Embed Size (px)
Citation preview
¿Cómo mejorar el manejo de las infecciones de piel y partes blandas en el Hospital?
José Ramón Paño PardoMedicina Interna
UMCEI-HULP
Joaquín Llorente GarcíaR4 Medicina Interna
Complejo Asistencial Universitario de León
Sesión de Enfermedades InfecciosasHospital Universitario La Paz
25 de Febrero de 2015
Contexto/Relevancia
Guía de tratamiento de las infecciones de piel y tejidos blandos Rev Esp Quimioterap, Diciembre 2006; Vol. 19 (Nº 4): 378-394
CLASIFICACÍÓN / DIAGNÓSTICO
ABORDAJE MÉDICO-QUIRURGUICO
Contexto/Relevancia
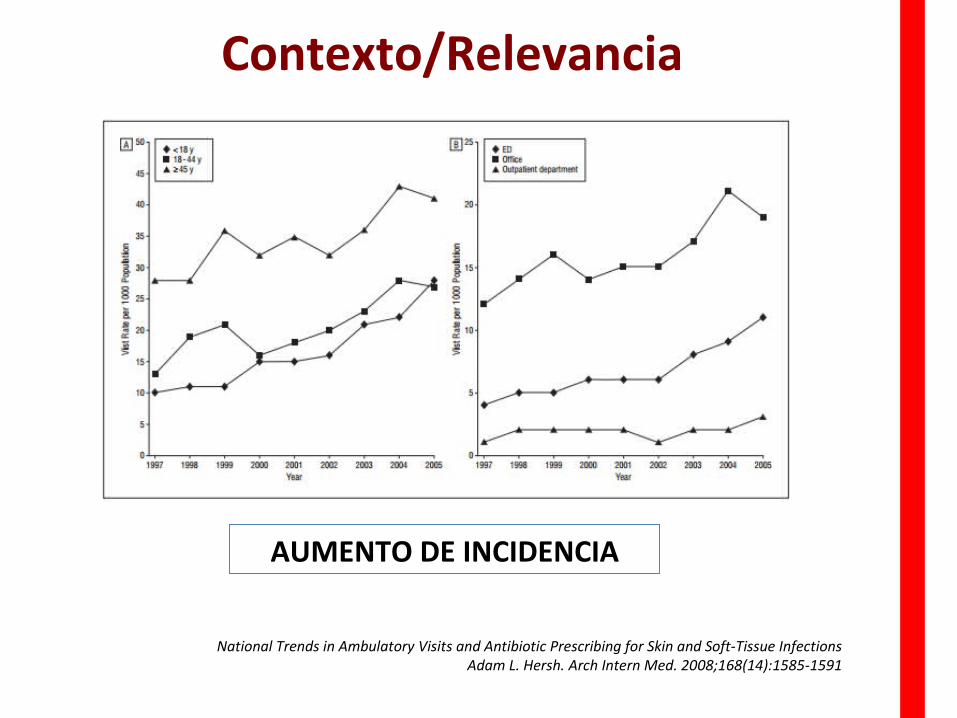
National Trends in Ambulatory Visits and Antibiotic Prescribing for Skin and Soft-Tissue Infections Adam L. Hersh. Arch Intern Med. 2008;168(14):1585-1591
AUMENTO DE INCIDENCIA
Contexto/Relevancia
Guión/Metodología
Metodología
Identificación de problemas en el manejo de IPPB* JLLG & JRP (a propósito de 2 casos clínicos)
Revisión de la literatura JLLG
¿Soluciones?
(JLLG & JRP) + ¡¡Audiencia!!
Ámbito: IPPB, excluyendo ILQ** y Pie diabético
* IPPB: Infección de piel y partes blandas** ILQ: infección de localización quirúrgica
Problemas en el manejo de IPPB
1. Identificación de la gravedad
2. Identificación/anticipación de la etiología
3. Monitorización de la evolución
Identificación de problemas
Problemas Diagnósticos
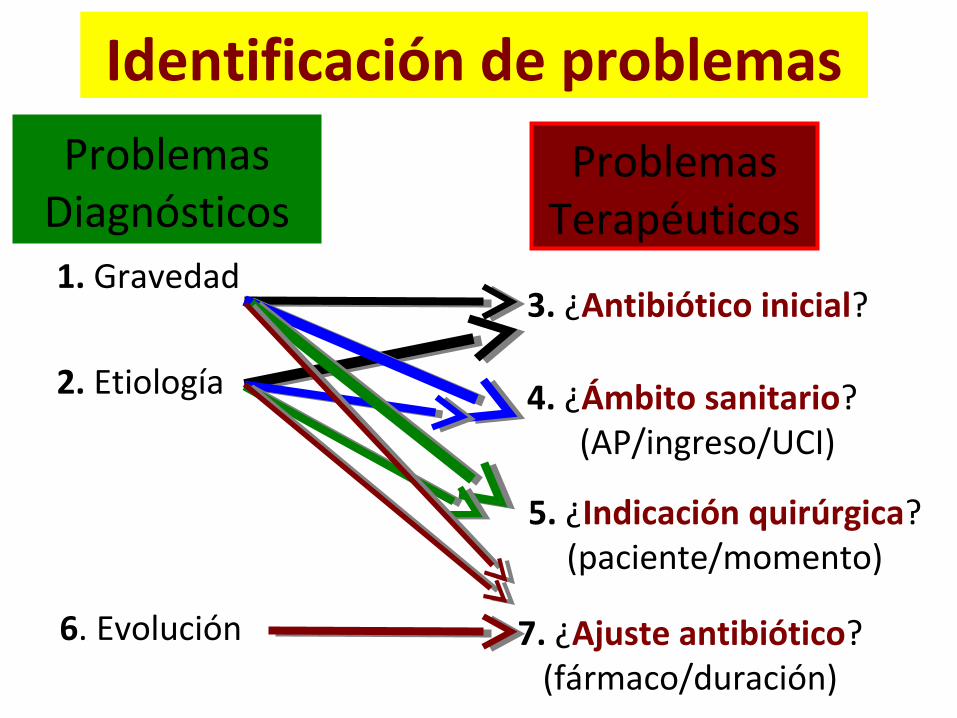
1. Gravedad
2. Etiología
6. Evolución
Identificación de problemas
Problemas Terapéuticos
3. ¿Antibiótico inicial?
4. ¿Ámbito sanitario?(AP/ingreso/UCI)
5. ¿Indicación quirúrgica?(paciente/momento)
7. ¿Ajuste antibiótico?(fármaco/duración)
Problemas Diagnósticos
Problemas en el manejo de IPPB
1. Identificación de la gravedad
1.1. Gravedad sistémica
1. Identificación de la gravedad
• No SIRS/ Sepsis*/ Sepsis Grave / Shock Séptico• Score de Pitt• APACHE, SOFA, etc
¡Común al resto de infecciones!

1.1. Gravedad local
1. Identificación de la gravedad
Extensión
Profundidad
¡Necrosis!Localización
1.1. Gravedad local
1. Identificación de la gravedad
¿Se puede identificar clínicamente la gravedad local?
¿Bien? ¿Mal? ¿Regular?
¿Clasificaciones clínicas para el manejo clínico de las infecciones
de piel y partes blandas?
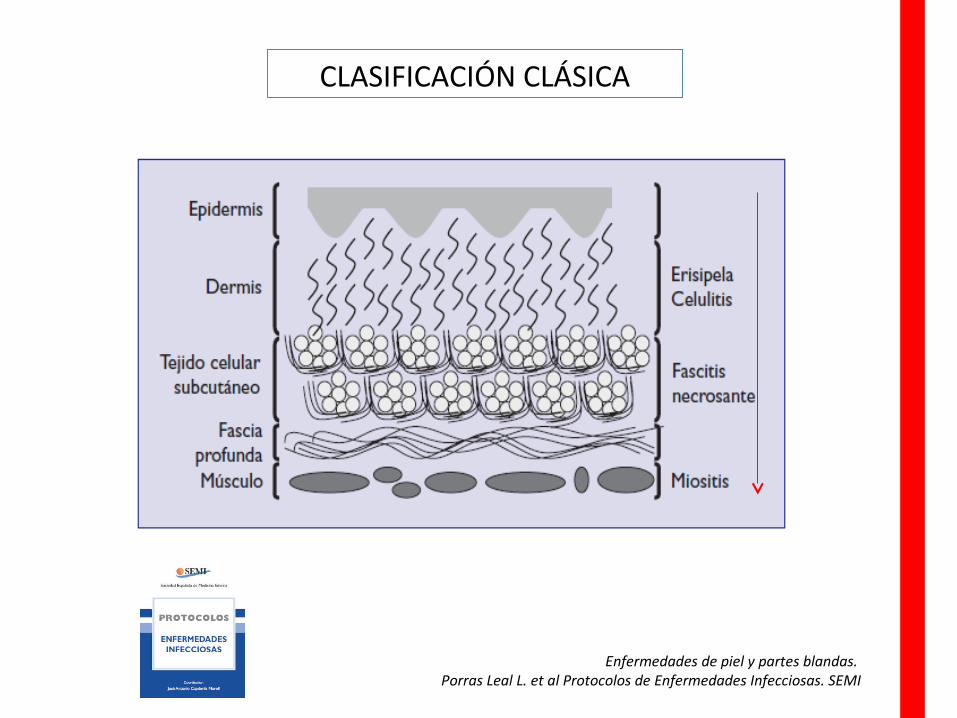
CLASIFICACIÓN CLÁSICA
Enfermedades de piel y partes blandas. Porras Leal L. et al Protocolos de Enfermedades Infecciosas. SEMI

ERISIPELA
• Tipo específico de celulitis superficial de la piel con una intensa afectación linfática (SGA)
• Dolorosa, rojo brillante, con piel edematosa e indurada («piel de naranja») y un borde elevado de avance bien delimitado Celulitis, Infecciones necrotizantes e infecciones del tejido subcutáneo.
Enfermedades Infecciosas. Principios y práctica., 7th ed, Mandell GL, Bennett JE, Dolin R (Eds), Elsevier, Philadelphia 2010.
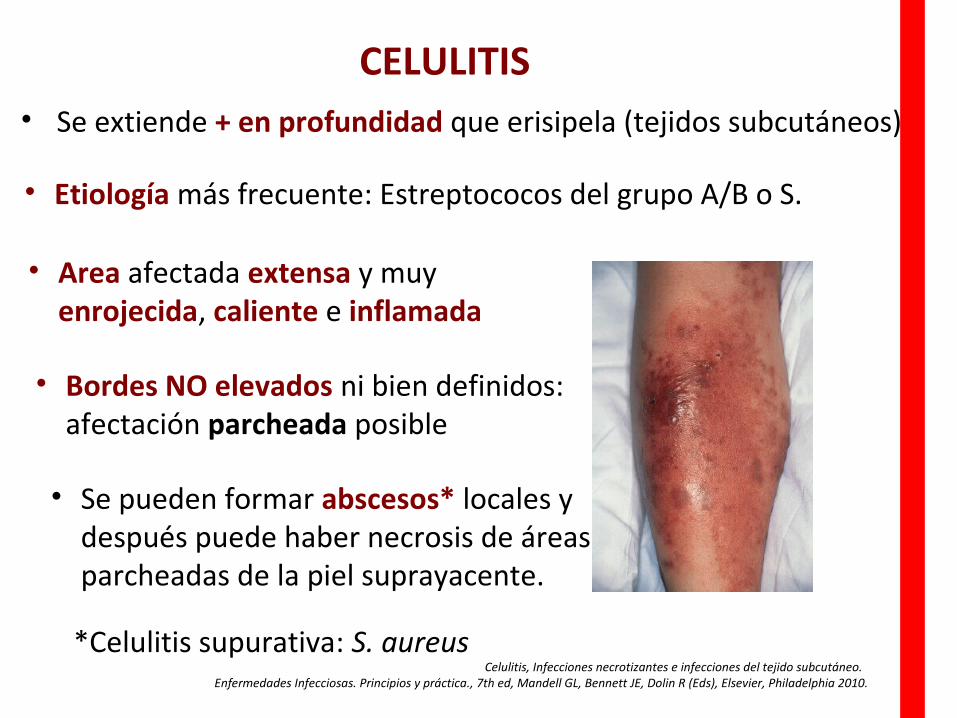
• Se extiende + en profundidad que erisipela (tejidos subcutáneos)
• Area afectada extensa y muy enrojecida, caliente e inflamada
Celulitis, Infecciones necrotizantes e infecciones del tejido subcutáneo. Enfermedades Infecciosas. Principios y práctica., 7th ed, Mandell GL, Bennett JE, Dolin R (Eds), Elsevier, Philadelphia 2010.
CELULITIS
• Etiología más frecuente: Estreptococos del grupo A/B o S.
• Bordes NO elevados ni bien definidos: afectación parcheada posible
• Se pueden formar abscesos* locales y después puede haber necrosis de áreas parcheadas de la piel suprayacente.
*Celulitis supurativa: S. aureus
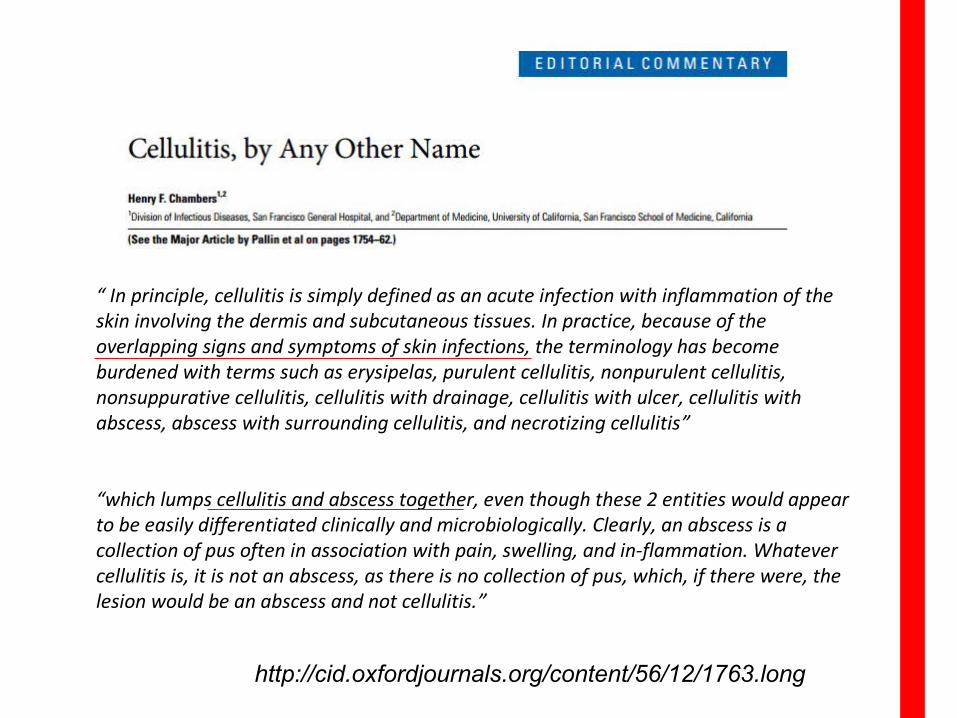
“ In principle, cellulitis is simply defined as an acute infection with inflammation of the skin involving the dermis and subcutaneous tissues. In practice, because of the overlapping signs and symptoms of skin infections, the terminology has become burdened with terms such as erysipelas, purulent cellulitis, nonpurulent cellulitis, nonsuppurative cellulitis, cellulitis with drainage, cellulitis with ulcer, cellulitis with abscess, abscess with surrounding cellulitis, and necrotizing cellulitis”
“which lumps cellulitis and abscess together, even though these 2 entities would appear to be easily differentiated clinically and microbiologically. Clearly, an abscess is a collection of pus often in association with pain, swelling, and in-flammation. Whatever cellulitis is, it is not an abscess, as there is no collection of pus, which, if there were, the lesion would be an abscess and not cellulitis.”
http://cid.oxfordjournals.org/content/56/12/1763.long
Celulitis, Infecciones necrotizantes e infecciones del tejido subcutáneo. Enfermedades Infecciosas. Principios y práctica., 7th ed, Mandell GL, Bennett JE, Dolin R (Eds), Elsevier, Philadelphia 2010.
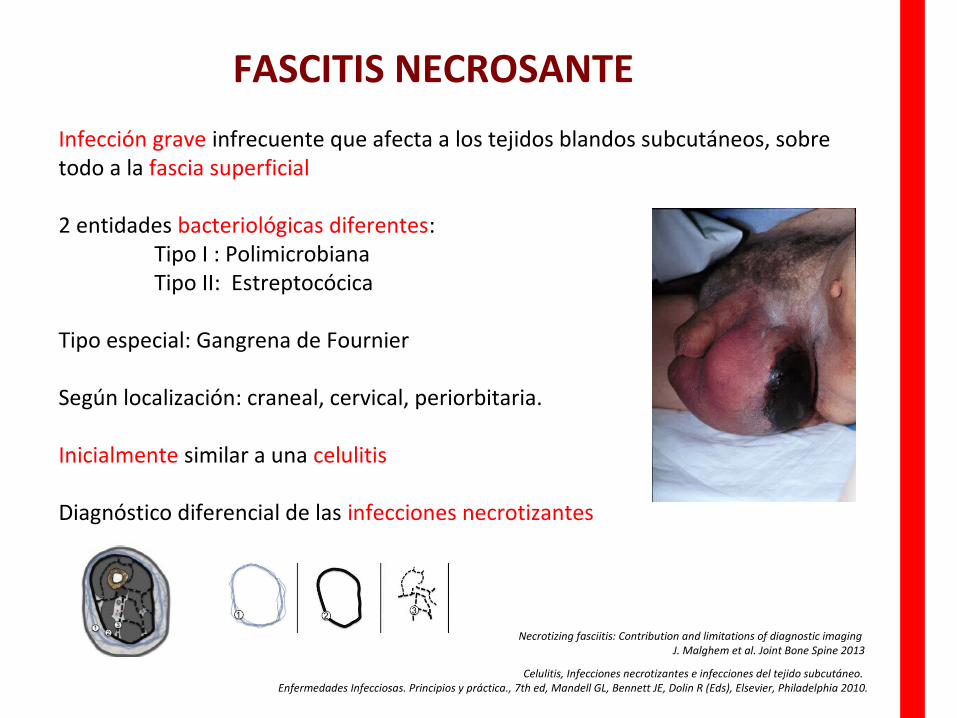
Infección grave infrecuente que afecta a los tejidos blandos subcutáneos, sobre todo a la fascia superficial
2 entidades bacteriológicas diferentes:Tipo I : PolimicrobianaTipo II: Estreptocócica
Tipo especial: Gangrena de Fournier
Según localización: craneal, cervical, periorbitaria.
Inicialmente similar a una celulitis
Diagnóstico diferencial de las infecciones necrotizantes
Necrotizing fasciitis: Contribution and limitations of diagnostic imaging J. Malghem et al. Joint Bone Spine 2013
FASCITIS NECROSANTE
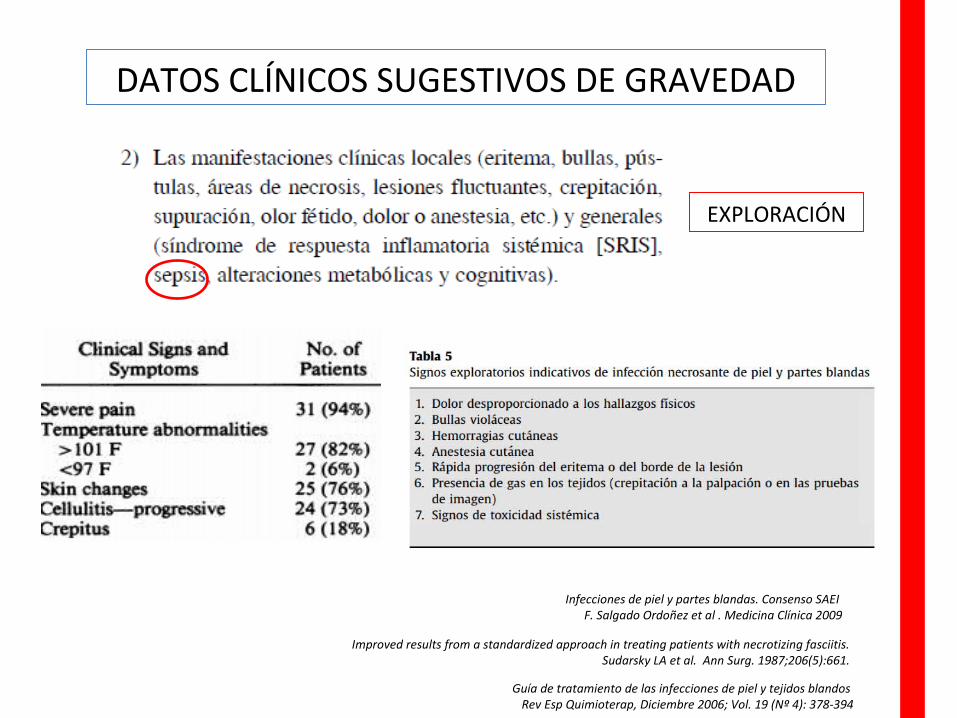
DATOS CLÍNICOS SUGESTIVOS DE GRAVEDAD
EXPLORACIÓN
Improved results from a standardized approach in treating patients with necrotizing fasciitis.Sudarsky LA et al. Ann Surg. 1987;206(5):661.
Guía de tratamiento de las infecciones de piel y tejidos blandos Rev Esp Quimioterap, Diciembre 2006; Vol. 19 (Nº 4): 378-394
Infecciones de piel y partes blandas. Consenso SAEI F. Salgado Ordoñez et al . Medicina Clínica 2009
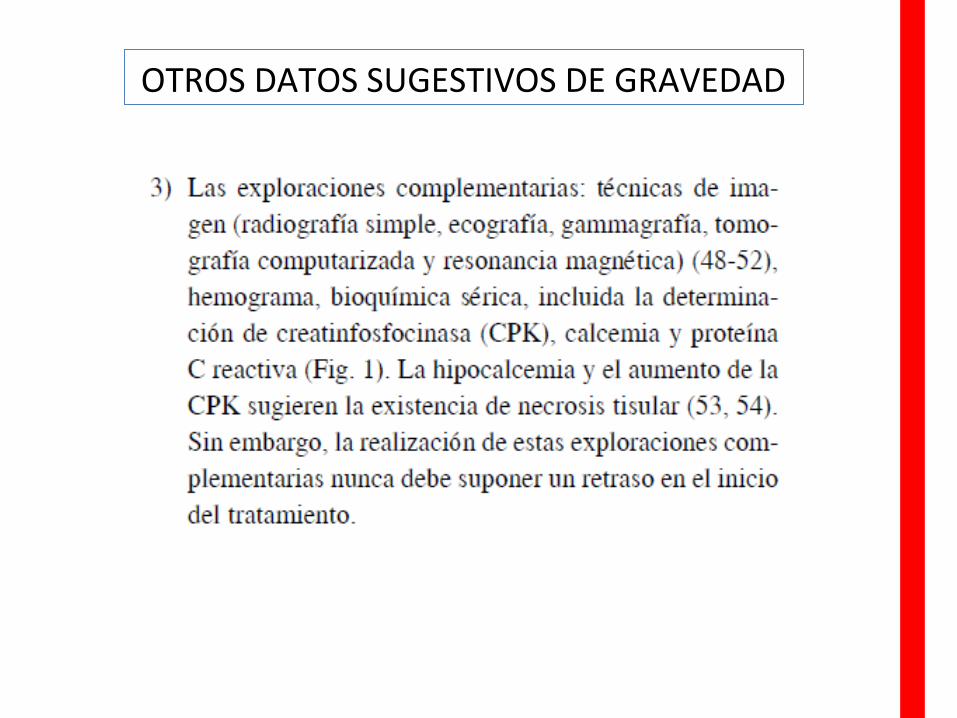
OTROS DATOS SUGESTIVOS DE GRAVEDAD
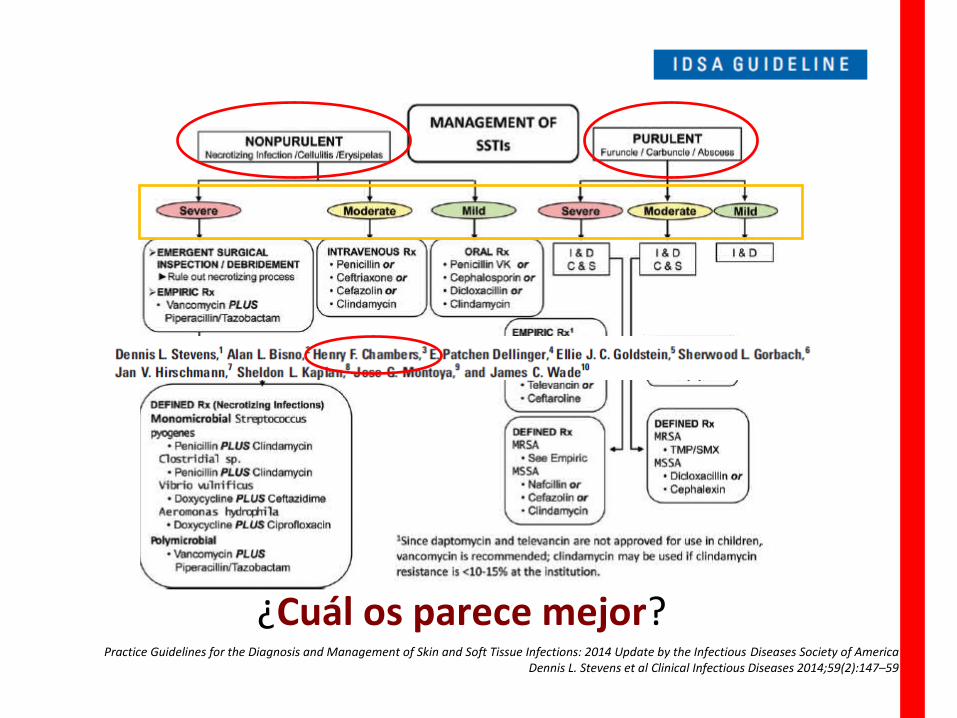
Practice Guidelines for the Diagnosis and Management of Skin and Soft Tissue Infections: 2014 Update by the Infectious Diseases Society of AmericaDennis L. Stevens et al Clinical Infectious Diseases 2014;59(2):147–59
¿Cuál os parece mejor?
Problemas en el manejo de IPPB
2. Identificación/anticipación de la etiología
1. Identificación dela gravedad
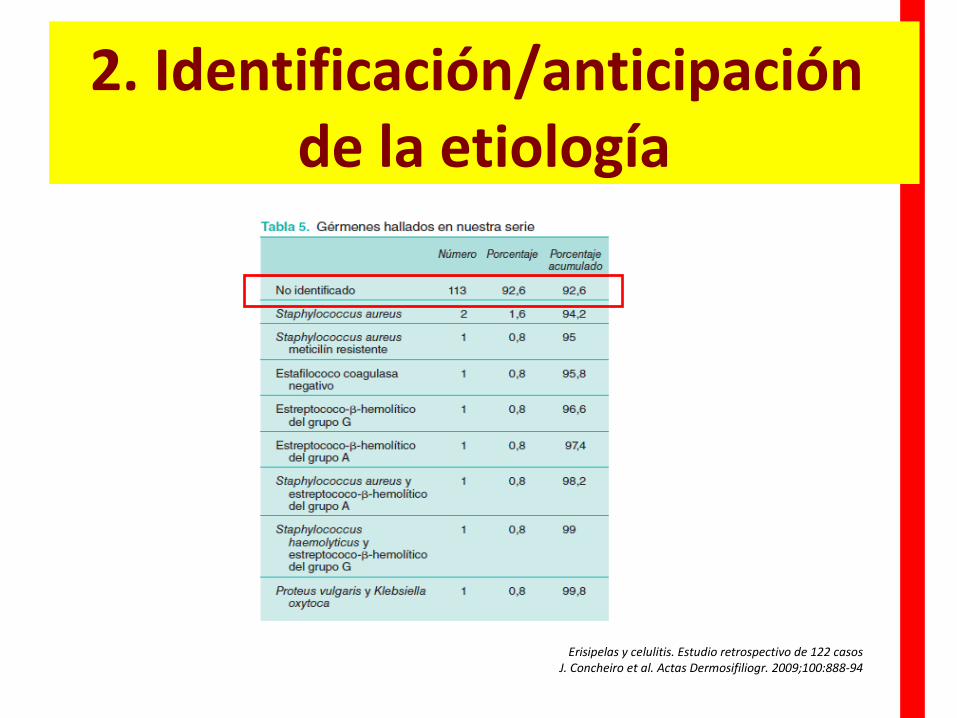
Erisipelas y celulitis. Estudio retrospectivo de 122 casosJ. Concheiro et al. Actas Dermosifiliogr. 2009;100:888-94
2. Identificación/anticipación de la etiología
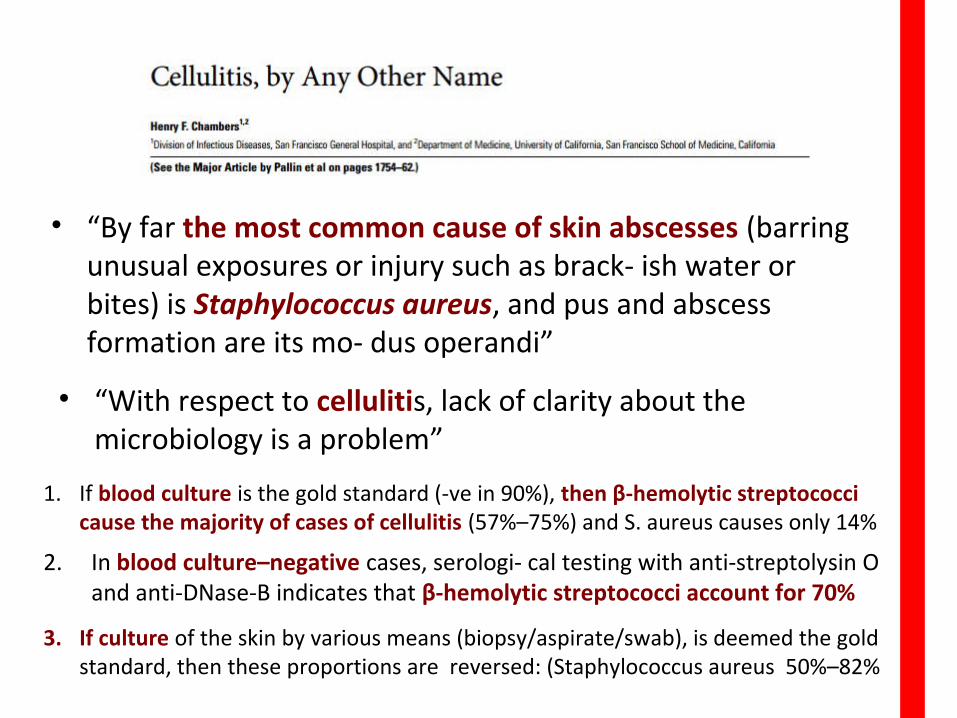
• “By far the most common cause of skin abscesses (barring unusual exposures or injury such as brack- ish water or bites) is Staphylococcus aureus, and pus and abscess formation are its mo- dus operandi”
• “With respect to cellulitis, lack of clarity about the microbiology is a problem”
1. If blood culture is the gold standard (-ve in 90%), then β-hemolytic streptococci cause the majority of cases of cellulitis (57%–75%) and S. aureus causes only 14%
2. In blood culture–negative cases, serologi- cal testing with anti-streptolysin O and anti-DNase-B indicates that β-hemolytic streptococci account for 70%
3. If culture of the skin by various means (biopsy/aspirate/swab), is deemed the gold standard, then these proportions are reversed: (Staphylococcus aureus 50%–82%
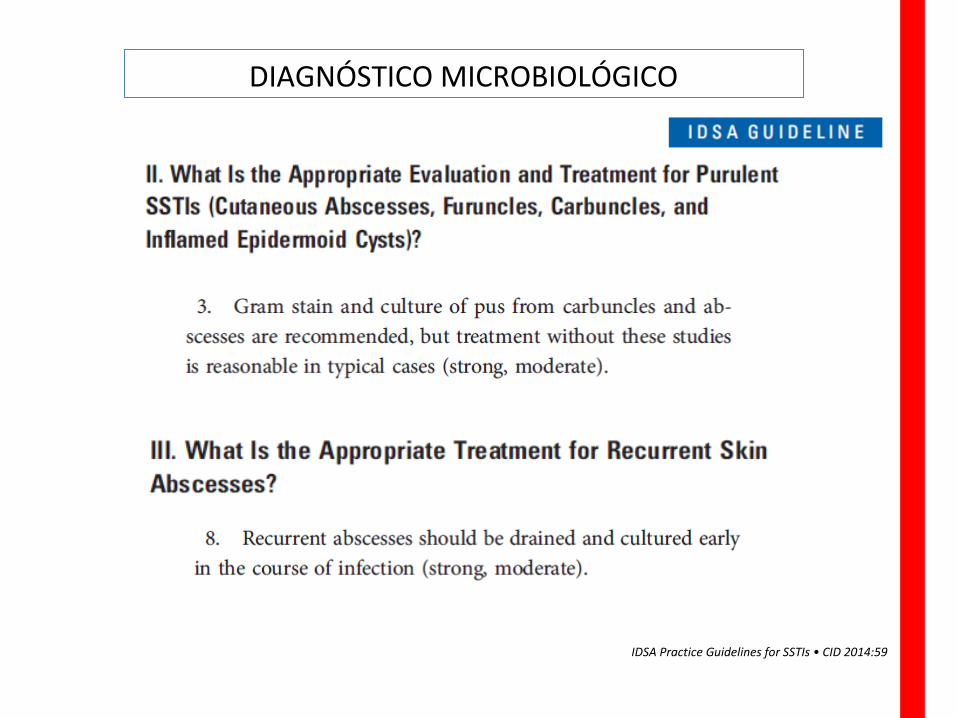
DIAGNÓSTICO MICROBIOLÓGICO
IDSA Practice Guidelines for SSTIs • CID 2014:59
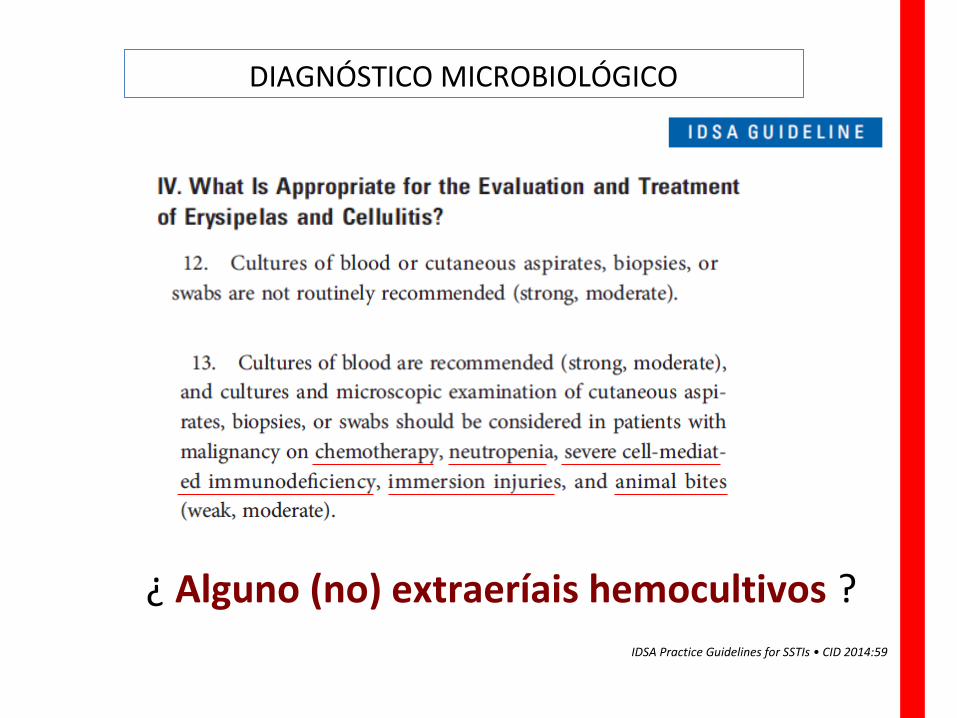
DIAGNÓSTICO MICROBIOLÓGICO
IDSA Practice Guidelines for SSTIs • CID 2014:59
¿ Alguno (no) extraeríais hemocultivos ?
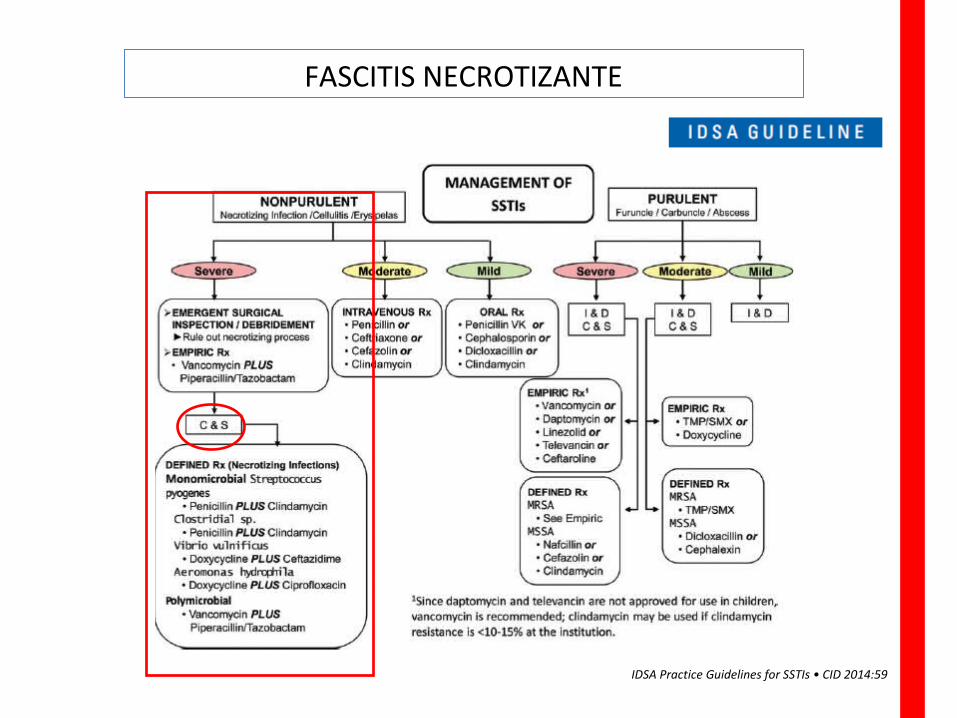
FASCITIS NECROTIZANTE
IDSA Practice Guidelines for SSTIs • CID 2014:59
ETIOLOGÍA DE FASCITIS NECROTIZANTE
Datos Aportados por el Servicio de Cirugía Plástica HULP
32 pacientes con diagnóstico de Fascitis Necrotizante
Se tomaron muestras intraoperatorias para Gram y Cultivo
27 positivos (84,3%) 5 estériles (15,7%)
Tipo I: 66% de los casos (G- y anaerobios)
Tipo II: 33% (G+)
Aislamiento más frecuente de microorganismos:E. coli (30,7%)Bacteroides (15,3%)S. pyogenes (15,3%)S. aureus (15,3%)
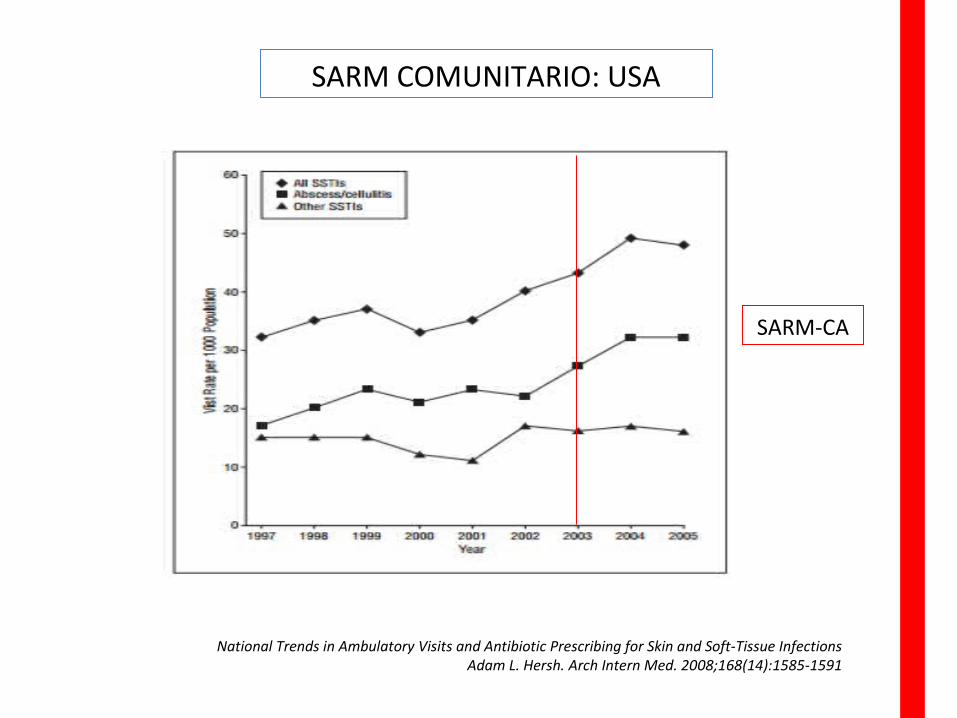
National Trends in Ambulatory Visits and Antibiotic Prescribing for Skin and Soft-Tissue Infections Adam L. Hersh. Arch Intern Med. 2008;168(14):1585-1591
SARM COMUNITARIO: USA
SARM-CA
Prevalencia del 11,2% (37 de 329 SARM)
36 casos de Infección de piel y partes blandas17 abscesos cutáneos7 celulitis 4 úlceras maleolares1 pie diabético1 infección de herida quirúrgica3 infecciones de herida traumáticas3 folicultiis o vesículas sobreinfectadas
Metástasis más frecuente que en SAMS
Elevada tasa de recidiva
Sensibles a antibióticos orales con actividad SARM (80 % de La cepas con CMI vanco >1,5)
Epidemiología y forma de presentación clínica de las infecciones originadas por Staphylococcus aureus resistente a meticilina productor de leucocidina de Panton-ValentineCobos-Trigueros et al. Revista Española de Quimioterapia 2010

Prevalencia de infecciones de piel y tejidos blandos producidas por Staphylococcus aureus resistente a Meticilina Comunitario en MadridBeatriz Casado-Verrier et al. Enferm Infecc Microbiol Clin. 2012
SARM COMUNITARIO
PREVALENCIABAJA
PROBLEMA RELATIVO
Problemas en el manejo de IPPB
3. Antibioterapia inicial
1. Identificación de la gravedad
2. Anticipación/Identificación de la etiología
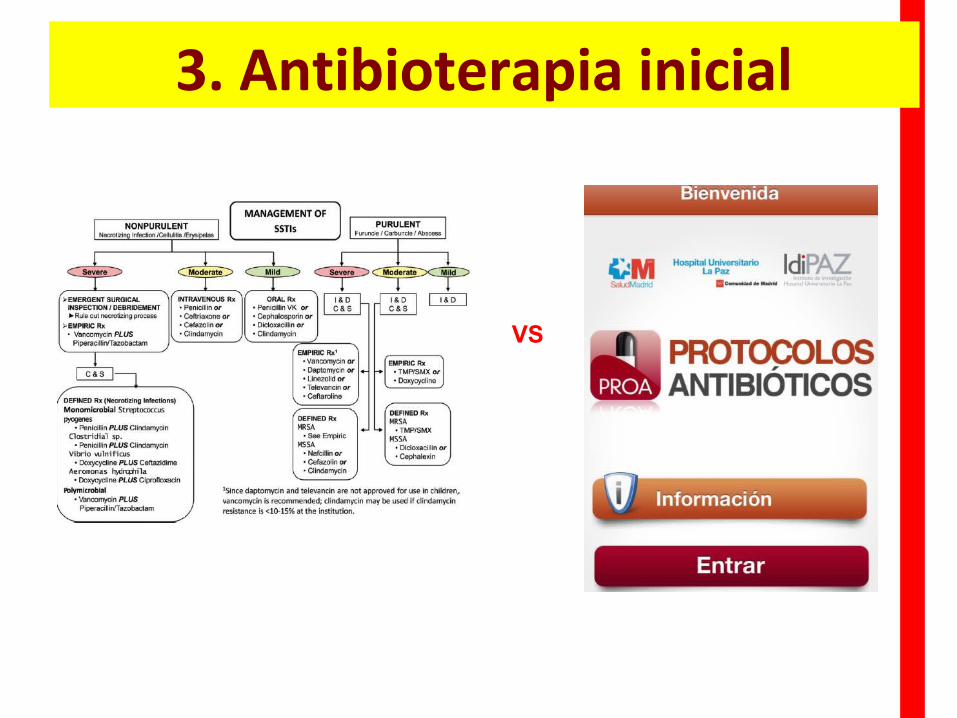
3. Antibioterapia inicial
VS
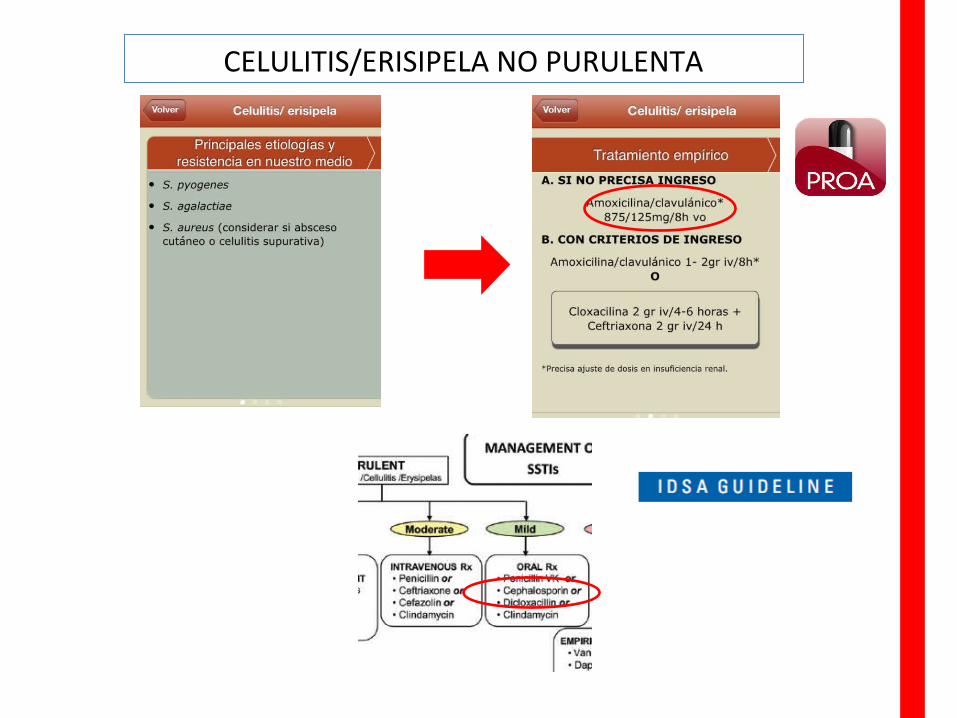
CELULITIS/ERISIPELA NO PURULENTA

¿Es necesario espectro para G-?
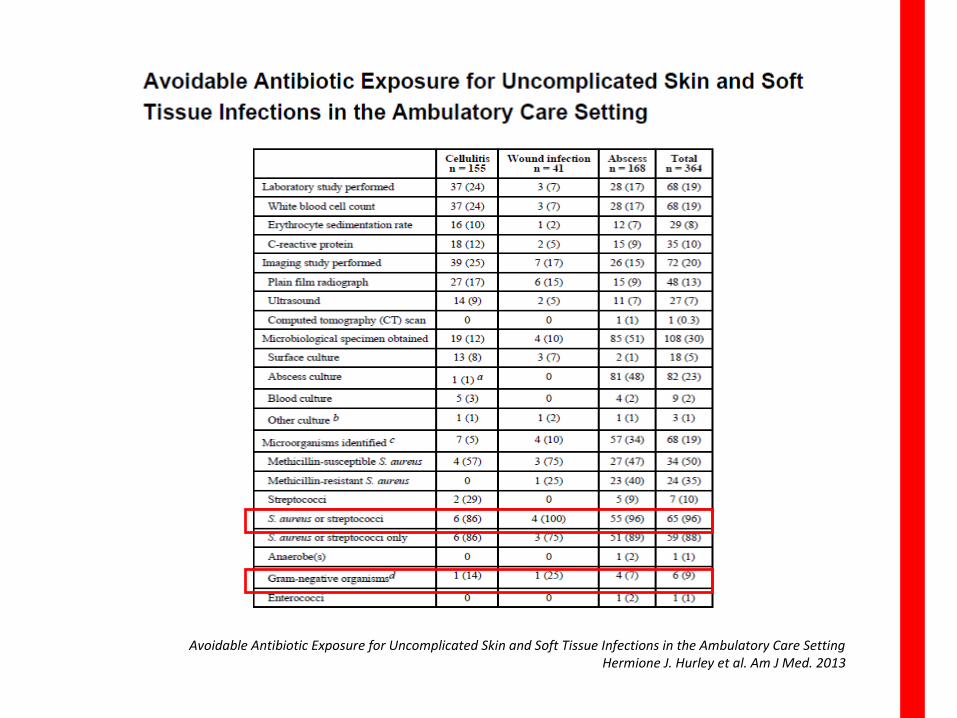
Avoidable Antibiotic Exposure for Uncomplicated Skin and Soft Tissue Infections in the Ambulatory Care SettingHermione J. Hurley et al. Am J Med. 2013
Avoidable Antibiotic Exposure for Uncomplicated Skin and Soft Tissue Infections in the Ambulatory Care SettingHermione J. Hurley et al. Am J Med. 2013
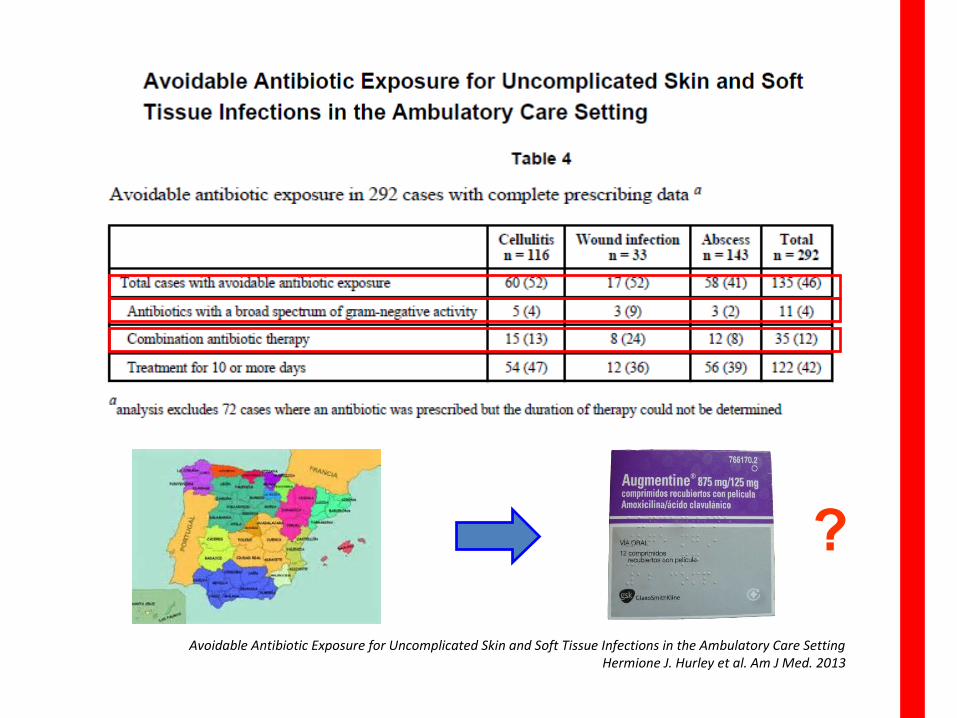
?
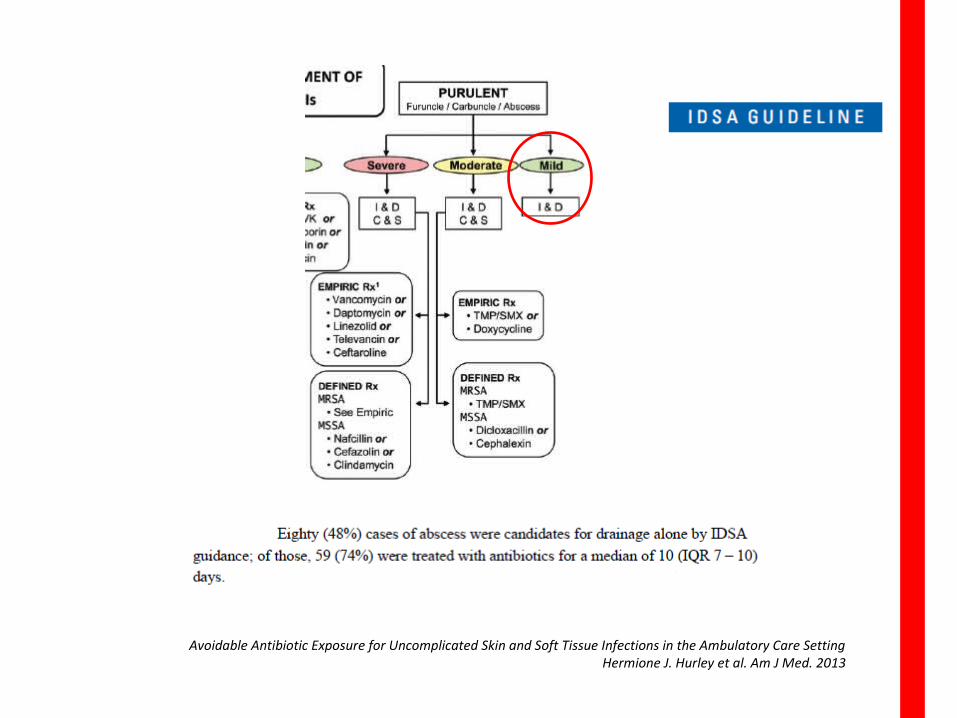
Avoidable Antibiotic Exposure for Uncomplicated Skin and Soft Tissue Infections in the Ambulatory Care SettingHermione J. Hurley et al. Am J Med. 2013
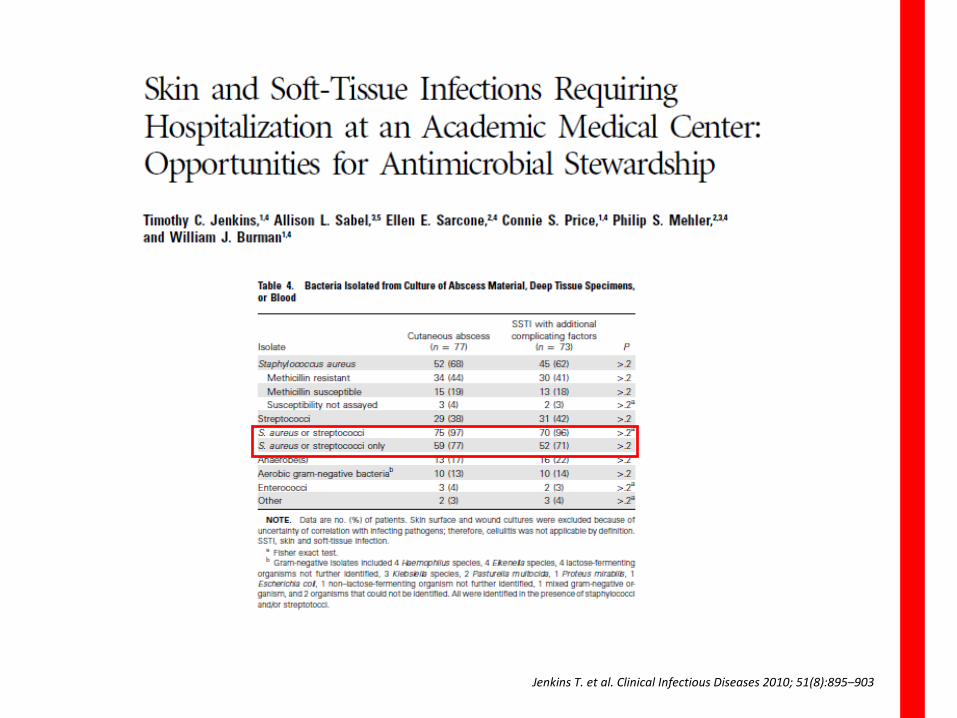
Jenkins T. et al. Clinical Infectious Diseases 2010; 51(8):895–903
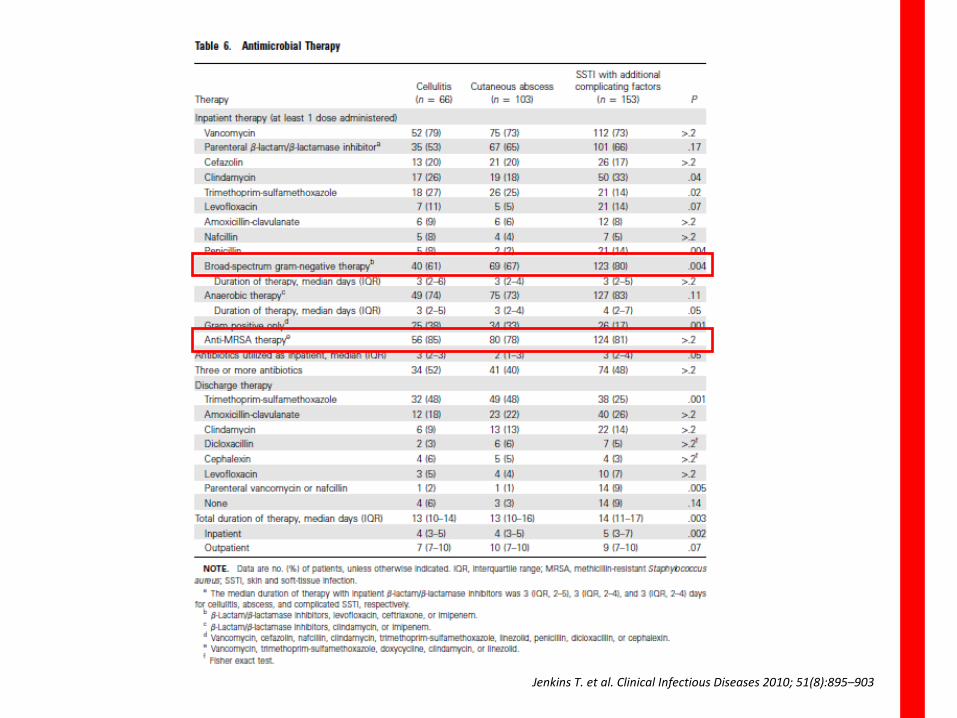
Jenkins T. et al. Clinical Infectious Diseases 2010; 51(8):895–903
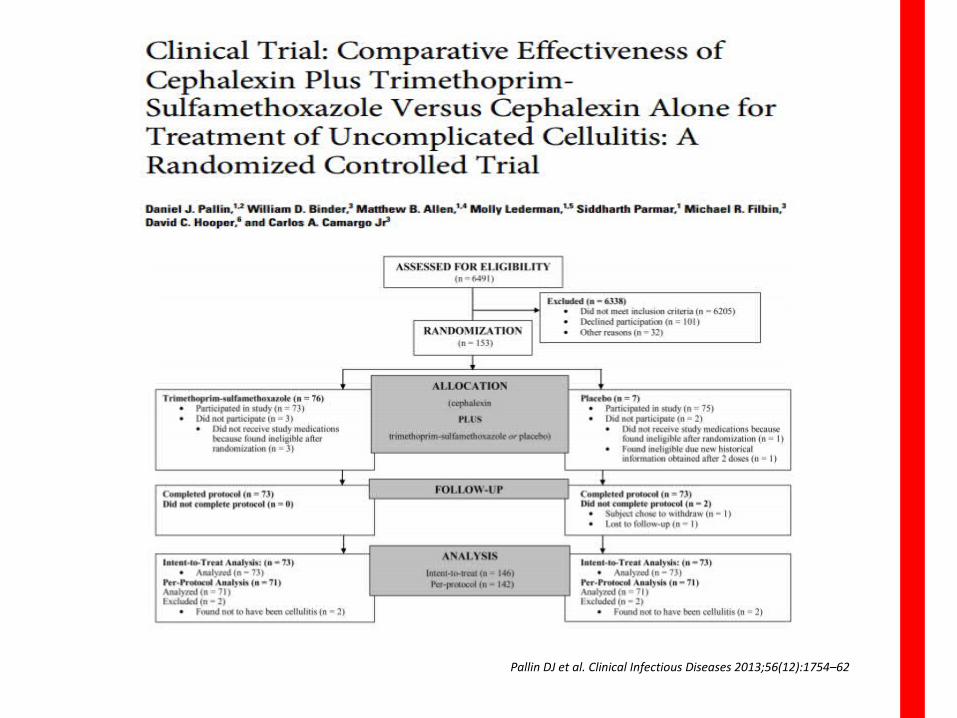
Pallin DJ et al. Clinical Infectious Diseases 2013;56(12):1754–62
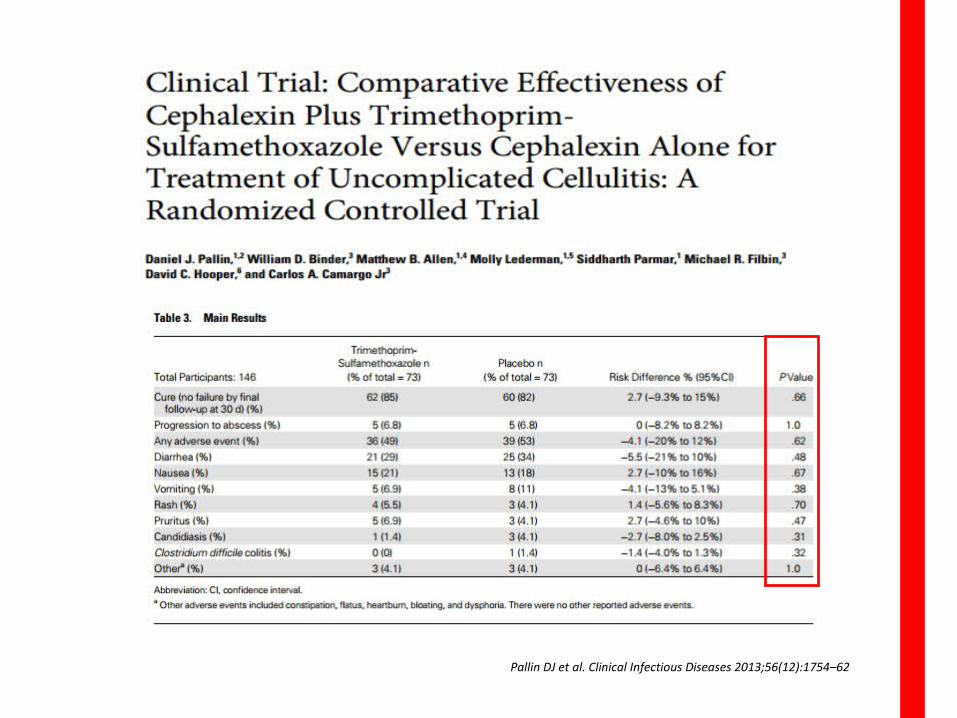
Pallin DJ et al. Clinical Infectious Diseases 2013;56(12):1754–62
Problemas en el manejo de IPPB
4. Ámbito sanitario
1. Identificación de la gravedad
2. Anticipación/Identificación de la etiología
3. Tratamiento antibiótico inicial
4. Ámbito sanitario
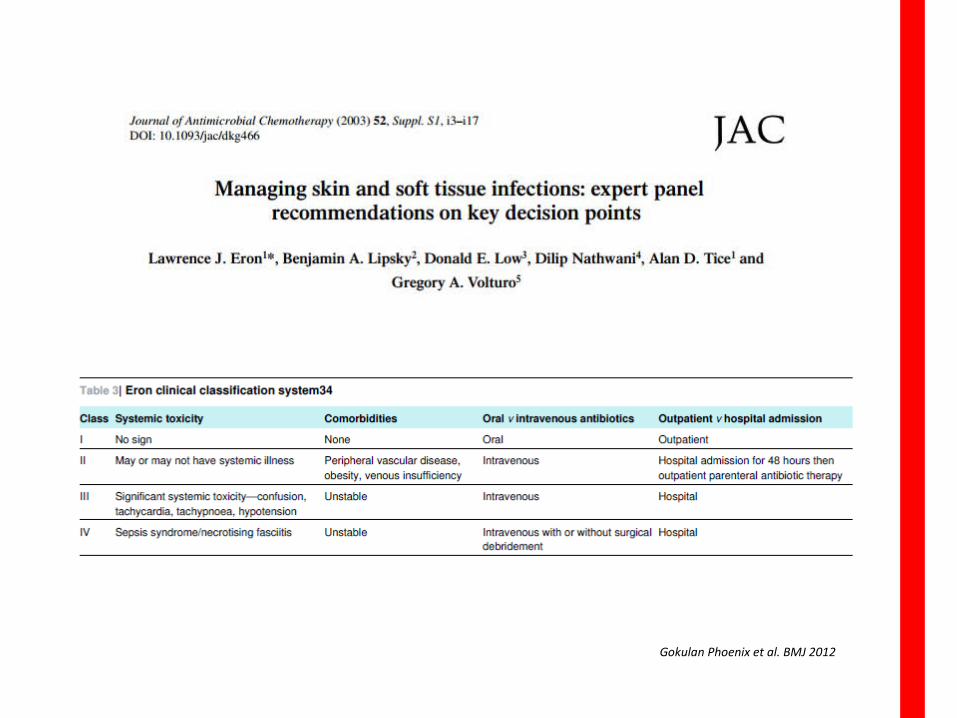
Gokulan Phoenix et al. BMJ 2012
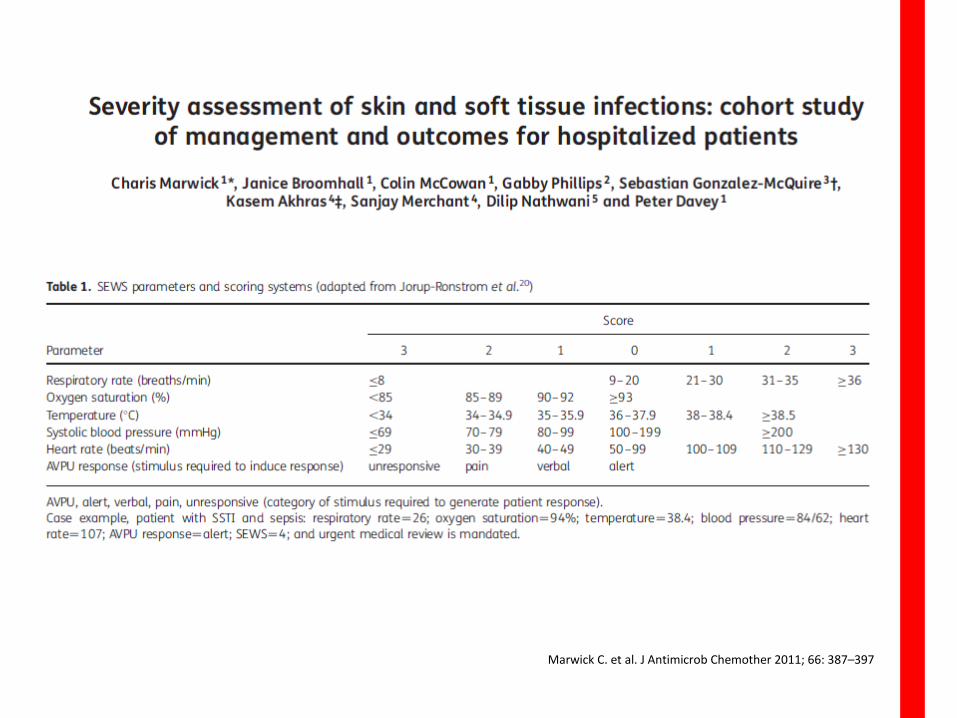
Marwick C. et al. J Antimicrob Chemother 2011; 66: 387–397
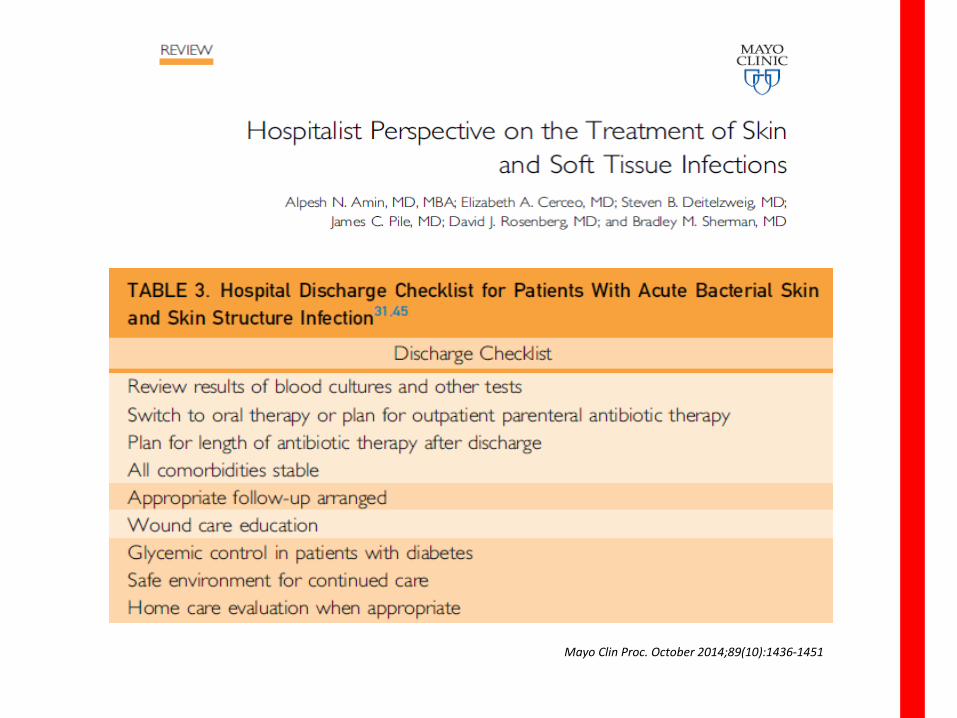
Mayo Clin Proc. October 2014;89(10):1436-1451
Problemas en el manejo de IPPB
5. Indicación quirúrgica: paciente/momento
1. Identificación de la gravedad
2. Anticipación/Identificación de la etiología
3. Tratamiento antibiótico inicial
4. Ámbito sanitario
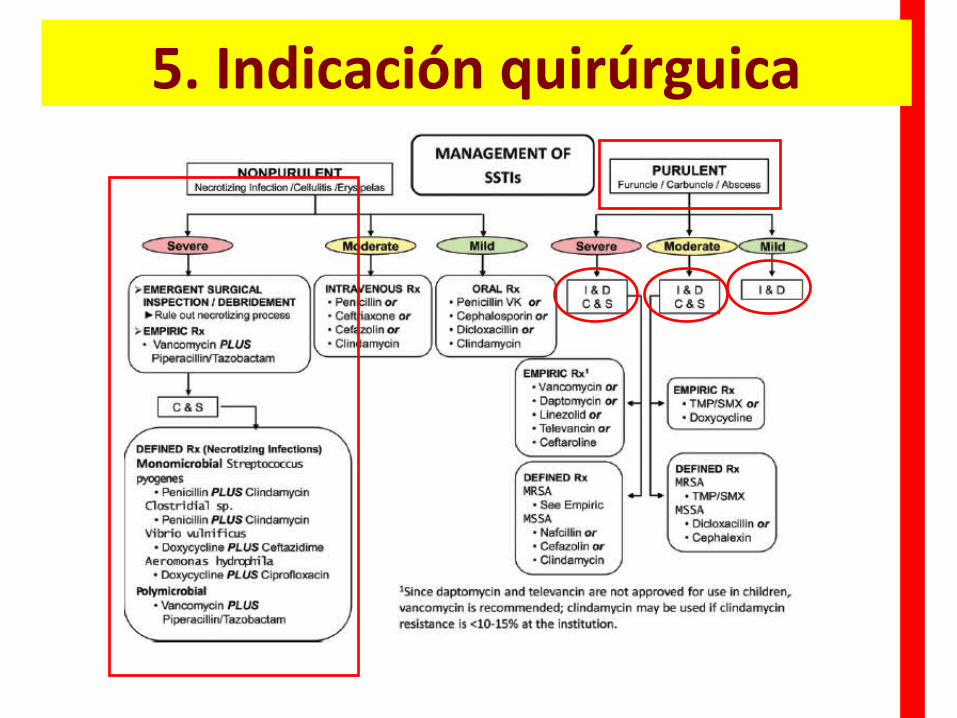
5. Indicación quirúrguica
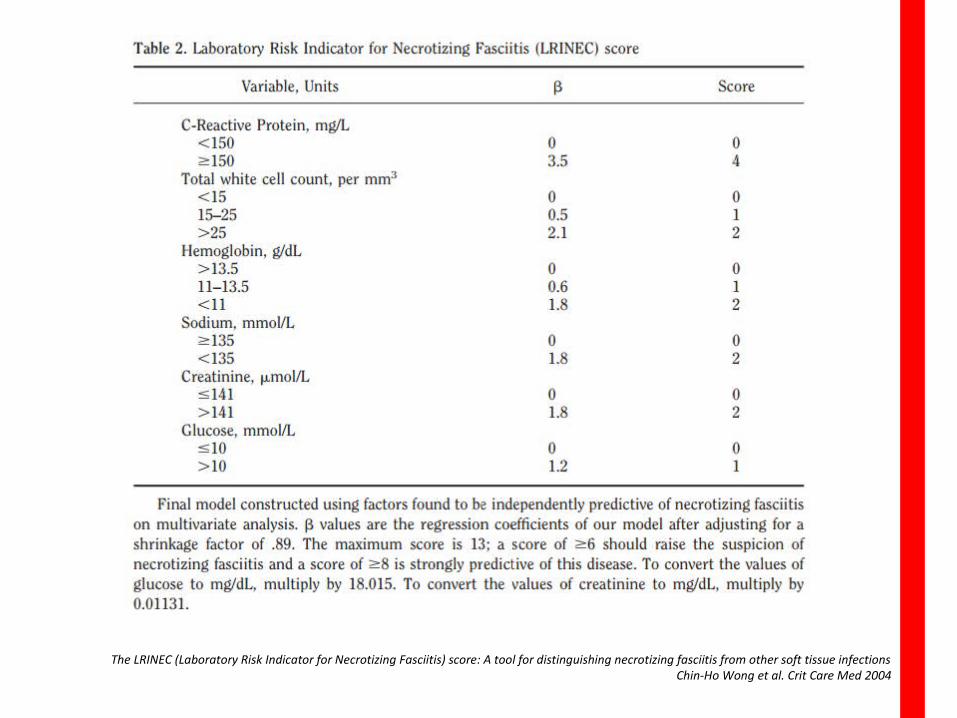
The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: A tool for distinguishing necrotizing fasciitis from other soft tissue infectionsChin-Ho Wong et al. Crit Care Med 2004
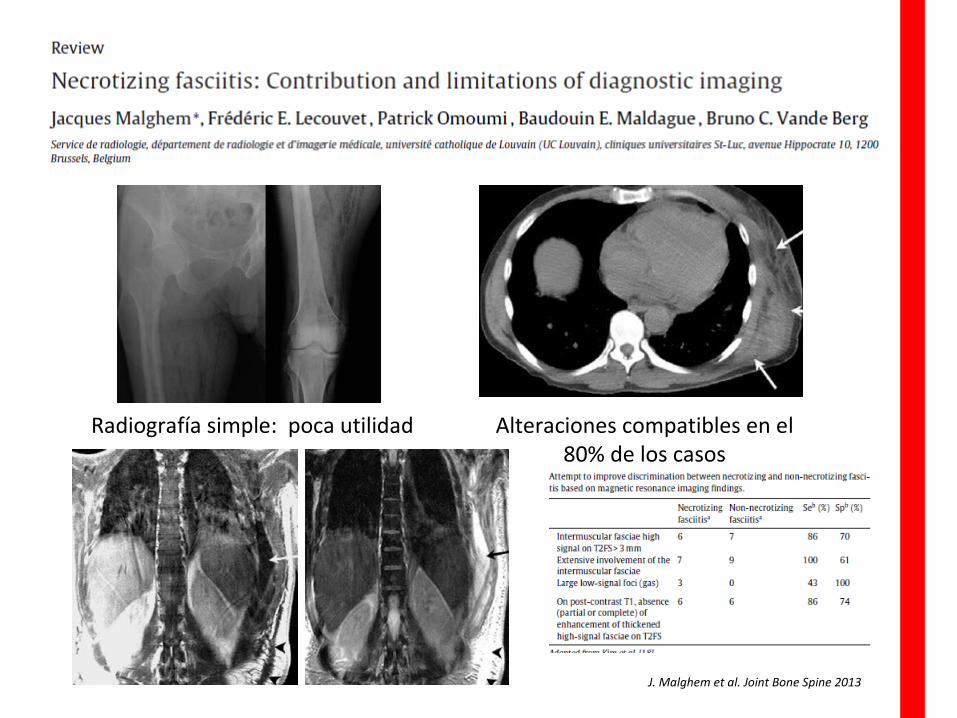
J. Malghem et al. Joint Bone Spine 2013
Radiografía simple: poca utilidad Alteraciones compatibles en el 80% de los casos
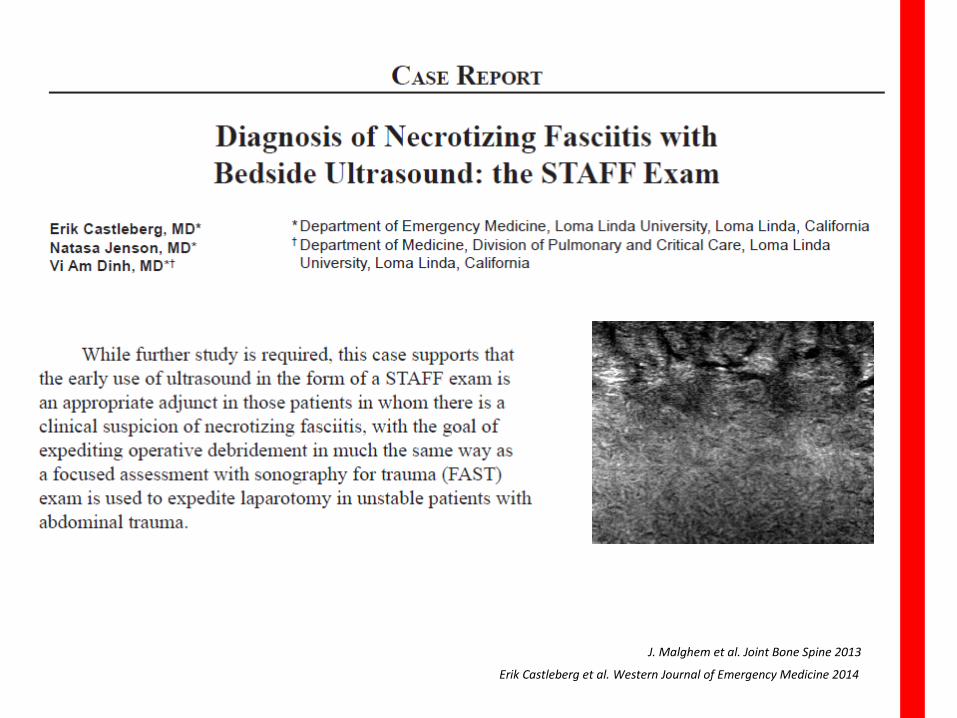
Erik Castleberg et al. Western Journal of Emergency Medicine 2014
J. Malghem et al. Joint Bone Spine 2013

CIRUGÍA
GOLD STANDARD DIAGNÓSTICO DE FASCITIS NECROTIZANTE
SIEMPRE REQUIERE CIRUGÍA
¿Cuándo esta indicado realizar un TC?¿ECO?
Problemas en el manejo de IPPB
6. Monitorización de la evolución
1. Identificación de la gravedad
2. Anticipación/Identificación de la etiología
3. Tratamiento antibiótico inicial
4. Ámbito sanitario
5. Indicación quirúrgica: paciente/momento
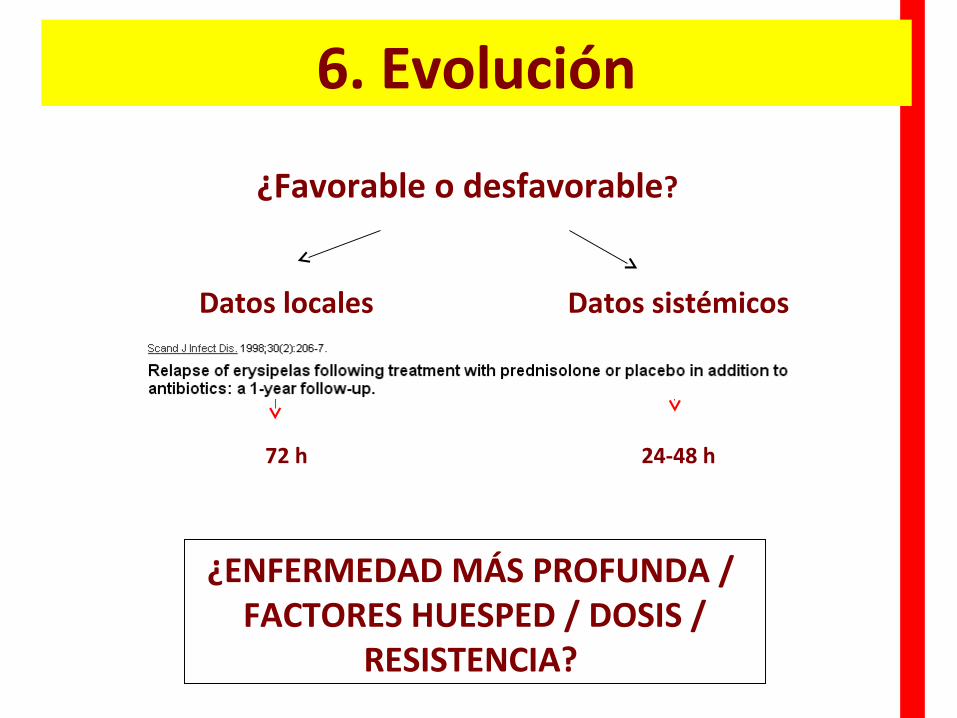
6. Evolución
¿Favorable o desfavorable?
Datos sistémicos
24-48 h
Datos locales
72 h
¿ENFERMEDAD MÁS PROFUNDA / FACTORES HUESPED / DOSIS /
RESISTENCIA?
Problemas en el manejo de IPPB
7. Ajuste antibiótico: tiempo/duración
1. Identificación de la gravedad
2. Anticipación/Identificación de la etiología
3. Tratamiento antibiótico inicial
4. Ámbito sanitario
5. Indicación quirúrgica: paciente/momento
6. Monitorización de la evolución
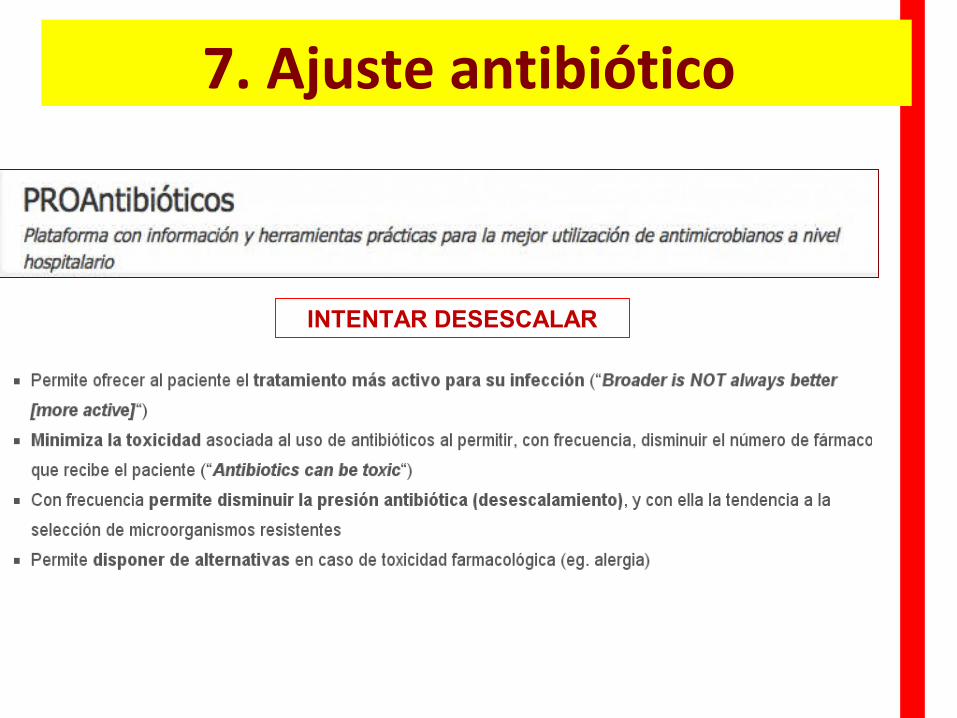
7. Ajuste antibiótico
INTENTAR DESESCALAR
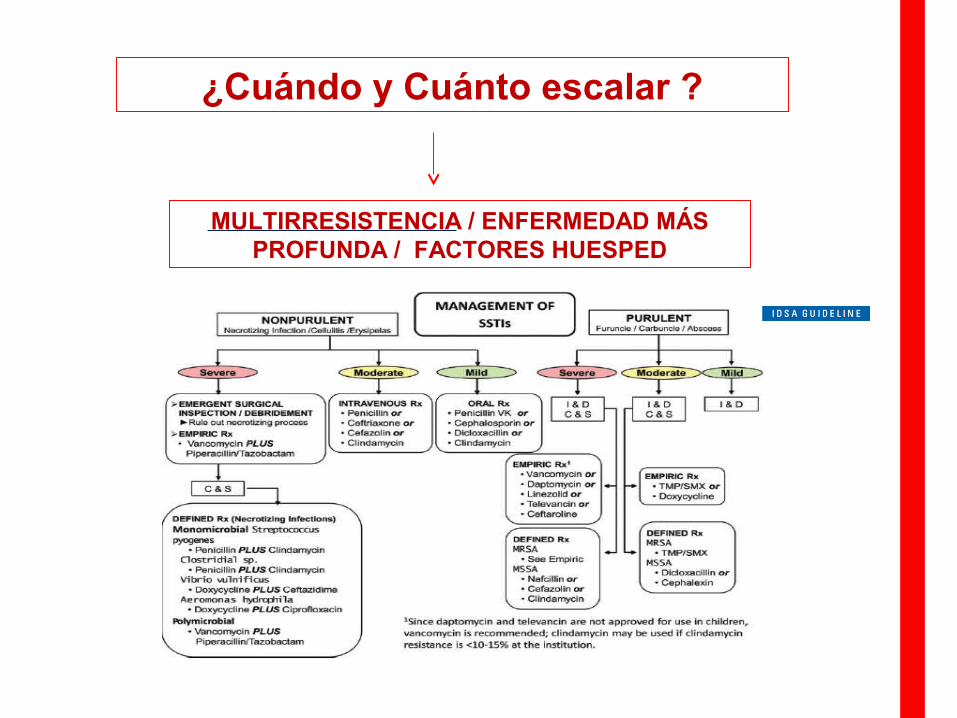
¿Cuándo y Cuánto escalar ?
MULTIRRESISTENCIA / ENFERMEDAD MÁS PROFUNDA / FACTORES HUESPED
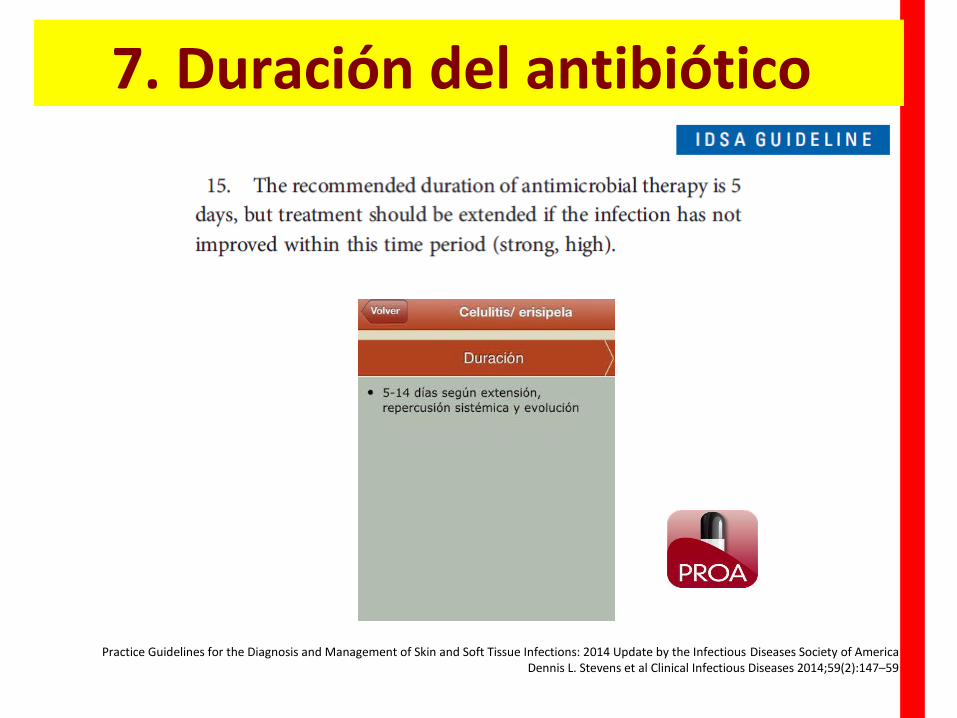
Practice Guidelines for the Diagnosis and Management of Skin and Soft Tissue Infections: 2014 Update by the Infectious Diseases Society of AmericaDennis L. Stevens et al Clinical Infectious Diseases 2014;59(2):147–59
7. Duración del antibiótico
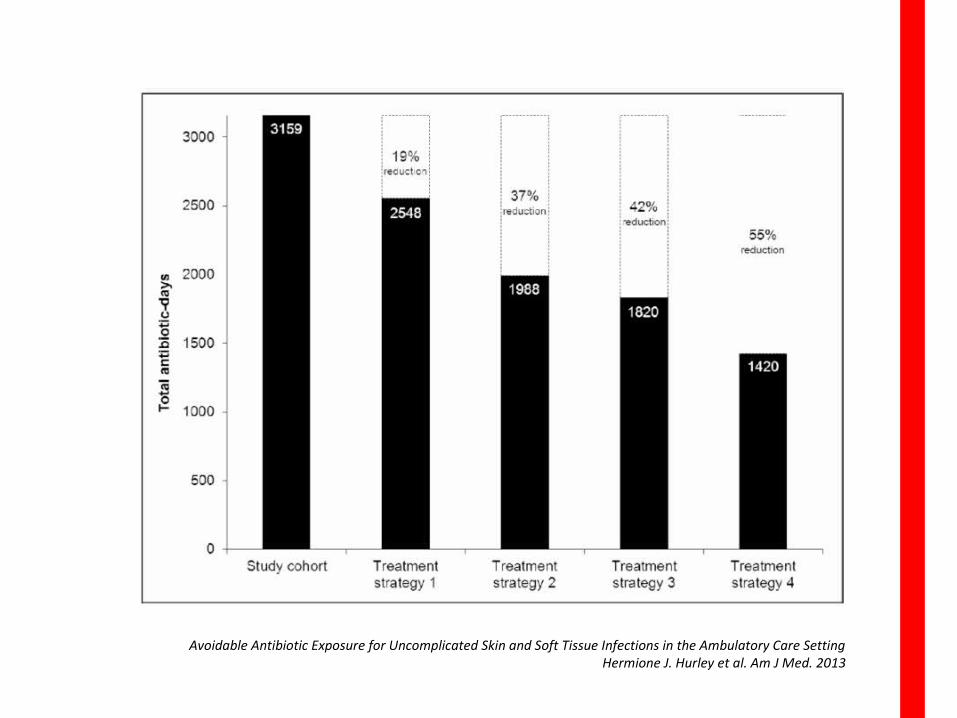
Avoidable Antibiotic Exposure for Uncomplicated Skin and Soft Tissue Infections in the Ambulatory Care SettingHermione J. Hurley et al. Am J Med. 2013

GRACIAS