Embed Size (px)
Citation preview

22 De Octubre Del 2013
Neuropatías Ópticas
Abraham Villalobos F. RMi

Introducción
✤ El nervio óptico posee 4 segmentos:
✤ Intraocular: retina. Axones y astrocitos, no mielinizado.
✤ Intraorbitario: 25 a 30mm. Dura, aracnoides y piamadre.
✤ Intracanalicular: 4 a 10 mm.
✤ Intracraneal: 16 mm.

Manifestaciones Clínicas
✤ Varía con cada etiología.✤ Disminución en la agudeza visual. Monocular.✤ Alteración en la saturación de los colores.
✤ Dolor: variable.
✤ Defecto pupilar aferente si la lesión es unilateral o asimétrica.
✤ Escotoma central.
✤ Papilitis (si hay compromiso del disco óptico).
✤ Atrofia, eventual, del nervio.

Etiología✤ Neuritis óptica es la causa más común en adultos jóvenes.
✤ Neuropatía óptica isquémica en mayores.Neuropatía óptica isquémicaArterítica
No arterítica
Neuritis ÓpticaInfeccionesNeurorretinitis: virus, toxoplasmosis, bartonella, otras.
Meningitis (cualquier causa)
Sífilis, enfermedad de Lyme
InflamatoriasParainfecciosa
Enfermedad sistémica autoinmune: LES, Sjögren, otras.
Paraneoplásica, sarcoidosis.
GenéticasNeuropatía óptica hereditaria de Leber
Neuropatía óptica autosómica dominante de Kjer
Compresivas
Absceso
Aneurisma de la rama oftálmica de la arteria carotídea
Oftalmopatía tiroidea
Pseudotumor orbitario
Pseudotumor cerebri
Tóxica/metabólica
Drogas
Toxinas
Deficiencia nutricional (Vitamina B1, B12, folato
Ambliopía por tabaco-alcohol
Radiación
Trauma

✤ Es la más común en pacientes mayores de 50 años.
✤ Anterior: afecta al nervio óptico.
✤ Posterior: retrobulbar.
✤ No arterítica:
✤ Es la más común.
✤ Pérdida aguda de la visión, monocular, indolora.
✤ Edema papilar.
Etiologías Neuropatía óptica isquémica

✤ No arterítica:
✤ Pobre perfusión por parte de la arteria ciliar posterior.
✤ Pacientes con HAS, DM, u otros factores de riesgo vasculares.
✤ Pérdida de agudeza visual al despertar por la mañana.
Neuropatía óptica isquémica

✤ No arterítica:
✤ Defecto en campo visual, altitudinal.
✤ No hay anormalidades en la RMI.
✤ Riesgo: 14.7% en 5 años para el ojo contralateral.
✤ Mal pronóstico. No hay manejo específico.
✤ No hay evidencia de la efectividad de la terapia antiplaquetaria.
Neuropatía óptica isquémica

✤ Arterítica:
✤ Pacientes mayores de 70 años.
✤ Usualmente debida a Arteritis de Células Gigantes.
✤ Polimialgia reumática: claudicación mandibular, artralgias, cefalea, fatiga.
✤ VSG y PCR aumentadas.
✤ EF: edema papilar, hemorragias peripapilares, oclusiones de las ramas de la arteria central de la retina o exudados cotonosos.
✤ Dx: biopsia de arteria temporal.
✤ Tratamiento: corticosteroides.
Etiologías Neuropatía óptica isquémica

✤ Enfermedad desmielinizante, inflamatoria.
✤ Asociada a Esclerosis Múltiple.
✤ 50% de estos pacientes la desarrollan.
✤ 20% inician de esta forma.
✤ Pérdida visual, monocular, subaguda.
✤ Dolor a la movilización: 92%.
✤ Pérdida de la saturación de los colores.
✤ Edades: 18 a 40 años.
✤ Los síntomas usualmente se desarrollan en pocos días, con severidad máxima dentro de 2 semanas.
✤ 2/3 son de afectación retrobulbar.
✤ 1/3 presentan papilitis.
✤ RMI: 95% presentan inflamación.
✤ Pronóstico: bueno.
✤ Tto. Metilprednisolona.
Neuritis Óptica

Neuritis Óptica
clinical pr actice
n engl j med 354;12 www.nejm.org march 23, 2006 1275
results in reduced constriction of the affected and contralateral pupils in reaction to light when the affected eye is stimulated during the swing-ing flashlight test. Absence of this finding in pa-tients with acute visual loss suggests retinal dis-ease (e.g., central serous retinopathy) or coincident optic-nerve dysfunction in the other eye.5-8
Visual-field loss is typical of acute demyelin-ating optic neuritis.21,25-27 Central scotomas are classic, but a more broad spectrum of patterns typically occurs, including diffuse defects (i.e., generalized depression of the entire central 30 degrees of the visual field) and focal defects.26,27 Altitudinal defects (visual-field loss above or be-low the horizontal meridian) are less common and should prompt consideration of a diagnosis of anterior ischemic optic neuropathy (Table 1). In addition to assessing visual acuity and the vi-sual field, low-contrast letter acuity (perception of light gray letters of progressively smaller size on a white background) and contrast sensitivity (minimum contrast level or shade of gray at which patients can perceive letters of a single large size) are methods used to detect visual dysfunction in patients with acute optic neuritis and multiple sclerosis.28-30 Although these tests are not rou-tinely performed in clinical practice, reductions in the scores for these measures have been dem-onstrated even in patients with visual acuities of 20/20 or better according to a Snellen chart.
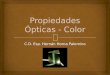
The optic disk appears normal in two thirds of patients with optic neuritis; these patients are said to have retrobulbar optic neuritis (Fig. 1A).21 When swelling (papillitis) is present in patients with optic neuritis (Fig. 1B), hemorrhages are uncommon. The presence of hemorrhages with swelling suggests alternative diagnoses, such as
anterior ischemic optic neuropathy (Table 1 and Fig. 1C).4 Lipid deposits, called retinal exudates, that result from optic-disk edema are rare and suggest a diagnosis of neuroretinitis. After weeks of follow-up, clinically observable atrophy of the optic-nerve head and thinning of the nerve-fiber layer of the surrounding retina may develop de-spite recovery of visual acuity.30
A
B
C
Figure 1. The Optic Disk in Acute Demyelinating Optic Neuritis.
In two thirds of cases, the optic disk appears normal (Panel A) and the patients are said to have retrobulbar optic neuritis. When optic-disk swelling (papillitis) is present (Panel B), it is mild and diffuse; there are no peripapillary hemorrhages, cotton-wool spots, or retinal exudates (lipid deposits) in this setting. Peripapillary hemorrhages, such as those seen in anterior ischemic optic neuropathy (Panel C, arrows), are associated with an extremely low risk or no risk of multiple sclerosis in patients with optic neuritis as a first demyelinating event and normal MRI of the brain.4 (Courtesy of Dr. Nicholas J. Volpe, Department of Ophthalmology, University of Pennsylvania School of Medicine, Scheie Eye Institute, Philadelphia.)
The New England Journal of Medicine Downloaded from nejm.org at Hinari Phase 1 sites -- comp on October 17, 2013. For personal use only. No other uses without permission.
Copyright © 2006 Massachusetts Medical Society. All rights reserved.

The New England Journal of Medicine Downloaded from nejm.org at Hinari Phase 1 sites -- comp on October 17, 2013. For personal use only. No other uses without permission.
Copyright © 1992 Massachusetts Medical Society. All rights reserved.
✤ Primer ECA en comparar tratamientos.
✤ 457 pacientes, 15 centros clínicos.
✤ 1º grupo: metilprednisolona 250 mg c/6hrs por 3 días seguidos de Prednisona a 1mg por kg/día por 14 días.
✤ 2º grupo: Prednisona 1mg/Kg/día por 11 días.
✤ 3º grupo: placebo vía oral.
The New England Journal of Medicine Downloaded from nejm.org at Hinari Phase 1 sites -- comp on October 17, 2013. For personal use only. No other uses without permission.
Copyright © 1992 Massachusetts Medical Society. All rights reserved.

The New England Journal of Medicine Downloaded from nejm.org at Hinari Phase 1 sites -- comp on October 17, 2013. For personal use only. No other uses without permission.
Copyright © 1992 Massachusetts Medical Society. All rights reserved.
The New England Journal of Medicine Downloaded from nejm.org at Hinari Phase 1 sites -- comp on October 17, 2013. For personal use only. No other uses without permission.
Copyright © 1992 Massachusetts Medical Society. All rights reserved.
✤ La función visual tuvo mejoría más rápida en el grupo de metilprednisolona comparada con placebo.
✤ No hubo diferencia en el grupo de prednisona oral vs placebo.
✤ El número de recurrencias fue mayor en el grupo de prednisona (RR 1.79, 95%IC 1.08 - 2.95).

clinical pr actice
n engl j med 354;12 www.nejm.org march 23, 2006 1279
on the basis of data in adults, treatment with intravenous methylprednisolone is generally rec-ommended if visual loss is unilateral and severe or is bilateral.20 Interferon therapy is considered in children with abnormal MRI scans of the brain, but data regarding the efficacy of therapy to prevent multiple sclerosis are lacking in this population.
Guidel ines
Practice parameters published by the Quality Standards Subcommittee of the American Acad-emy of Neurology note that intravenous methyl-prednisolone may hasten recovery of visual func-tion but that no evidence of long-term benefit exists.41 This practice guideline antedated the publication of the clinical trials of interferon.
Summ a r y a nd R ecommendations
The patient described in the vignette has signs and symptoms typical of acute monosymptom-atic demyelinating optic neuritis. Such patients should undergo evaluation with gadolinium-enhanced MRI of the brain to determine the risk
of the development of multiple sclerosis. If there are two or more white-matter lesions that are 3 mm or more in diameter, ovoid, and periven-tricular in location, which suggest a high risk of multiple sclerosis, treatment to reduce this risk should be strongly considered. I recommend in-travenous methylprednisolone (1 g per day for 3 days) followed by oral prednisone (1 mg per kilogram per day for 11 days, with subsequent tapering over a period of 4 days). This therapy is based on data suggesting that it is likely to has-ten recovery of visual function by two to three weeks and may reduce the risk of multiple sclero-sis within two years after the first episode of optic neuritis. Treatment with interferon beta-1a or interferon beta-1b should be strongly consid-ered after methylprednisolone treatment (Table 2), with the aim of further reducing or delaying de-velopment of multiple sclerosis during the long term. Oral prednisone alone may increase the risk for recurrent optic neuritis and should be avoided.
Dr. Balcer reports having received research fees from Biogen, Berlex, Centocor, and Serono. No other potential conflict of in-terest relevant to this article was reported.
I am indebted to Steven Galetta for helpful comments regard-ing the manuscript.
Table 2. Treatment Options for Acute Demyelinating Optic Neuritis in Patients at High Risk for Multiple Sclerosis.*
Treatment Standard Dosage Contraindications and Potential Side Effects
Short-term
Intravenous methylpred-nisolone
1 g daily for 3 days plus 1 mg/kg of body weight of oral prednisone daily for 11 days followed by 4 days of tapering (day 1, 20 mg; days 2 and 4, 10 mg)
Contraindications: systemic infection, im-munodeficiency, severe hypertension
Potential side effects: sleep disturbances, mild mood changes, stomach upset, weight gain, hyperglycemia, worsening hypertension
Long-term
Interferon beta-1a (Avonex)Interferon beta-1a (Rebif)Interferon beta-1b
(Betaseron)
30 µg intramuscularly once weekly22 µg subcutaneously once weekly 250 µg subcutaneously every other day
Contraindications: pregnancy, hypersensitivi-ty to interferon beta or human albumin
Potential side effects: influenza-like symp-toms (e.g., fever, chills, and myalgias, which may be treated symptomatically), depression, anemia, hepatic dysfunction, inflammation at the injection site of sub-cutaneous preparations
Monitoring: complete blood counts, liver function tests
* Characteristic demyelinating lesions in patients at risk for multiple sclerosis (indicating high risk in first episodes of acute optic neuritis) are 3 mm or larger in diameter, are ovoid, are located in periventricular areas of the white matter, and radiate toward the ventricular spaces.12-15
The New England Journal of Medicine Downloaded from nejm.org at Hinari Phase 1 sites -- comp on October 17, 2013. For personal use only. No other uses without permission.
Copyright © 2006 Massachusetts Medical Society. All rights reserved.
Laura J. Balcer. Optic Neuritis. New Eng J Med 2006, 354:1273-80

Infecciones
✤ Efecto directo del agente causal o secundaria a vasculitis.
✤ Virus del Oeste del Nilo.
✤ Síntomas: propios de infección en SNC.
✤ RMI + LCR sugerentes.
✤ Puede ser la primera manifestación en infecciones crónicas, indolentes (TB, criptococos, etc).
✤ Infección aislada: Toxoplasmosis, enfermedad por arañazo del gato.
✤ Neurorretinitis.

Infecciones
✤ Exploración física:
✤ Edema de mácula y papila.
✤ Exudados maculares en forma de estrella.
✤ Tto: esteroide + antibiótico sistémico.
✤ Sífilis
✤ Asociada a inflamación vítrea - uveítis posterior.
✤ Puede ser mono o binocular.
✤ Recurrencia en el 50% de los casos.

✤ Parainfecciosa:
✤ Sarampión, parotiditis, varicela, influenza, virus de Epstein-Barr
✤ De 1 a 3 semanas posteriores.
✤ Fenómeno postvacunación (<1%).
✤ Más común en niños.
✤ Bilateral.
✤ Papilitis con retinitis.
✤ Pronóstico: bueno, aún sin tratamiento.
✤ Bilateral: Síndrome de Guillain - Barré.
Etiología Inflamatoria

✤ Sarcoidosis:
✤ En 5% puede ser manifestación inicial.
✤ Bilateral en 24 a 64% de los casos.
✤ Clínica similar a neuritis óptica.
✤ El disco óptico puede tener apariencia nodular.
✤ RM: engrosamiento del nervio óptico, generalizado, de forma nodular --> menínges + otras lesiones en parénquima.
✤ Pronóstico: variable.
Etiología Inflamatoria

✤ Enfermedades autoinmunes:
✤ LES: 1% de los pacientes.
✤ Secundaria a vasculitis o SAAF asociado a LES.
✤ Síndrome de Sjögren: 16% pueden presentarlo. Neuritis óptica.
✤ Granulomatosis de Wegener: Secundaria a extensión de la inflamación en áreas paranasales.
✤ Enfermedad de Behçet: Uveítis --> Meningitis. La NO es rara.
✤ EII: puede sugerir otras patologías autoinmunes.
✤ Paraneoplásica: reporte de casos. Asociada a cáncer pulmonar de células pequeñas.
Etiología Inflamatoria
Delalande S, de Seze J, Fauchais AL, et al. Neurologic manifestations in primary Sjögren syndrome: a study of 82 patients. Medicine (Baltimore) 2004; 83:280.

✤ Existe pérdida gradual de la visión.
✤ El grado de dolor es variable.
✤ RM: hace el diagnóstico.
✤ El uso de esteroide mejora la visión, al disminuir el edema.
✤ Neoplasia:
✤ Masas selares o supraselares: adenoma pituitaria, craneofaringioma, meningioma, lesiones metastásicas, meningiomas en el nervio óptico.
✤ Linfoma.
Etiología Compresiva

✤ Otros:
✤ Oftalmopatía distiroidea.
✤ Aneurisma de la arteria oftálmica.
✤ Absceso.
✤ Hipertensión intracraneal idiopática o Pseudotumor cerebri.
Etiología Compresiva

✤ Neuropatía óptica hereditaria de Leber:
✤ Subaguda e indolora. Bilateral. Progresa en semanas - meses.
✤ 80 a 90% de los casos son varones jóvenes.
✤ Mutación del DNA mitocondrial (11, 778; 3460; 14,484) (complejo I).
✤ EF: telangiectasias circunpapilares.
✤ 1/3 puede ser normal.
✤ Pronóstico: depende de la mutación.
Etiología Genética

✤ Neuropatía óptica hereditaria de Leber:
✤ Subaguda e indolora. Bilateral. Progresa en semanas - meses.
✤ 80 a 90% de los casos son varones jóvenes.
✤ Mutación del DNA mitocondrial (11, 778; 3460; 14,484) (complejo I).
✤ EF: telangiectasias circunpapilares.
✤ 1/3 puede ser normal.
✤ Pronóstico: depende de la mutación.
Etiología Genética

Etiología Tóxicas y metabólicasToxinas
Monóxido de Carbono
Etilenglicol
Metanol
Percloroetileno
Toabaco
Tolueno
Estireno
Fármacos (efecto directo en el nervio óptico: Antimicrobianos.Clioquinol
Cloranfenicol
Dapsona
Etambutol
Isoniazida
Yoclorhidroxiquinoleína
Linezolid
Inmunomoduladores
Ciclosporina
Tacrolimus (FK506)
Alfa - interferón 2b
Quimioterapia
5-Fluorouracilo
Cisplatino
Carboplatino
Nitrosureas
Paclitaxel
Vincristina
Otros
Amiodarona
Clorpropamida
Benoxaprofeno
Cimetidina
Disulfiran
Melatonina, sertralina (Zoloft).
Efecto indirecto de fármacos
Sildenafil
Infliximab

✤ La mayoría presentan pérdida de la visión severa y permanente.
✤ Nutricional:
✤ Vitaminas B12, B1 y folatos.
✤ Se exacerban por tabaco y probablemente por alcoholismo.
✤ Uni o bilateral.
✤ Aguda y de progresión lenta.
✤ RM: normal.
✤ Pronóstico: reservado, aún con tratamiento.
Etiología Tóxicas y metabólicas

✤ Radiación
✤ Puede ocurrir 6 a 24 meses posterior a ésta.
✤ Raras con dosis menores a 50 Gy.
✤ Lenta en progresión.
✤ RM: hiperintensidad a nivel de nervio óptico.
✤ No hay tratamiento.
✤ Trauma
✤ En segmento intraorbitario e intracanalicular.
✤ Pronóstico: depende de la extensión del trauma.
✤ Tto: descompresión + corticosteroides.
Etiología Tóxicas y metabólicas

✤ Metanol
✤ CH3 OH
✤ Ácido fórmico: causa daño a nivel mitocondrial en las células del nervio óptico.
✤ Síntomas tipo Parkinson.
✤ Pronóstico: malo.
✤ Tratamiento: manejo de acidosis metabólica.
Etiología Tóxicas y metabólicas
then converts the aldehyde to a corresponding carboxylic acid. For methanol, thisreaction sequence can be represented as37:
Methanol Formaldehyde Formic acid
CH3– OH
dehydrogenase Aldehyde
NAD+
NADH + H+
H2O
H– C– OH
OO
H– C– H
Alcohol dehydrogenase
NAD+
NADH + H+
Conversion of methanol to formaldehyde occurs slowly, and constitutes the rate-limiting step of this reaction sequence. Both formaldehyde and formic acid are cyto-toxic, but formaldehyde, with a half-life of 1 to 2 minutes, is present only transientlyand does not accumulate. The formic acid molecule largely dissociates, releasinga hydrogen cation and a formate anion:
Formate Formic acid
H+
+OHH
O
C OH C
O
The released hydrogen ion lowers the pH of body fluids, and formate accumulatesbecause it is only slowly metabolized to carbon dioxide or excreted by the kidney.Much of the resulting hydrogen ion production from this dissociation reaction isneutralized by bicarbonate ions present in body fluids, depleting bicarbonate andgenerating carbon dioxide, which is excreted by the lungs:
Because the buffering of hydrogen ions is incomplete, hydrogen ion accumulationalso occurs, resulting in acidemia.Formate exerts its cytotoxic effects, at least in part, by inhibiting cytochrome aa3
and cytochrome c oxidase and thereby interfering with intramitochondrial electrontransport.38–42 This interference does not cause cellular hypoxia, but it preventsoxygen use by mitochondria, slowing or stopping oxidative phosphorylation in themanner similar to that of cyanide or carbon monoxide.42 Although tissue oxygenationmay increase because of continued tissue oxygen delivery and decreased cellularuptake, the end effect is similar to that of hypoxia in that there is decreased aerobicproduction of adenosine triphosphate (ATP). Thus, formate inhibits and preventsATP-requiring intracellular reactions from taking place, compromising cellular functionand homeostasis. Critical degrees of interference with these cytochromes result incellular injury and death. The CNS seems to be especially sensitive to the toxic effectsof formate. Retinal and optic nerve neurons, perhaps because of peculiarities in theirmitochondrial density, may be particularly susceptible to the adverse effects offormate.38,43–49 The basal ganglia, particularly the putamen, and subcortical whitematter also seem to have greater sensitivity to formate toxicity.50–54
The metabolism of ethylene glycol is more complex than methanol. As with meth-anol, alcohol dehydrogenase acts to oxidize a hydroxyl-containing carbon atom toa corresponding aldehyde55:
Glycoaldehyde Ethylene glycol
Alcohol dehydrogenase NAD
+HHDAN
+C
CH2OH
HO
CH2OH
CH2OH
++ +
Methanol and Ethylene Glycol Intoxication 667
symptoms following methanol ingestion who respondedto levodopa.In 2007, we reported a case of severe methanol
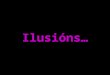
poisoning requiring hemodialysis, where the patientdeveloped delayed onset extrapyramidal dysfunction.6 Onday six post-ingestion, the patient was noted to havesymptoms and signs of a Parkinsonian syndrome; brainMRI done on day 13 post-intoxication confirmed bilateralbasal ganglia damage (Fig. 2). Additionally, this patientalso demonstrated respiratory muscle stiffness/weaknesswith reduced inspiratory and expiratory mouth pressures onformal pulmonary function testing, which did not objec-tively improve on levodopa therapy.6 Table 3 summarizesthe reported cases of delayed neurological sequelae frommethanol poisoning.
Mechanisms of toxicity
A number of mechanisms have been hypothesized toexplain why methanol intoxication produces basal gangliahemorrhage. These include high concentrations of formicacid in the basal ganglia leading to necrosis andimpairment of mitochondrial cytochrome oxidase, causinga myelinoclastic effect2,38,39,40; reduced venous drainageor inadequate arterial blood flow39; hypoxemia39; hypo-tension39; acidosis39; and the heparin therapy used duringhemodialysis.39 Studies of methanol toxicity in animals(e.g. mice, dogs and rabbits) that clear formate quickly donot develop acidosis or damage to the optic nerve orbasal ganglia.45 Primates, or the Yucatan micro pig(which has a unique inability to clear formate, since itpossesses the lowest hepatic folate concentrations of anyanimal species studied) are more closely related tohumans with regard to formate metabolism.45 Futureresearch should involve the study of the pathogenesis ofmethanol-induced Parkinsonian syndrome in these animalmodels, to yield a better understanding of this diseaseprocess in humans.
Conclusions
Though uncommon, delayed neurological sequelae havebeen reported following ingestion of ethylene glycol,diethylene glycols and methanol. These complicationsmanifest several days or weeks following acute intoxication.The observed anatomical and functional neurologicaldefects appear multi-factorial in origin. Formic acid isimplicated in the optic nerve damage from methanol.Oxalate crystal deposition likely causes the cranial neuro-pathies related to ethylene glycol. 2-hydroxyethoxyaceticacid is thought to be the causal moiety in cranialneuropathies resulting from diethylene glycol toxicity.However, it remains unclear why the facial nerve is thecranial nerve most commonly involved or why the basalganglia appear most predisposed to damage. The occurrenceof renal failure seems to be a risk factor for development ofdelayed neurotoxicity in ethylene glycol and diethyleneglycol poisoning.
Declaration of interest
The authors report no conflicts of interest. The authorsalone are responsible for the content and writing of thepaper.
References
1. Cavender FL, Sowinski EJ. Glycols. In: Clayton GD, Clayton FEeditors. Patty’s Industrial Hygiene and Toxicology. New York: JohnWiley & Sons Inc; 1994:4645–4719.
2. Lewis LD, Smith BW, Mamourian AC. Delayed sequelae after acuteoverdoses or poisonings: cranial neuropathy related to ethylene glycolingestion. Clin Pharmacol Ther 1997; 61:692–699.
3. Berger JR, Ayyar DR. Neurological complications of ethylene glycolintoxication. Report of a case. Arch Neurol. 1981; 38:724–726.
4. Walder AD, Tyler CK. Ethylene glycol antifreeze poisoning. Threecase reports and a review of treatment. Anesthesia 1994; 49:964–967.
5. Hanston P, Vanbinst R, Mahieu P. Determination of ethylene glycoltissue content after fatal oral poisoning and pathologic findings. Am JForen Med Pathol 2002; 23:159–161.
6. Reddy NJ, Lewis LD, Gardner TB, Osterling W, Eskey CJ,Nierenberg DW. Two cases of rapid onset Parkinson’s syndromefollowing toxic ingestion of ethylene glycol and methanol. ClinPharmacol Ther 2007; 81:114–121.
7. Morgan BW, Ford MD, Follmer R. Ethylene glycol ingestionresulting in brainstem and midbrain dysfunction. J Toxicol ClinToxicol 2000; 38:445–451.
8. Spillane L, Roberts JR, Meyer AE. Multiple cranial nerve deficitsafter ethylene glycol poisoning. Ann Emerg Med 1991; 20:208–210.
9. Palmer BF, Eigenbrodt EH, Henrich WL. Cranial nerve deficit: a clueto diagnosis of ethylene glycol poisoning. Am J Med 1989; 87:91–92.
10. Mallya KB, Mendis T, Guberman A. Bilateral facial paralysisfollowing ethylene glycol ingestion. Can J Neurol Sci 1986; 13:340–341.
11. Marczynska-Wolanska H, Hasiec T, Ksiazek A. Bilateral peripheralfacial nerve palsy in acute poisoning with ethylene glycol. Pol TygLek (in Polish) 1989; 44(46–48):965–6,976.
12. Fellman DM. Facial diplegia following ethylene glycol. Arch Neurol1982; 39:739–740.
Table 3. Delayed neurological sequelae from methanol poisoning.
Study n
Days todevelopment
of neurotoxicity Features
Reddy et al.6* 1 6 Parkinsonism, basalganglia injury
Guggenheimet al.42
1 NA Severe bilateral opticatrophy, rigidityhypokinesis
Passma et al.43 15 NA Visual disturbance,polyneuropathy,encephalopathy,ataxia, paraesthesiae
Hovda et al.44 5 NA Visual disturbances
NA, not available.*A case of ethylene glycol-related Parkinsonism is also reported here.
972 N.J. Reddy et al.
Clinical Toxicology vol. 48 no. 10 2010
Clin
ical
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
HIN
AR
I on
10/1
6/13
For p
erso
nal u
se o
nly.
presenting with or developing renal failure may go on toexhibit significant central and peripheral neurologicalcomplications several days to weeks following exposure.Early diagnosis and prevention of the complications ofacidemia and renal failure by administration of fomepizoleis paramount.
Methanol
Methanol (CH3 OH) also known as ‘‘wood alcohol’’ is ahighly toxic component of common commodities such aswindshield washer fluid, gasoline, de-icers, antifreeze, andpaint.37
Metabolism
The toxicity of methanol ingestion in humans is primarilymediated through its metabolites. Methanol is metabolized
by alcohol dehydrogenase to formaldehyde, which is thenconverted by aldehyde dehydrogenase to formic acid. It is theformic acid that is thought to account for the major pro-portion of the anion gap in patients with methanol-inducedacidosis.37,38 Furthermore, formic acid has been hypothe-sized to cause optic nerve damage at the level of the mito-chondrion in patients with toxic methanol ingestions.39–41
Features
Several authors have described long-term sequelae withParkinsonian symptoms in patients following toxicmethanol ingestions. McLean et al.38 reported twosurvivors of severe methanol poisoning who developed(in addition to blindness), a Parkinsonian-like extrapyr-amidal syndrome. Levodopa administered to the moreseverely affected patient had no effect on the extrapyr-amidal features. However, Guggenheim et al.42 reporteda 13-year-old girl with delayed-onset Parkinsonian
Fig. 2. MRI of the brain on day 13 post-methanol ingestion. FLAIR image (A) show edema in the basal ganglia, predominantly theputamen and globus pallidus bilaterally. T1-weighted images show hyperintense signal (B) and striking post contrast enhancement (C).Gradient echo image (D) shows bands of hemorrhage in the putamen.6
Delayed neurological sequelae 971
Clinical Toxicology vol. 48 no. 10 2010
Clin
ical
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
HIN
AR
I on
10/1
6/13
For p
erso
nal u
se o
nly.

Bibliografía
✤ Glaser JS. Topical diagnosis: Prechiasmal visual pathways. In: Neuro-ophthalmology, Glaser JS (Ed), JB Lippincott, Philadelphia 1990. p.83.
✤ Liu GT. Visual loss: optic neuropathies. In: Neuro-Ophthalmology: Diagnosis and Management, Liu GT, Volpe NJ, Galetta SL (Eds), WB Saunders, Philadelphia 2001.
✤ Lee AG, Brazis PW. Systemic infections of neuro-ophthalmic significance. Ophthalmol Clin North Am 2004; 17:397.
✤ Pawate S, Moses H, Sriram S. Presentations and outcomes of neurosarcoidosis: a study of 54 cases. QJM 2009; 102:449.
✤ Sadun AA. Metabolic optic neuropathies. Semin Ophthalmol 2002; 17:29.
✤ Nandy J, Reddy et al. Delayed neurological sequelae from ethylen glycol, diethylene glycol an methanol poisonings.Clinical Toxicology (2010) 48, 967-973.