposition blood vessel + Open Foramen Ovale + Open Ductus Botalli (n = 1), Open Ductus Botalli + Open ForamenOvale + tricuspidalis and mitral insufficiency (n = 1), Open Ductus Botalli + Atrium Septum Defect with surgery (n = 2), dysplastic pulmonic valve and
tricuspidalis insufficiency (n = 1).Data are presented as mean ± standard deviation, median (interquartile range) or number (percentage), as appropriate. ECMO= extracorporeal membraneoxygenation, PDE5 treatment = treatment with phosphodiesterase type 5 inhibitor.
2 | TOUSSAINT-DUYSTER ET AL.

2 | MATERIALS AND METHODS
2.1 | Patients, procedures, and study design
We included all CDH patients born between January 1999 and
May 2012 who joined our prospective, multidisciplinary follow-up
program at the Erasmus MC-Sophia Children's Hospital. This program
conforms to the present standard of care for children born with major
anatomical congenital anomalies, including ECMO treatment if
needed. In this program, the children and their parents are followed
by a multidisciplinary team, and eight standardized assessments are
performed between 0.5 and 17 years of age.10,15
We excluded data from patients diagnosed with CDH after seven
days of age, those with paraesophageal diaphragmatic defects, those
with a diaphragmatic eventration, and those with psychomotor
disabilitieswho could not perform amaximal cardiopulmonary exercise
test. Until November 2007, ECMO treatment was applied in cases of
reversible severe respiratory failure by using the entry criteria reported
by Stolar et al.16 After November 2007, children were treated
according to the standardized CDH EURO Consortium consensus
treatment protocol3 which included similar ECMO criteria (Table 1 of
the online supplement).
A pediatrician and a pediatric surgeon performed standardized
physical examination. Exercise capacity was evaluated by an experi-
enced pediatric physical therapist. Standardized information (type and
frequency of sports participation other than gymnastics) was recorded
about sports participation. Prior to the exercise test, parents estimated
their child's fitness level as higher, equal to or less than that of children
with the same age. Perinatal and demographic characteristics were
retrieved frommedical records. The last included patient was tested in
July 2017.
The Medical Ethics Committee of the Erasmus MC stated that the
rules laid down in theMedical Research Involving Human Subjects Act
and did not apply to this research proposal (MEC-2016-111). Parents
of all children were routinely informed about the study and provided
permission to use the data for research purposes.
2.2 | Measurements
2.2.1 | Baseline data
The following baseline data were recorded: gender, age, gestational
age, birth weight, ethnicity, side hernia, type of repair, duration of
mechanical ventilation, ventilation-free days in the first 28 days of life,
type of initial mechanical ventilation, duration of intensive care unit
(ICU) stay, duration of initial hospital stay, presence of chronic lung
disease (CLD),17 congenital cardiac anomalies, treatment with
phosphodiesterase type 5 inhibitor, and sports participation. More-
over, we assessed lung function. Forced expiratory volume in 1 s
(FEV1) was assessed with an electronic spirometer (Masterscreen PFT,
Carefusion, SanDiego, CA) after inhalation of 400 µg salbutamol18 and
expressed as absolute value and as SDS.19 Total lung capacity (TLC)
was determined by whole body plethysmography (Masterscreen Body
Plethysmography, Carefusion, San Diego, CA) and expressed as
absolute value and percentile score. Diffusion capacity corrected for
alveolar volume (KCO) was measured using a multigas analyzer
(Masterscreen PFT, Carefusion, San Diego, CA) by the single-breath
method. Percentile scores for static lung volumes and diffusion
capacity obtained by the reference equations of Koopman et al20 were
transformed into SDS using an inverse normal transformation.
2.2.2 | Exercise capacity
All children performed a maximal cardiopulmonary exercise test after
the lung function assessment, that is, 1-2 h after inhalation of
salbutamol if applicable. Therefore, we evaluated only lung function
after bronchodilation (BD). Themaximal cardiopulmonary exercise test
was performed on a motordriven treadmill (En Mill; Enraf Nonius,
Rotterdam, the Netherlands), programmed for increases in angle of
inclination and speed according to the Bruce protocol.21,22 The
children were encouraged to perform to exhaustion. The maximal
endurance time (in minutes, one decimal) served as criterion of
exercise capacity, with SDS based on reference values for healthy
Dutch children.21,22 Heart rate and transcutaneous oxygen saturation
were monitored before and during the test with a pulse oximeter
(MARS (Motion Artifact Reduction System), type 2001; Respironics
Novametrix, Murrysville, PA). Heart rate of ≥185 beats per min23 or
loss of coordination because of excessive fatiguewas taken asmaximal
performance.
2.3 | Statistical analysis
Differences in baseline data between “participants in the follow-up
program” and “non-participants in the follow-up program” and the
children “treated with neonatal ECMO” and “not treated with
neonatal ECMO” were evaluated using Mann-Whitney U tests for
continuous variables and chi-square tests for categorical variables.
One-sample t-tests were used to test whether the normally
distributed data of exercise capacity differed from population norms
(SDS = 0). To test whether exercise capacity differed between ECMO
treated CDH patients and non-ECMO treated CDH patients,
independent samples t-tests were used. Longitudinal evaluation of
the endurance times at 5, 8, and 12 years of age was performed
using linear mixed-models, which can account for within-subject
correlations and allows for missing values in the dependent
variable.24 To investigate whether perinatal and demographic
characteristics had a significant influence on SDS endurance time,
we considered the following list of baseline data in the linear mixed-
model as covariates: gestational age, ECMO treatment, use of a
standardized treatment protocol (after November 2007), patch
repair, duration of initial hospital stay, ventilator-free days in the first
28 days of life, type of initial mechanical ventilation, congenital
cardiac malformation, and sports participation. We used a stepwise
backward approach to select covariates from this list of baseline
data. Two-way interaction effects were then added to the resulting
model if the interaction effect was statistically significant. The
TOUSSAINT-DUYSTER ET AL. | 3

results of the linear mixed-models are reported using estimated
marginal means, which are the predicted values of the dependent
variable adjusted for the effect of covariates. To investigate whether
lung function parameters (FEV1, TLC, KCO) had a significant influence
on SDS endurance time, only data of exercise capacity at the ages of
8 and 12 years was used, as lung function was not measured at the
age of 5. Therefore, separate linear mixed-models were performed
with the above-mentioned list of baseline data and FEV1, TLC and
KCO as covariates at 8 and 12 years of age. Multicollinearity was
assessed using variance inflation factors (VIFs). VIFs ≤5.0 were
considered acceptable, whereas higher values were taken as a sign of
multicollinearity. Spearman's rank correlation was used to test
whether the levels of exercise capacity as estimated by the parents
was associated with the measured SDS endurance time.
Analyses were performed using SPSS 21.0 (IBM, Chicago, IL), and
all statistical tests used a two-sided significance level of 0.05.
3 | RESULTS
3.1 | Patients
Between January 1999 and July 2012, 234 children were born with
CDH in the Erasmus MC—Sophia Children's Hospital. Sixty-five
(27.7%) died before hospital discharge (Figure 1). Fifty-five (32.4%)
of the 169 survivors were excluded for various reasons (Figure 1).
Thus, 114 (67.1%) performed the Bruce-protocol (220measurements).
We excluded the results of 29 measurements (13.8%) because
maximal performance was not achieved (Figure 1). The analysis for
this study concerned 191 reliable tests performed by 107 children
(62.9 % of all survivors), of whom 30 (28.0%) had received ECMO
treatment.
Patient characteristics are presented in Table 1. Duration of
mechanical ventilation, ventilator- free days within the first 28 days of
life, PICU stay and duration of initial hospital stay differed significantly
between children treated with and without ECMO. Also the presence
of CLD, treatment with phosphodiesterase type 5 inhibitor, and FEV1
after BD (at 8 years of age) were significantly different between these
groups (Table 1). No differences in background characteristics, except
for ethnicity (P = 0.001) and birthweight (P = 0.030), were found
between the participants and non-participants of our follow-up
program (data not shown).
3.2 | Exercise capacity
The estimated marginal mean (95% confidence interval (CI)) SDS
endurance time was significantly below the norm at all ages: 5 years:
−0.44 (−0.65 to −0.24); 8 years: −1.01 (−1.23 to−0.78); 12 years: −1.10
(−1.40 to −0.80) (all P < 0.001) (Table 3). The mean (SD) heart rate at
maximal exercise was 191 (9.0) beats per minute and the median (IQR)
transcutaneous oxygen saturation at maximal exercise was 98% (96-
99). Exercise capacity decreased significantly from the ages of 5 to 8
years (P < 0.001) and from 5 to 12 years (P < 0.001) (Table 2 of the
online supplement).
3.3 | ECMO treated CDH patients versus non-ECMOtreated CDH patients
Exercise capacity differed significantly between ECMO treated and
non-ECMO treated patients (mean difference (95%CI) 0.421 (0.117 to
0.724, P = 0.007), particularly at the age of 8 (P = 0.036). Exercise
capacity declined significantly in ECMO treated patients from 5 to
8 years (P = 0.001) and from 5 to 12 years (P = 0.006). This decline was
also seen in non-ECMO treated patients; from 5 to 8 years (P = 0.008)
and 5 to 12 years (P = 0.015) (Table 3, Figure 2, Table 2 of the online
supplement).
3.4 | Associations between exercise capacity andbaseline data
Exercise capacity was significantly negatively associated with the
duration of initial hospital stay (estimated coefficient (95%CI) −0.006
(−0.009 to 0.003), P < 0.001) and positively with KCO (estimated
coefficient (95%CI) 0.27 (0.01 to 0.53), P = 0.039). No other significant
associations were found between exercise capacity and timepoint of
assessment, gestational age, use of a new treatment protocol, patch
repair, ventilator free days in the first 28 days of life, type of initial
mechanical ventilation, congenital cardiac malformation, FEV1, TLC,
and sports participation (Table 3 of the online supplement). Although
exercise capacity differed significantly between ECMO treated and
non-ECMO treated patients—with lower exercise capacity in ECMO
treated patients—ECMO had no significant effect on the deterioration
of exercise capacity: no significant interaction-effect was found
between ECMO and time point of assessment for exercise capacity
(P = 0.363). For both groups the same trend in deterioration was
observed (Figure 2).
All VIFs were ≤3.1.
3.5 | Exercise capacity estimated by the parents
The levels of exercise capacity as estimated by the parents correlated
positively with the measured SDS endurance time (r = 0.420,
P < 0.001).
4 | DISCUSSION
Weevaluated longitudinally maximal exercise capacity in children with
CDH aged 5 to 12 years. Exercise capacity was significantly below the
norm at all ages, and declined significantly over time—not only in
children treated with ECMO but also in those who did not need ECMO
treatment. The duration of initial hospital stay and the diffusion
capacity of the lungs were associated with exercise capacity.
Treatment of neonates with CDH is challenging and therapeutic
strategies have changed over the decades. This has resulted in
decreasing mortality rates,2,25 and development of lung protecting
strategies, for example, gentle ventilation with permissive hypercap-
nia.26 Therefore, it is hard to compare the data of our population with
those who survived over 20 years ago.8,12–14,27,28 We previously
4 | TOUSSAINT-DUYSTER ET AL.

found decreased exercise capacity in 5-year-old CDH patients,
irrespective of whether they had been treated with ECMO.10 In
another study, in children with different underlying diagnoses, who
had all been treated with neonatal ECMO, we showed that maximal
exercise capacity was below the norm at 5, 8, and 12 years and
deteriorated over time.11Many children in that study cohortwere born
in the early 1990s.11 Despite the differences in study population, a
similar course in deteriorating of exercise capacity was observed in the
current study. These findings suggest that exercise capacity should be
assessed in childhood and adolescence, and even into adulthood. The
FIGURE 1 Flowchart of the study population selection. aChromosome aberration (n = 2), Cohen syndrome (n = 1), Loeys-Dietz syndrome(n = 1), Simpson-Golabi-Behmel syndrome (n = 3), Wolf-Hirschhorn syndrome (n = 1), autism (n = 3). bHemiplegia (n = 3), aortastenosis (n = 1),tracheacanule (n = 1), severe chronic lung disease (n = 1), organizational reasons (n = 2), anxiety (n = 1). cLoss of coordination (n = 7), anxiety(n = 7), refused (n = 2), no maximal performance (n = 10), loose shoelaces (n = 1), insufficient Dutch language (n = 1), calf muscle pain (n = 1).CDH = congenital diaphragmatic hernia; ECMO= extracorporeal membrane oxygenation
TOUSSAINT-DUYSTER ET AL. | 5

question remains, however, whether timely intervention indicated by
the assessment outcome may improve or at least prevent deteriora-
tion. Encouraging the children to engage in physical activity could help
prevent secondary morbidities. Pro-active counselling by physicians
and early referral to physical therapists may be useful.
The introduction of the postnatal treatment protocol of the CDH
EURO Consortium led to an increased survival of children born with
CDH.3 This protocol was implemented in our department in
November 2007. Standardization of postnatal management has
resulted in lower mortality but not a lower prevalence of CLD.2 This
suggests that more patients with CDH who develop CLD survive,
which may affect maximal exercise capacity. However, we could not
demonstrate a significant effect of the introduction of the protocol on
maximal endurance time (Tables 3 and 4 of the online supplement). The
effect of improved intensive caremight have been be counterbalanced
by a higher prevalence of survivors with CLD. Larger numbers of
children should be studied at 8 and 12 years to demonstrate a possible
effect of the implementation of the treatment protocol on exercise
capacity.
We assumed that children with more severe lung hypoplasia,
might be at the highest risk for impaired exercise capacity. Indeed,
children who had been treated with ECMO had significantly more
airflow obstruction and lower SDS endurance time. Interestingly, KCO
was significantly below the norm both in ECMO treated and non-
ECMO treated children and was positively associated with exercise
capacity, whereas ECMO treatment was not associated with exercise
capacity. We speculate that microstructural changes of the lungs,
which have been described in young adults with CDH,6 may already
occur at younger age. Future studies focusing on lung structure
imaging may be useful to identify patients at risk for clinical
deterioration and impaired exercise tolerance. The association
between initial hospital stay duration and exercise capacity that we
TABLE 2 Characteristics at follow-up assessments
At follow-up Total n = 107 ECMO n = 30 non-ECMO n = 77 P
At 5 years of age n = 87 n = 23 n = 64
Sports participation (%) 46 (52.9) 14 (60.9) 32 (50.0) 0.373
Referral to PPTa (%) 13 (14.9) 4 (17.4) 9 (14.1) 0.703
PPT continuationb (%) 8 (9.2) 4 (17.4) 4 (6.3) 0.115
At 8 years of age n = 69 n = 26 n = 43
SDS FEV1 −0.28 (−1.25 to 0.62) −1.02 (−1.82 to 0.56) −0.10 (−0.73 to 0.67) 0.024
SDS TLC −0.05 (−0.90 to 0.58) −0.07 (−1.04 to 0.39) −0.05 (−0.80 to 0.71) 0.576
SDS KCO −1.48 (−2.05 to −0.51) −1.64 (−2.33 to −0.99) −1.18 (−1.97 to −0.44) 0.172
Sports participation (%) 54 (78.3) 18 (69.2) 36 (83.7) 0.160
Referral to PPTa (%) 20 (28.9) 10 (38.4) 10 (23.7) 0.180
PPT continuationb (%) 2 (2.9) 1 (3.8) 2 (4.7) 0.717
At 12 years of age n = 35 n = 18 n = 17
SDS FEV1 −0.54 (−1.55 to 0.25) −1.10 (−2.52 to 0.24) −0.35 (−0.88 to 0.25) 0.136
SDS TLC 0.28 (−0.81 to 1.08) −0.15 (−1.07 to 0.66) 0.39 (−0.67 to 1.49) 0.159
SDS KCO −1.28 (−1.88 to −0.88) −1.48 (−2.33 to −0.20) −1.20 (−1.62 to −0.90) 0.446
Sports participation (%) 24 (68.6) 11 (61.1) 13 (76.5) 0.335
Referral to PPTa (%) 10 (28.6) 6 (33.3) 4 (23.5) 0.527
PPT continuationb (%) – – – –
aAfter follow-up assessment the patient was referred to a local community based pediatric physical therapist to start intervention.bAfter follow-up assessment the patient was recommended to continue intervention by a local community based pediatric physical therapist.
Data are presented as median (interquartile range) or number (percentage), as appropriate. ECMO, extracorporeal membrane oxygenation.
TABLE 3 Endurance time of CDH patients treated with and without ECMO
5 years 8 years 12 years
All CDH patients, n = 107 −0.44 (−0.65 to −0.24)a −1.01 (−1.23 to −0.78)a −1.10 (−1.40 to −0.80)a
ECMO, n = 31 −0.63 (−1.04 to −0.21)b −1.34 (−1.74 to −0.94)a −1.32 (−1.77 to −0.86)a
non-ECMO, n = 71 −0.38 (−0.61 to −0.15)a −0.82 (−1.10 to −0.55)a −0.96 (−1.38 to −0.53)a
Data are presented as estimated marginal means (95% confidence intervals) SDS endurance time. Significantly below the population norm (SDS = 0):aP ≤ 0.001; bP = 0.004.
6 | TOUSSAINT-DUYSTER ET AL.

found suggests that the most critically ill neonates with the most
severe pulmonary problems are most likely to suffer from persistent
pulmonary morbidity later in life.
Besides, we speculate that parents of children who had been
critically ill as neonates may consider their child more vulnerable than
the parents of the child's healthy peers. For this reason, and also
because pulmonary morbidity persist for years,4,5 parents may not
encourage physical activities. This may, in turn, puts them at risk of
gross motor function problems29,30 and consequently reduced
participation in physical activities. Smith et al found similar problems
in children born very preterm. Reduced exercise capacity could not be
explained by airflow obstruction. Therefore, these authors also
hypothesized that children born very preterm are deconditioned and
that a lack of physical activitymight play a role.31 Although in our study
ECMO treatment had no significant influence on decreased exercise
capacity and its deterioration, we assume that the lower exercise
capacity in ECMO treated CDHpatients might be explained by the fact
that ECMO treated patients are the most critically ill children at
neonatal age with more severe lung hypoplasia, more airflow
obstruction, and less participation in physical activities.
Following this reasoning, the deterioration in exercise capacity
between the ages 5 and 8, and its stabilization from the ages of 8,
could perhaps partly be explained by sports participation. At the age
of 8 and 12 about two thirds of the children participated in sports
versus only half of them at the age of 5. Assumable, parents consider
their child in the first years of life more vulnerable and are reluctant
to encourage their children in daily physical activities and sports
participation.
The main strengths of this study are the longitudinal design
within the infrastructure of a standardized follow-up program, the
small proportion of children lost to follow-up and the relatively large
sample size for this rare congenital anomaly. Some limitations need
to be addressed. Not all children participating in the follow-up
program had reached the age of 12 years yet. The resulting small
number of children assessed at 12 years of age increases the
probability of a type II error, although mixed models account for data
missing at random. Secondly, postnatal management of CDH
changed during the study period, which could have influenced our
results as more children with severe lung hypoplasia survived after
introduction of the standardized postnatal treatment protocol. We
did not find a significant effect of the introduction of the postnatal
treatment protocol on exercise capacity (Tables 3 and 4 of the online
supplement), but larger sample sizes of 8-year-old and 12-year-old
children may be needed to detect a significant difference. Thirdly, we
used the maximal endurance time rather than the peak oxygen
consumption as measure of exercise capacity, mainly for reasons of
feasibility. Wearing a mask may lead to loss of cooperation and to
submaximal results, especially in the younger children. A strong
correlation between maximal endurance time and maximal oxygen
uptake has been reported by Cumming and coworkers.32 Besides,
since our setting is an outpatient clinic and not a primary research
setting, we feel that cardiopulmonary exercise testing (CPX), which
includes breath gas analysis, is too intensive to perform in every
CDH patient during routine follow-up. In future research projects in
our department, CPX in children will be evaluated, and conclusions
on exercise capacity in CDH patients might be extended. Fourthly,
we did not include a group of healthy controls. However, we used
recently established reference data collected in our own center.21,22
Fifthly, we had no data on physical activity. Reduced physical activity
might be one of the explanations for decreased exercise capacity in
children with CDH and is subject of an ongoing research project in
our center. Finally, considering the large amount of possible
determinants of exercise capacity, as well as the possibility of
multicollinearity we had to be critical which lung function
parameters to include as possible determinants in the mixed model
analysis. In a cross-sectional study of Peetsold et al,5 exercise
capacity and lung function was measured in school-aged children
born with CDH and having been referred either to the Paediatric
Surgical Centre of Amsterdam (the Netherlands) between 1987 and
1999, and to our center between 1988 and 1994. They showed no
associations between VO2max and lung function parameters, except
for FEV1 (R2 = 0.27; P = 0.001). In another study of our research
group none of the lung function parameters, but DLCO was related to
VO2peak % pred. in young adult CDH patients.14 Therefore, as
multicollinearity arose between lung function parameters in this
study, we critically chose to include only FEV1, TLC and KCO in the
mixed model analysis.
The significant differences in ethnicity and birthweight between
the participants and non-participants in this study was in line with
expectations. We found a higher percentage of other ethnicities than
Dutch and lower birthweight in the non-participant group. Native
Dutch parents and children showed higher follow-up and treatment
adherence than parents of other ethnicities.33 Differences in birth-
weight between ethnicities are common.34 Nevertheless, we will
pursue our strategies to enhance adherence in non-native Dutch
parents and children in our follow-up program. Background character-
istics that reflect severity of illness did not differ between the
FIGURE 2 Change in maximal exercise capacity over time inchildren with CDH. Data shown are estimated marginal means fromthe linear mixed-model analysis with 95% confidence intervals.CDH = congenital diaphragmatic hernia; ECMO= extracorporealmembrane oxygenation; SDS = standard deviation score
TOUSSAINT-DUYSTER ET AL. | 7

participants and non-participants (data not shown). Selection bias is
likely not present.
5 | CONCLUSION
CDH patients were at risk for decreased exercise capacity at school-
age. Decreased exercise capacity deteriorated over time, not only in
children who had needed neonatal ECMO treatment but also in
children who had not needed ECMO. Exercise capacity was
significantly negatively associated with the duration of initial hospital
stay and positively with KCO. Early risk stratification for decreased
exercise capacity may be important to offer timely intervention.
Further studies are needed to unravel the causes of decreased exercise
capacity. We recommend prolonged follow-up, pro-active advice on
physical activities and sports participation or referral to a physical
therapist.
ACKNOWLEDGMENTS
We thank the staff of our long-term follow-up team, the technicians of
the lung function department of our hospital for their help in data
collection. Ko Hagoort provided editorial advice. No funding was
secured for this study.
ORCID
Hanneke IJsselstijn http://orcid.org/0000-0001-5824-3492
REFERENCES
1. Ackerman KG, Pober BR. Congenital diaphragmatic hernia andpulmonary hypoplasia: new insights from developmental biologyand genetics. Am J Med Genet C Semin Med Genet.
2007;145C:105–108.2. Van Den Hout L, Schaible T, Cohen-Overbeek TE, et al. Actual
outcome in infants with congenital diaphragmatic hernia: the role of astandardized postnatal treatment protocol. Fetal Diagn Ther.2011;29:55–63.
3. Reiss I, Schaible T, van den Hout L, et al. Standardized postnatalmanagement of infants with congenital diaphragmatic hernia inEurope: the CDH EURO Consortium consensus. Neonatology.2010;98:354–364.
4. Spoel M, Laas R, Gischler SJ, et al. Diagnosis-related deterioration of
lung function after extracorporeal membrane oxygenation. Eur RespirJ. 2012;40:1531–1537.
5. Peetsold MG, Heij HA, Nagelkerke AF, et al. Pulmonary function andexercise capacity in survivors of congenital diaphragmatic hernia. Eur
Respir J. 2009;34:1140–1147.6. Spoel M, Marshall H, IJsselstijn H, et al. Pulmonary ventilation and
micro-structural findings in congenital diaphragmatic hernia. PediatrPulmonol. 2016;51:517–524.
7. Trachsel D, Selvadurai H, Adatia I, et al. Resting and exercise
cardiorespiratory function in survivors of congenital diaphragmatichernia. Pediatr Pulmonol. 2006;41:522–529.
8. Zaccara A, Turchetta A, Calzolari A, et al. Maximal oxygen consump-tion and stress performance in children operated on for congenital
diaphragmatic hernia. J Pediatr Surg. 1996;31:1092-1094; discussion1095.
9. Turchetta A, Fintini D, Cafiero G, et al. Physical activity, fitness, and
dyspnea perception in children with congenital diaphragmatic hernia.Pediatr Pulmonol. 2011;46:1000–1006.
10. Gischler SJ, van der Cammen-van Zijp MHM, Mazer P, et al.A prospective comparative evaluation of persistent respiratory
morbidity in esophageal atresia and congenital diaphragmatic herniasurvivors. J Pediatr Surg. 2009;44:1683–1690.
11. van der Cammen-van Zijp MH, Gischler SJ, Hop WC, de Jongste JC,Tibboel D, IJsselstijn H. Deterioration of exercise capacity afterneonatal extracorporeal membrane oxygenation. Eur Respir J.
2011;38:1098–1104.12. Marven SS, Smith CM, Claxton D, et al. Pulmonary function, exercise
performance, and growth in survivors of congenital diaphragmatichernia. Arch Dis Child. 1998;78:137–142.
13. PeetsoldMG, Vonk-Noordegraaf A, Heij HH, Gemke RJBJ. Pulmonary
function and exercise testing in adult survivors of congenitaldiaphragmatic hernia. Pediatr Pulmonol. 2007;42:325–331.
14. van der Cammen-van ZijpMH, SpoelM, Laas R, et al. Exercise capacity,daily activity, and severity of fatigue in term born young adults afterneonatal respiratory failure. Scand JMed Sci Sports. 2014;24:144–151.
15. Mazer P, Gischler SJ, Cammen-VAN Zijp VANDERMH, et al. Earlydevelopmental assessment of children with major non-cardiaccongenital anomalies predicts development at the age of 5 years.Dev Med Child Neurol. 2010;52:1154–1159.
16. Stolar CJ, Snedecor SM, Bartlett RH. Extracorporeal membrane oxygen-
ation andneonatal respiratory failure: experience from theextracorporeallife support organization. J Pediatr Surg. 1991;26:563–571.
17. Jobe AH, Bancalari EH. Controversies about the definition of broncho-pulmonary dysplasia at 50 years. Acta Paediatr. 2017;106:692–693.
18. Miller MR, Hankinson J, Brusasco V, et al. Standardisation ofspirometry. Eur Respir J. 2005;26:319–338.
19. Quanjer PH, Stanojevic S, Cole TJ, et al. Multi-ethnic reference valuesfor spirometry for the 3-95-yr age range: the global lung function 2012equations. Eur Respir J. 2012;40:1324–1343.
20. Koopman M, Zanen P, Kruitwagen CL, van der Ent CK, Arets HG.Reference values for paediatric pulmonary function testing: theUtrecht dataset. Respir Med. 2011;105:15–23.
21. van der Cammen-van ZijpMH, van den Berg-Emons RJ,Willemsen SP,Stam HJ, Tibboel D, IJsselstijn H. Exercise capacity in Dutch children:
new reference values for the Bruce treadmill protocol. Scand J Med SciSports. 2010;20:e130–e136.
22. van der Cammen-van ZijpMHM, IJsselstijn H, Takken T, et al. Exercisetesting of pre-school children using the Bruce treadmill protocol: new
reference values. Eur J Appl Physiol. 2010;108:393–399.23. Karila C, de Blic J, Waernessyckle S, Benoist MR, Scheinmann P.
Cardiopulmonary exercise testing in children − An individualizedprotocol for workload increase. Chest. 2001;120:81–87.
24. Fitzmaurice GM, Ware JH. Applied Longitudinal Analysis. Hoboken:
John Wiley & Sons; 2004.
25. Barroso C, Correia-Pinto J. Thoracoscopic repair of congenital
diaphragmatic hernia, review of the results. Minerva Pediatr.2017;70:281–288.
26. Wung JT, Sahni R,Moffitt ST, Lipsitz E, Stolar CJ. Congenital diaphragmatichernia: survival treatedwith very delayed surgery, spontaneous respiration,and no chest tube. J Pediatr Surg. 1995;30:406–409.
27. IJsselstijn H, Tibboel D, Hop WJ, Molenaar JC, de Jongste JC. Long-
term pulmonary sequelae in children with congenital diaphragmatichernia. Am J Respir Crit Care Med. 1997;155:174–180.
28. Montgomery MFB, Freyschuss U, Mortensson W. Long-term-follow-up of respiratory function, maximal working capacity, and esophagealfunction. Pediatr Surg Int. 1995;10:519–522.
29. van der Cammen-van Zijp MHM, Janssen AJ, Raets MM, et al.Motor performance after neonatal extracorporeal membrane
8 | TOUSSAINT-DUYSTER ET AL.

oxygenation: a longitudinal evaluation. Pediatrics. 2014;134:427–435.
30. MadderomMJ, Toussaint LCC, van der Cammen-van Zijp MHM, et al.
Congenital diaphragmatic hernia with(out) ECMO: impaired develop-ment at 8 years. Arch Dis Child Fetal Neonatal Ed. 2013;98:316–322.
31. Smith LJ, van Asperen PP, McKay KO, Selvadurai H, Fitzgerald DA.Reduced exercise capacity in children born very preterm. Pediatrics.
2008;122:287–293.32. Cumming GR, Everatt D, Hastman L. Bruce treadmill test in children:
normal values in a clinic population. Am J Cardiol. 1978;41:69–75.33. DahhanN,MeijssenD, ChegaryM, BosmanD,Wolf B. Ethnic diversity
outpatient clinic in paediatrics. BMC Health Serv Res. 2012;12:12.
34. Troe EJ, Raat H, Jaddoe VW, et al. Explaining differences inbirthweight between ethnic populations. The Generation R Study.BJOG. 2007;114:1557–1565.
SUPPORTING INFORMATION
Additional supporting information may be found online in the
Supporting Information section at the end of the article.
How to cite this article: Toussaint-Duyster LCC, van der
Cammen-van Zijp MHM, de Jongste JC, et al. Congenital
diaphragmatic hernia and exercise capacity, a longitudinal
evaluation. Pediatric Pulmonology. 2019;1–9.
https://doi.org/10.1002/ppul.24264
TOUSSAINT-DUYSTER ET AL. | 9
Recommended