Embed Size (px)
Citation preview
¿Qué hacer ?
¿Cómo evaluarla ?
Prof Dr Ricardo E Ronderos FASE FACC
Director Instituto de Cardiologia La Plata
Jefe Serv de Diagnostico por Imágenes Cardiovasculares
ICBA
Director Magister US en Cardiologia
Universidad Nacional de La Plata
Argentina
ESTENOSIS VALVULAR AORTICA
ASINTOMATICOS
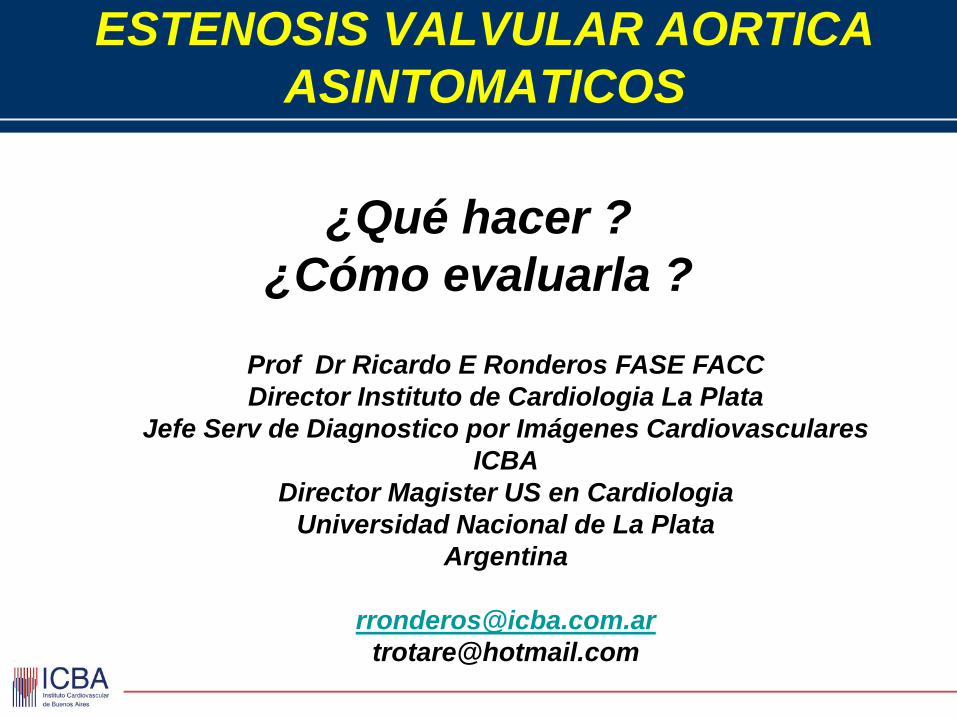
ESTENOSIS VALVULAR AORTICA ETIOLOGIA
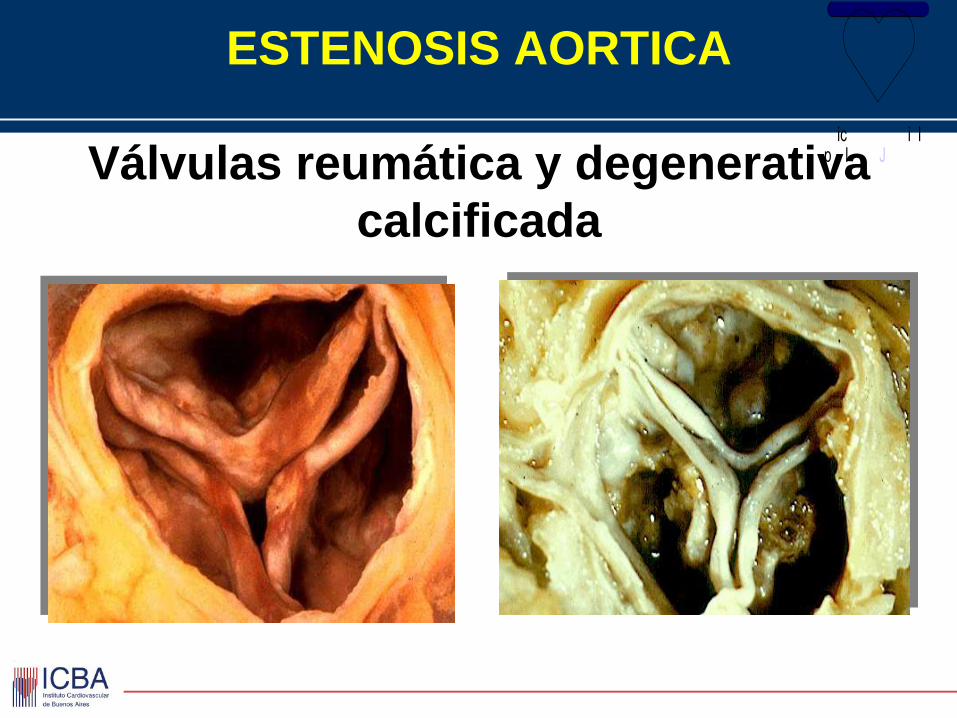
ESTENOSIS AORTICA
Válvulas reumática y degenerativa
calcificada
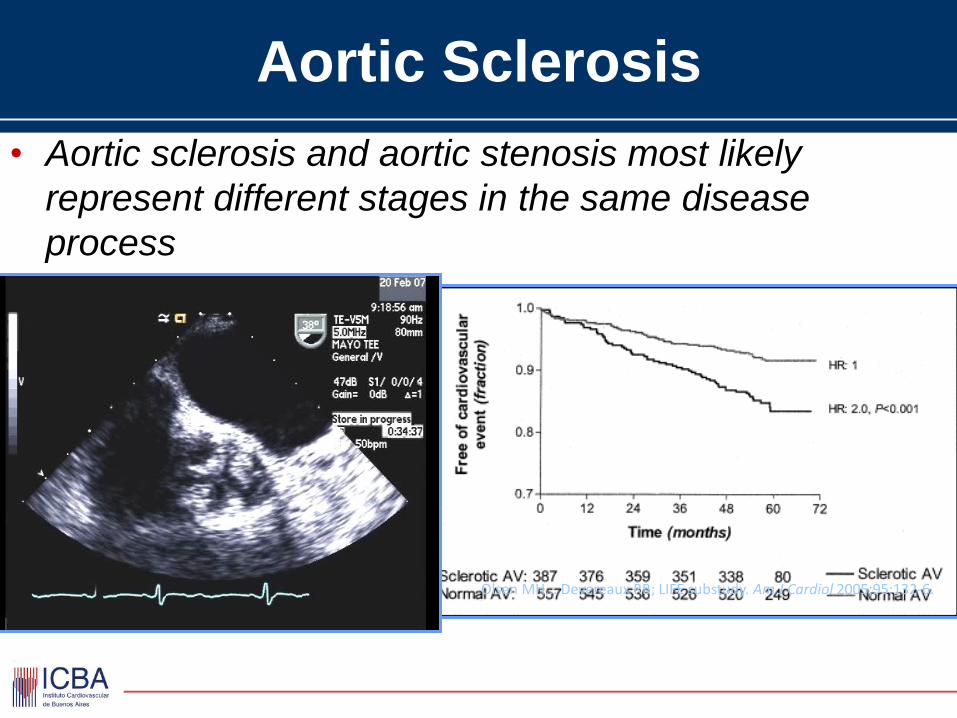
Aortic Sclerosis
• Aortic sclerosis and aortic stenosis most likely
represent different stages in the same disease
process
Olsen MH... Devereaux RB; LIFE substudy. Am J Cardiol 2005;95:132-6.
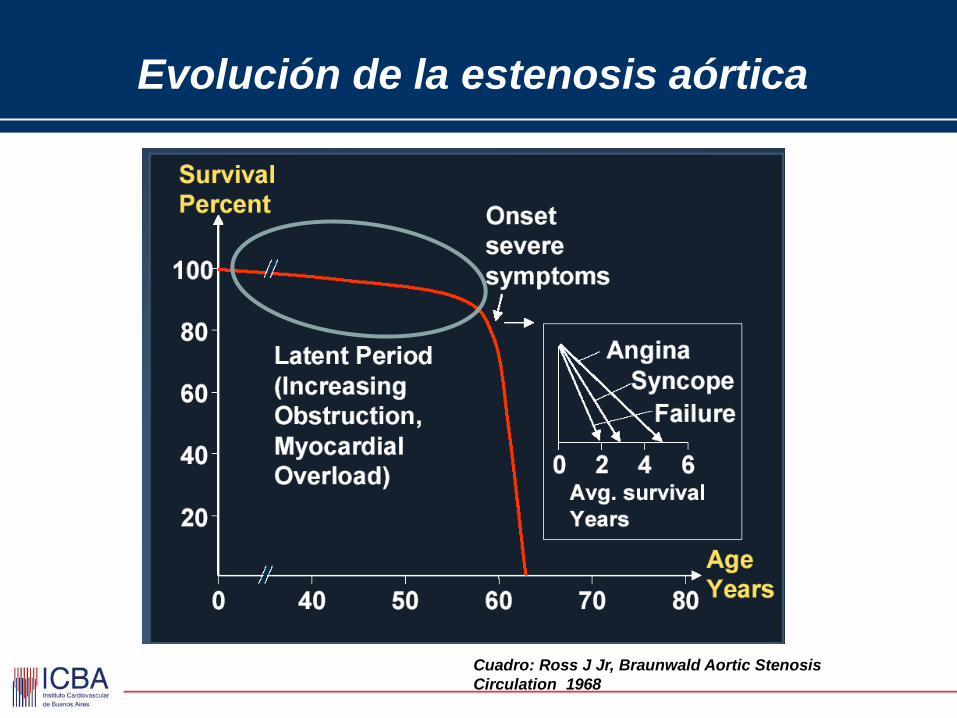
Evolución de la estenosis aórtica
Cuadro: Ross J Jr, Braunwald Aortic Stenosis
Circulation 1968
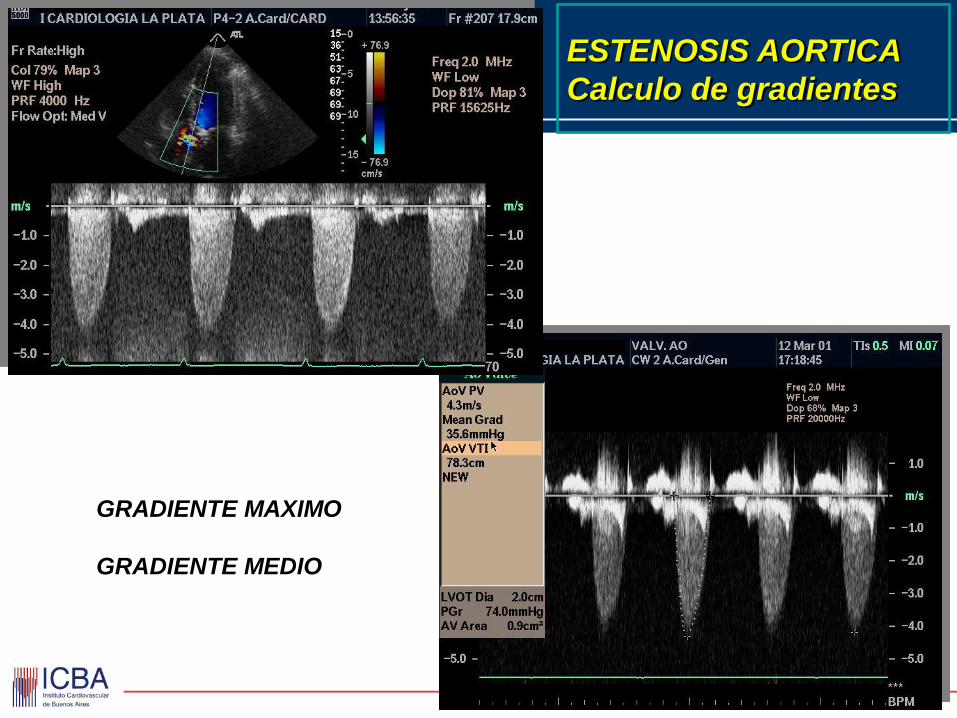
ESTENOSIS AORTICA
Calculo de gradientes
GRADIENTE MAXIMO
GRADIENTE MEDIO
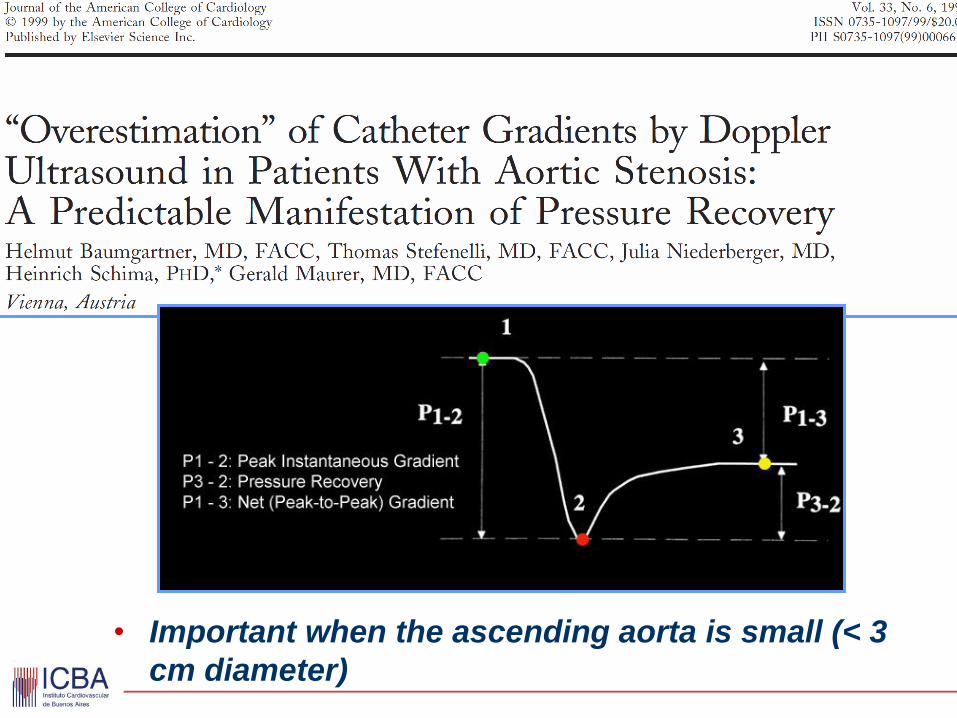
• Important when the ascending aorta is small (< 3
cm diameter)
www.manbit.com/ERS/images%5CPressureRecovery.jpg
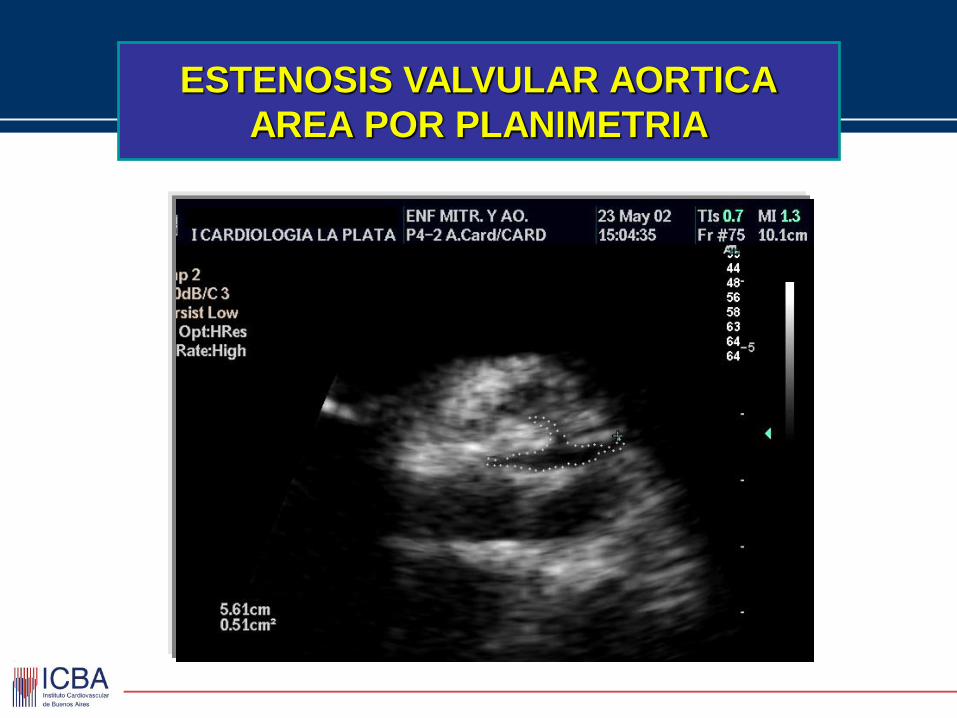
ESTENOSIS VALVULAR AORTICA
AREA POR PLANIMETRIA
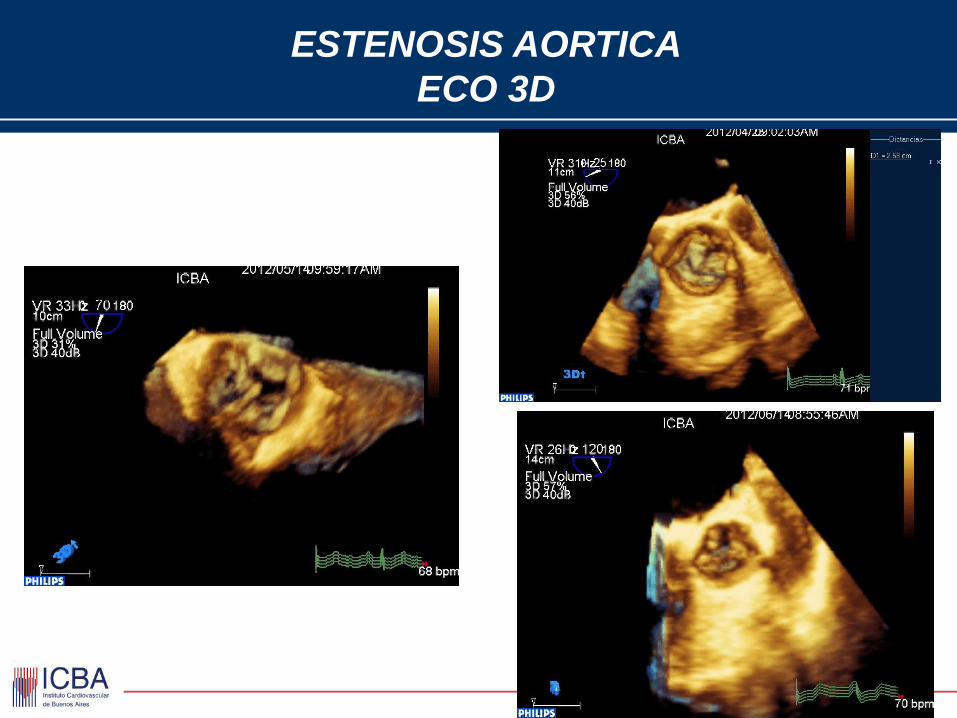
ESTENOSIS AORTICA
ECO 3D
Diástole Sístol
e
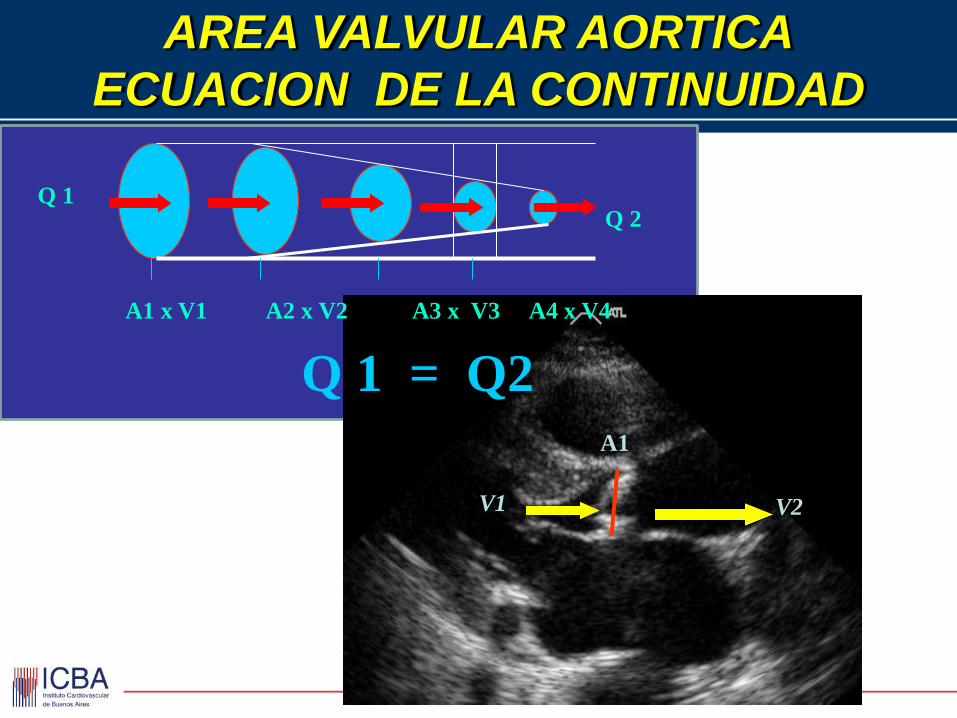
Q 1
AREA VALVULAR AORTICA
ECUACION DE LA CONTINUIDAD
Q 2
A1 x V1 A2 x V2 A3 x V3 A4 x V4
Q 1 = Q2
A1
V1 V2
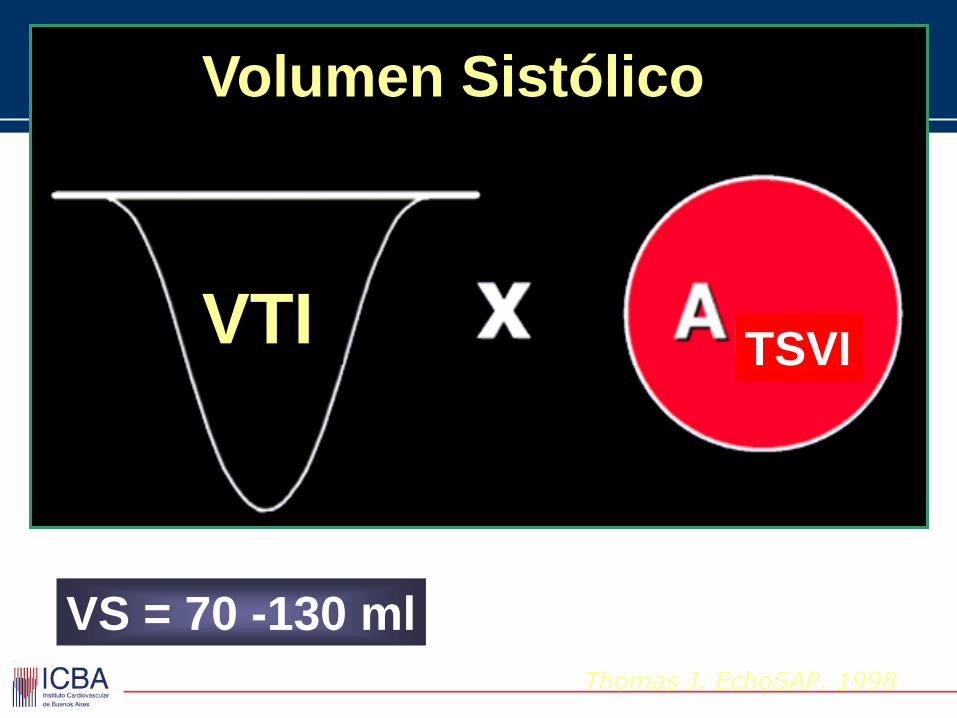
Thomas J. EchoSAP. 1998
Volumen Sistólico
VTI TSVI
VS = 70 -130 ml
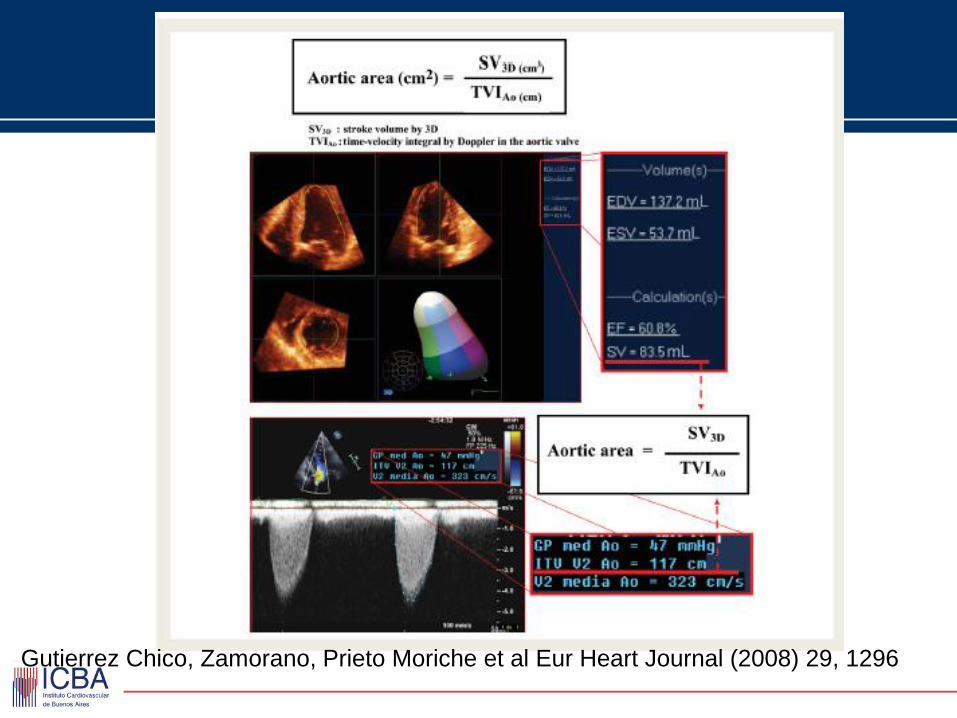
Gutierrez Chico, Zamorano, Prieto Moriche et al Eur Heart Journal (2008) 29, 1296
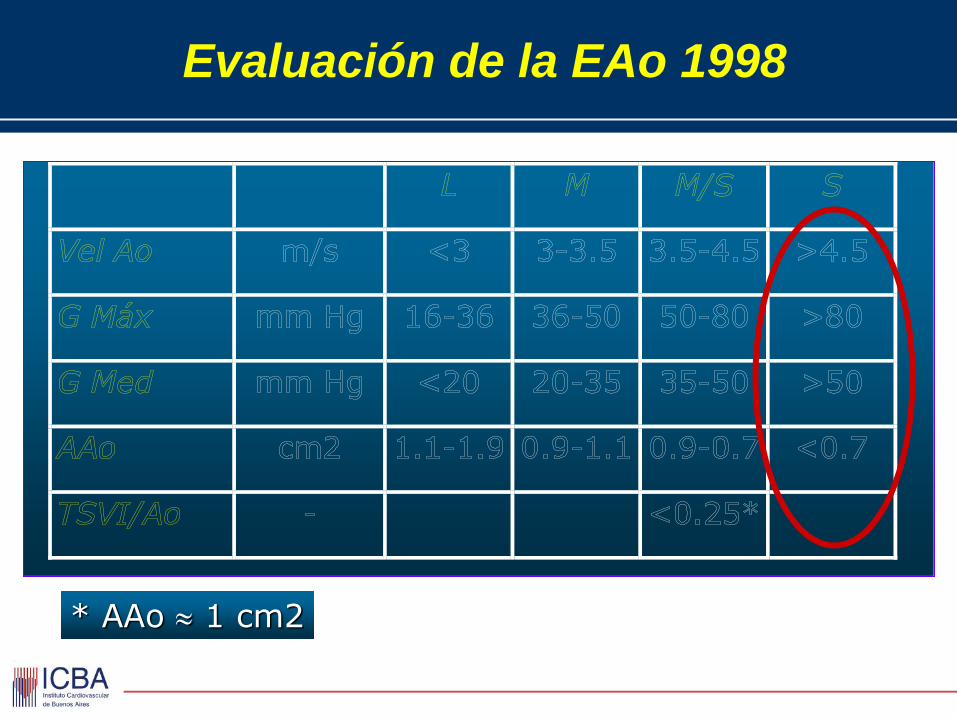
Evaluación de la EAo 1998
* AAo 1 cm2
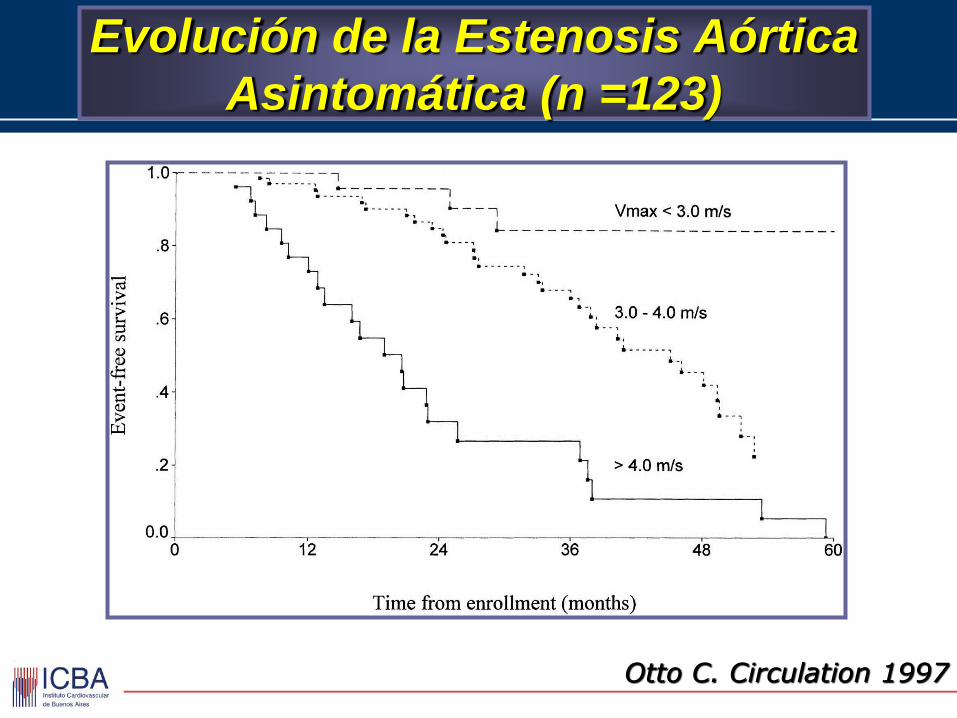
Otto C. Circulation 1997
Evolución de la Estenosis Aórtica
Asintomática (n =123)
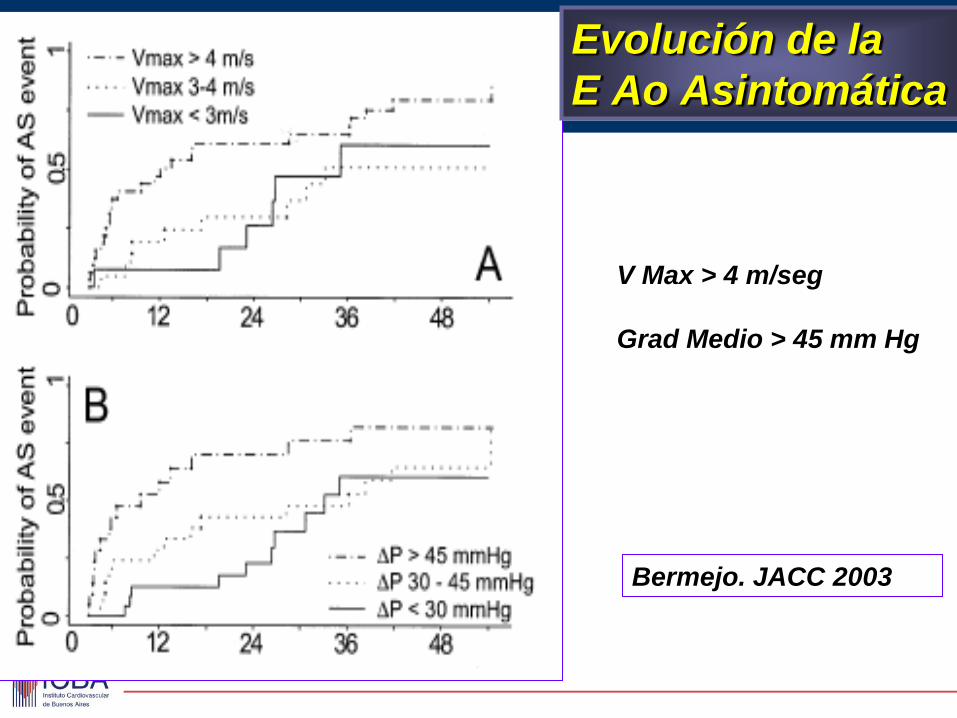
Bermejo. JACC 2003
Evolución de la
E Ao Asintomática
V Max > 4 m/seg
Grad Medio > 45 mm Hg
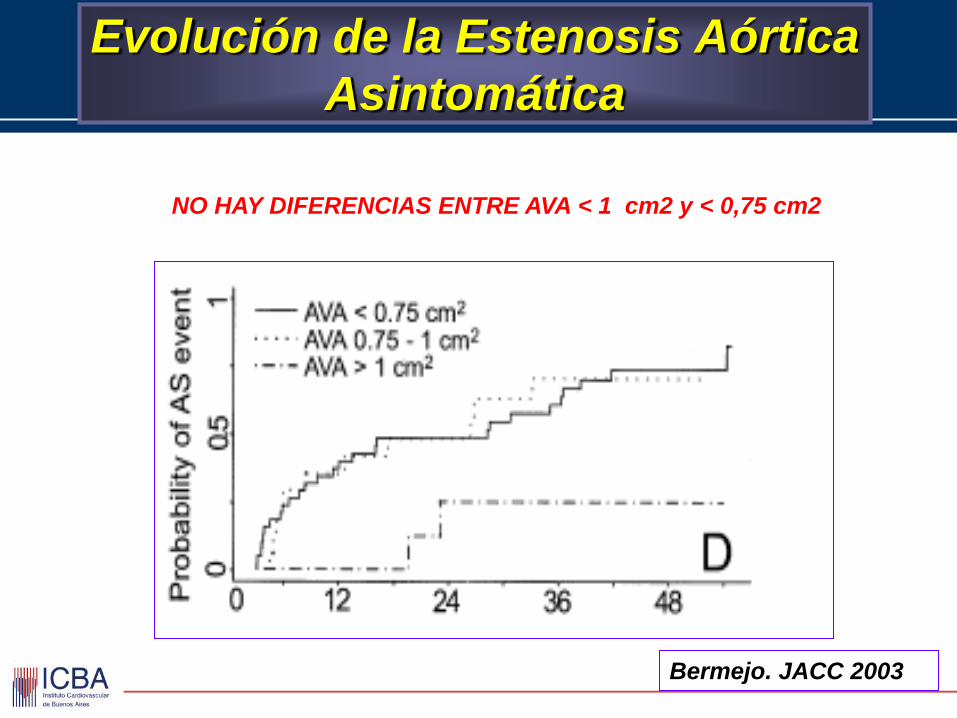
Bermejo. JACC 2003
Evolución de la Estenosis Aórtica
Asintomática
NO HAY DIFERENCIAS ENTRE AVA < 1 cm2 y < 0,75 cm2
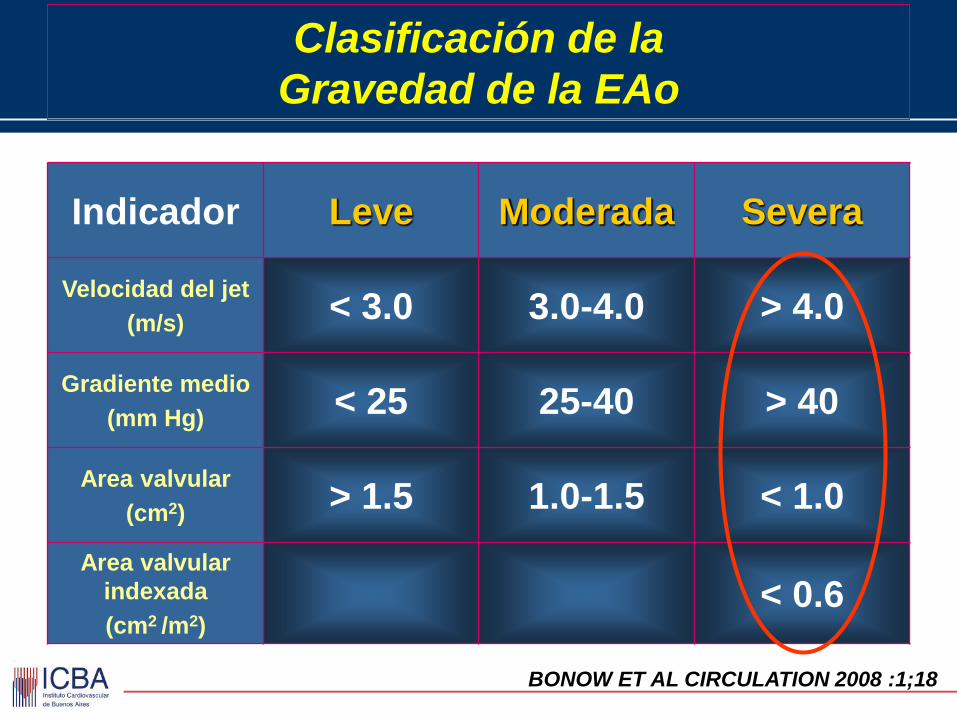
Clasificación de la
Gravedad de la EAo
Indicador Leve Moderada Severa
Velocidad del jet
(m/s) < 3.0 3.0-4.0 > 4.0
Gradiente medio
(mm Hg) < 25 25-40 > 40
Area valvular
(cm2) > 1.5 1.0-1.5 < 1.0
Area valvular
indexada
(cm2 /m2)
< 0.6
BONOW ET AL CIRCULATION 2008 :1;18
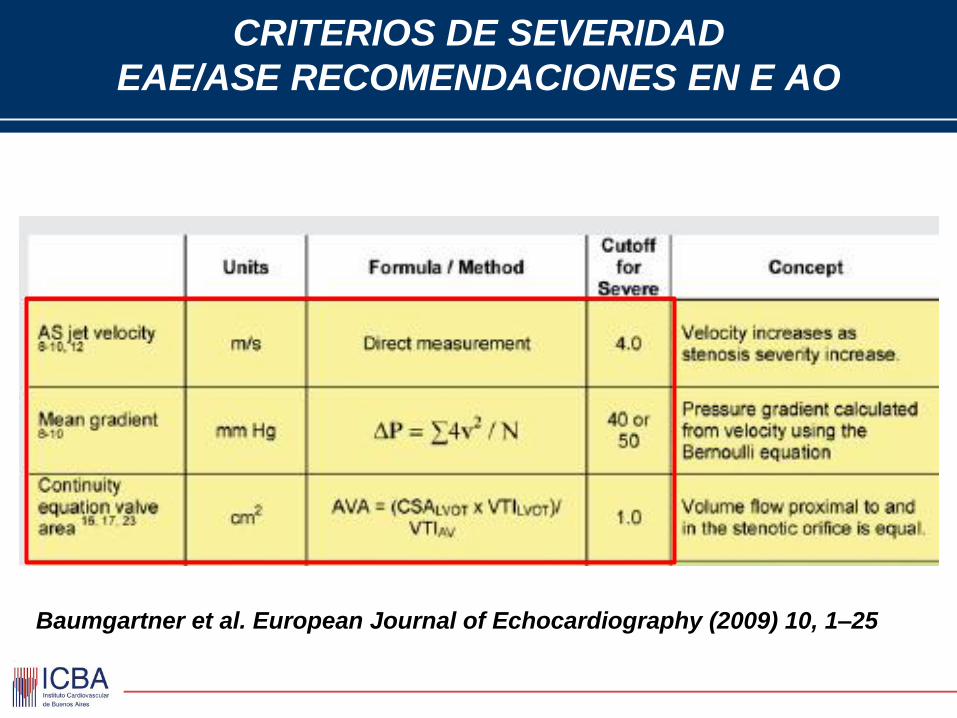
CRITERIOS DE SEVERIDAD
EAE/ASE RECOMENDACIONES EN E AO
Baumgartner et al. European Journal of Echocardiography (2009) 10, 1–25
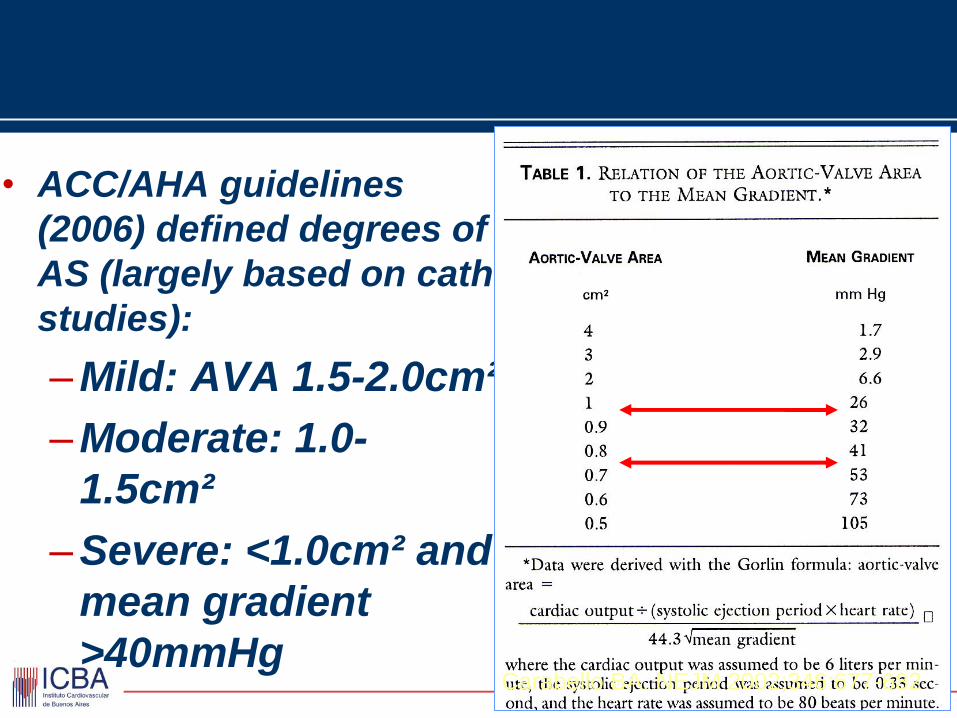
• ACC/AHA guidelines
(2006) defined degrees of
AS (largely based on cath
studies):
–Mild: AVA 1.5-2.0cm²
–Moderate: 1.0-
1.5cm²
–Severe: <1.0cm² and
mean gradient
>40mmHg
Carabello BA. NEJM 2002;346:677-682
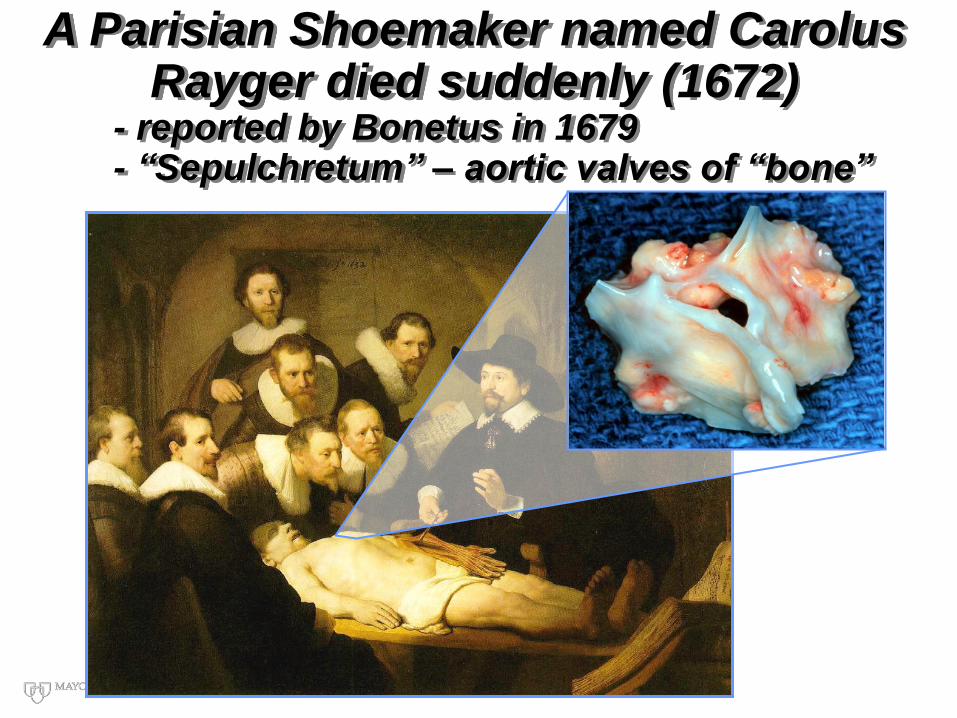
A Parisian Shoemaker named Carolus Rayger died suddenly (1672)
- reported by Bonetus in 1679 - “Sepulchretum” – aortic valves of “bone”
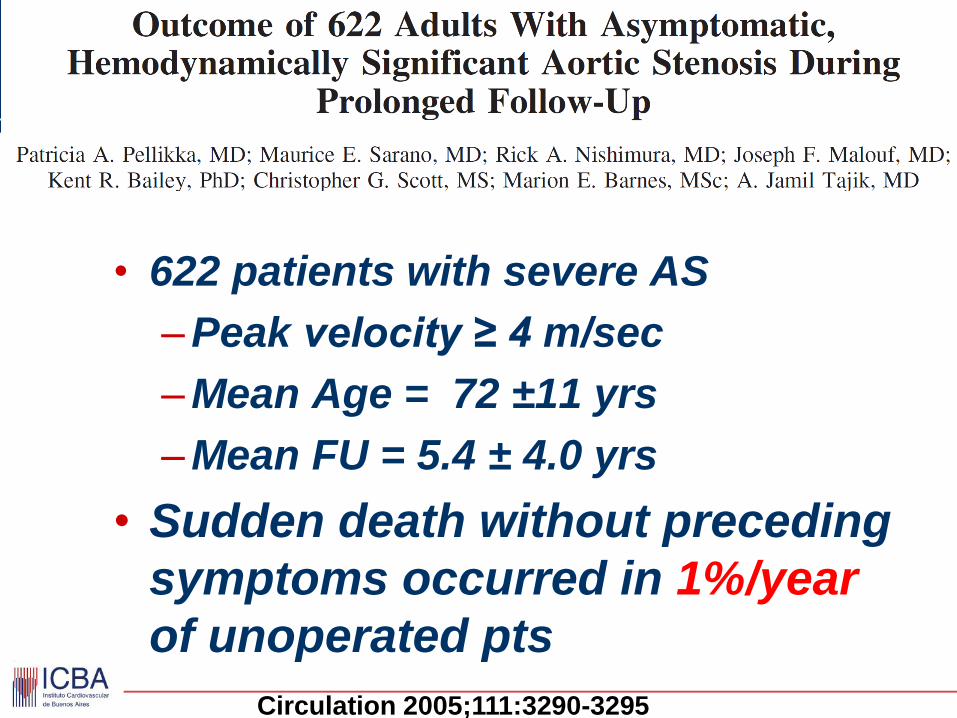
• 622 patients with severe AS
–Peak velocity ≥ 4 m/sec
–Mean Age = 72 ±11 yrs
–Mean FU = 5.4 ± 4.0 yrs
• Sudden death without preceding
symptoms occurred in 1%/year
of unoperated pts
Circulation 2005;111:3290-3295
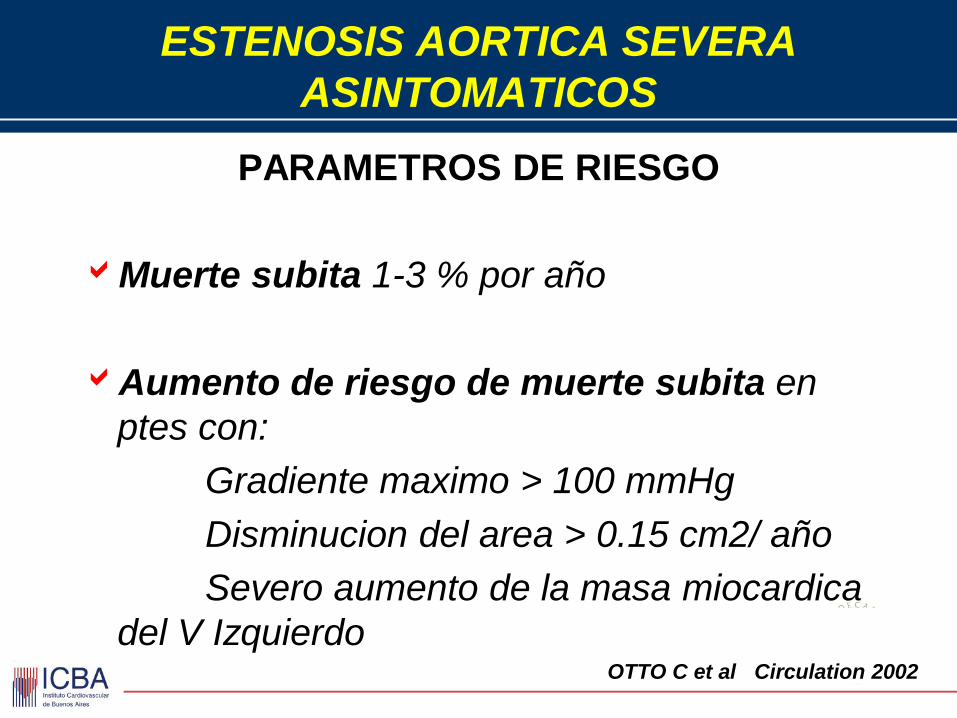
ESTENOSIS AORTICA SEVERA
ASINTOMATICOS
PARAMETROS DE RIESGO
Muerte subita 1-3 % por año
Aumento de riesgo de muerte subita en
ptes con:
Gradiente maximo > 100 mmHg
Disminucion del area > 0.15 cm2/ año
Severo aumento de la masa miocardica
del V Izquierdo
OTTO C et al Circulation 2002
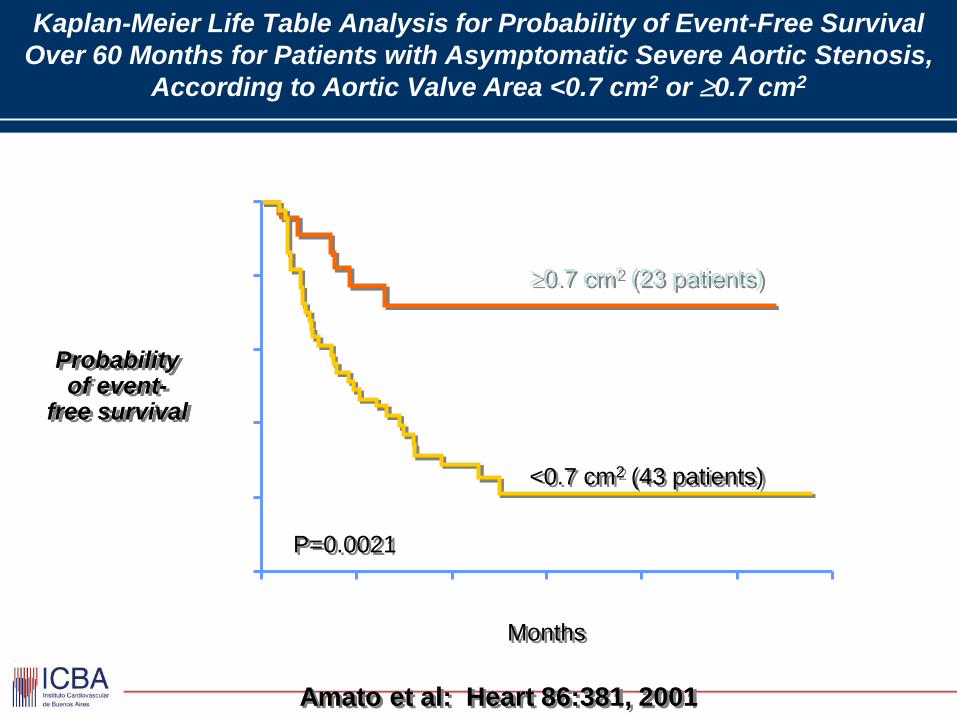
Kaplan-Meier Life Table Analysis for Probability of Event-Free Survival
Over 60 Months for Patients with Asymptomatic Severe Aortic Stenosis,
According to Aortic Valve Area <0.7 cm2 or 0.7 cm2
Probability of event-
free survival
Amato et al: Heart 86:381, 2001
Months
<0.7 cm2 (43 patients)
0.7 cm2 (23 patients)
P=0.0021 0.0
0.2
0.4
0.6
0.8
1.0
0 10 20 30 40 50 60
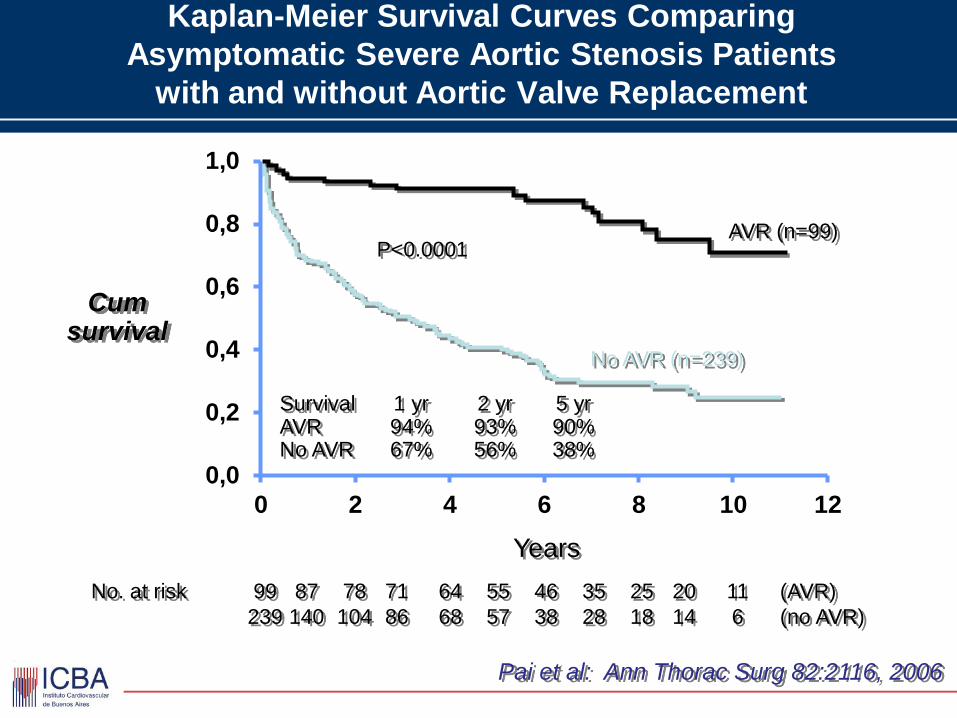
Kaplan-Meier Survival Curves Comparing
Asymptomatic Severe Aortic Stenosis Patients
with and without Aortic Valve Replacement
Cum survival
Pai et al: Ann Thorac Surg 82:2116, 2006
Years
No. at risk 99 87 78 71 64 55 46 35 25 20 11 (AVR)
239 140 104 86 68 57 38 28 18 14 6 (no AVR)
Survival 1 yr 2 yr 5 yr AVR 94% 93% 90% No AVR 67% 56% 38%
P<0.0001
No AVR (n=239)
AVR (n=99)
0,0
0,2
0,4
0,6
0,8
1,0
0 2 4 6 8 10 12
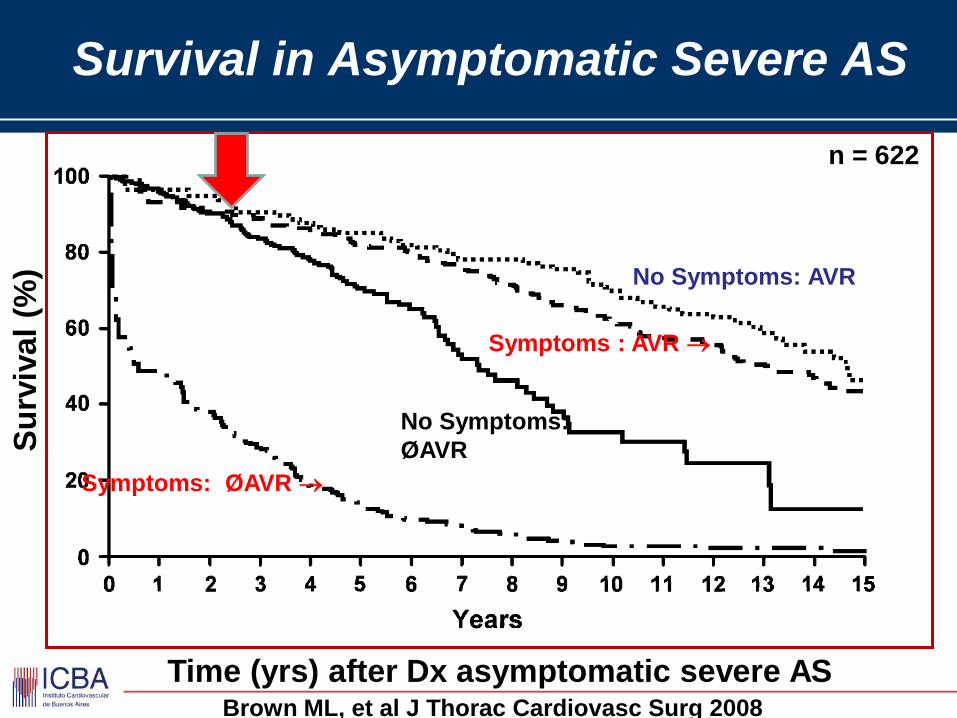
Survival in Asymptomatic Severe AS
Su
rviv
al
(%)
Time (yrs) after Dx asymptomatic severe AS Brown ML, et al J Thorac Cardiovasc Surg 2008
No Symptoms: AVR
Symptoms : AVR
No Symptoms:
ØAVR
Symptoms: ØAVR
n = 622
ESTENOSIS AORTICA
ASINTOMATICA
• Las E Ao severas tiene mayor mortalidad que
las de menor severidad Independientemente
de los sintomas
• La cirugia de RVAo se acompana de mejor
sobrevida que el tratamiento medico en E Ao
severa asintomatica
• La muerte subita esta presente en severas
1%/ ano
• DEBEMOS ENTONCES OPERAR A LOS
ASINTOMATICOS?
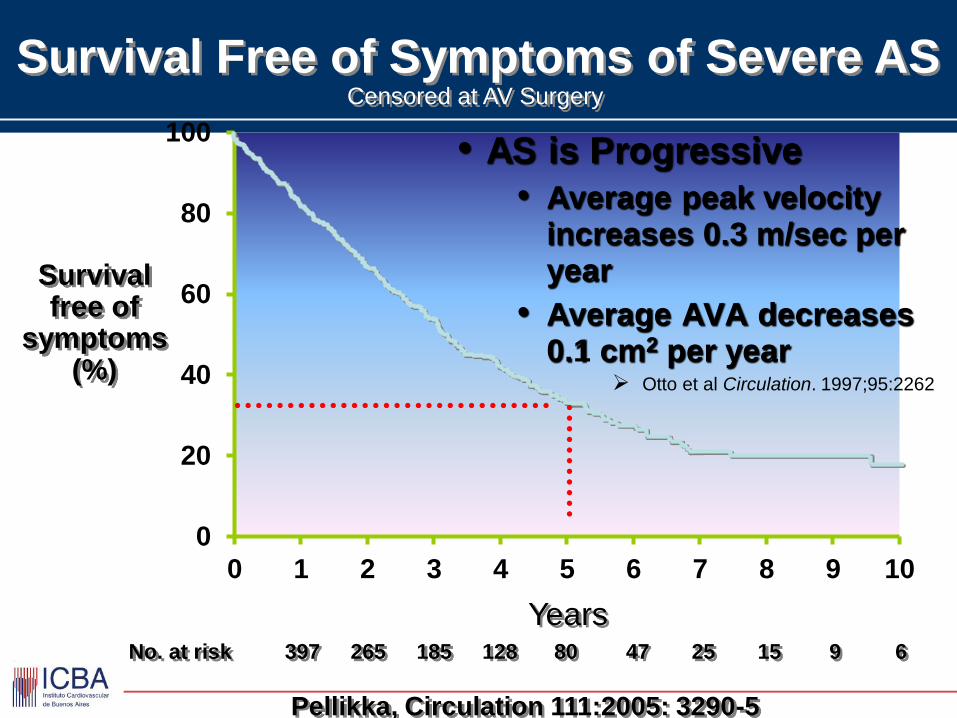
Years No. at risk 397 265 185 128 80 47 25 15 9 6
Survival free of
symptoms (%)
0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10
Survival Free of Symptoms of Severe AS Censored at AV Surgery
Pellikka, Circulation 111:2005: 3290-5
• AS is Progressive
• Average peak velocity increases 0.3 m/sec per year
• Average AVA decreases 0.1 cm2 per year
Otto et al Circulation. 1997;95:2262
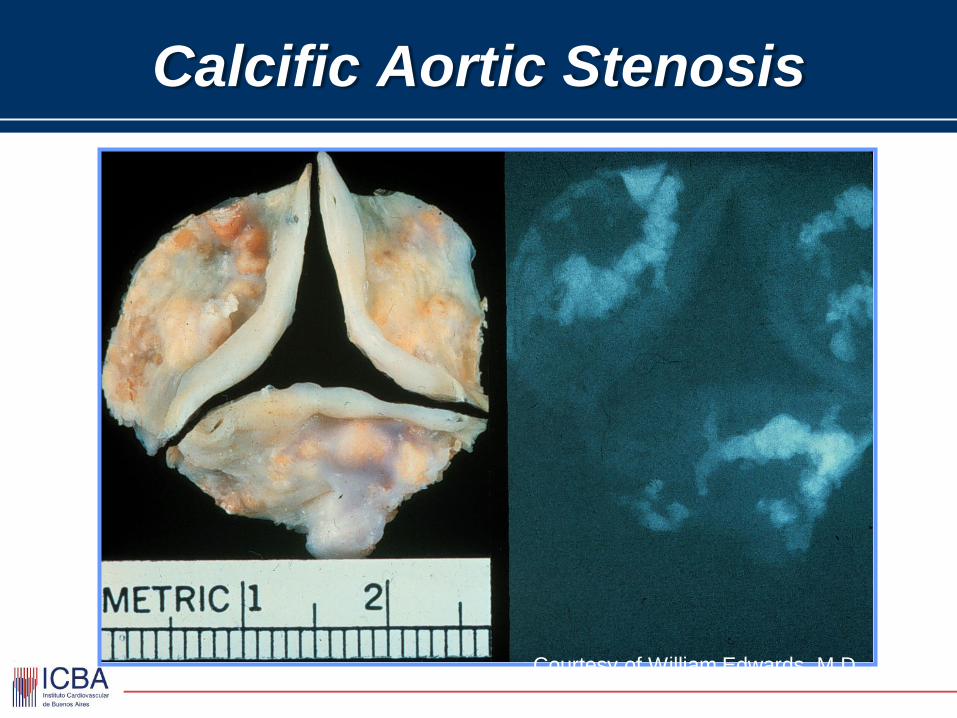
Calcific Aortic Stenosis
Courtesy of William Edwards, M D
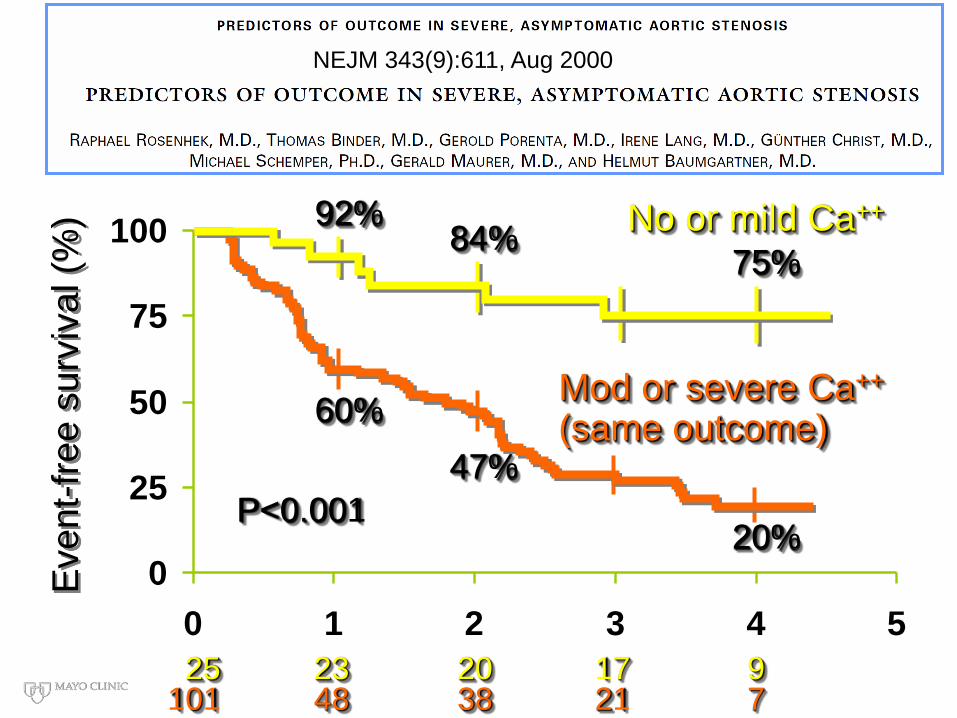
0
25
50
75
100
0 1 2 3 4 5
CP1065828-11
Event-
fre
e s
urv
ival (%
)
25 23 20 17 9 101 48 38 21 7
Mod or severe Ca++ (same outcome)
P<0.001
60%
47%
20%
No or mild Ca++ 92% 84%
75%
NEJM 343(9):611, Aug 2000
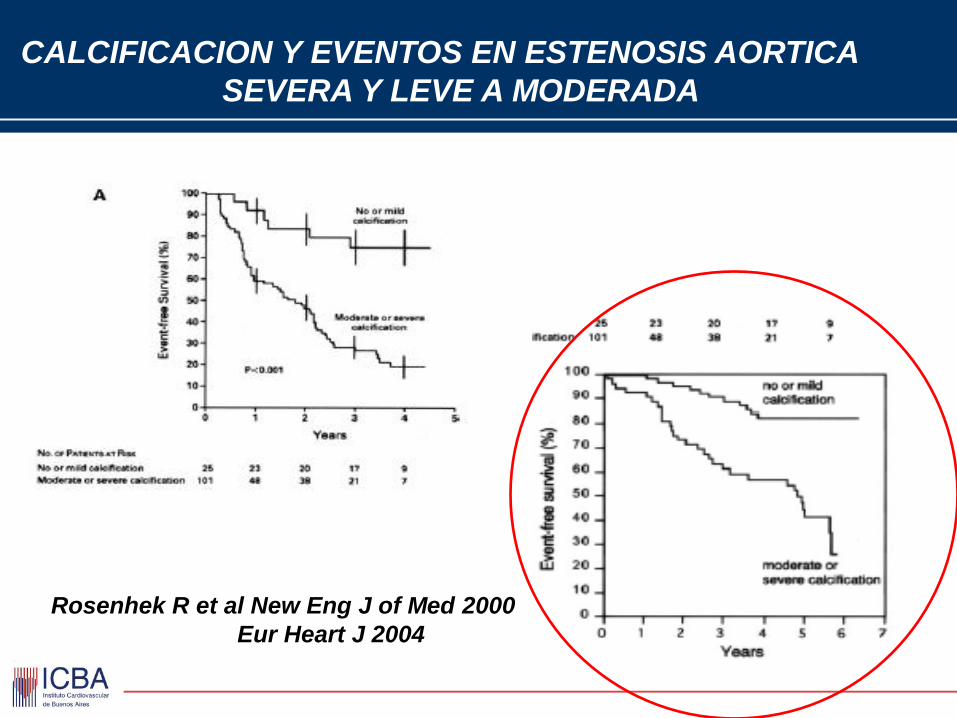
Rosenhek R et al New Eng J of Med 2000
Eur Heart J 2004
CALCIFICACION Y EVENTOS EN ESTENOSIS AORTICA
SEVERA Y LEVE A MODERADA
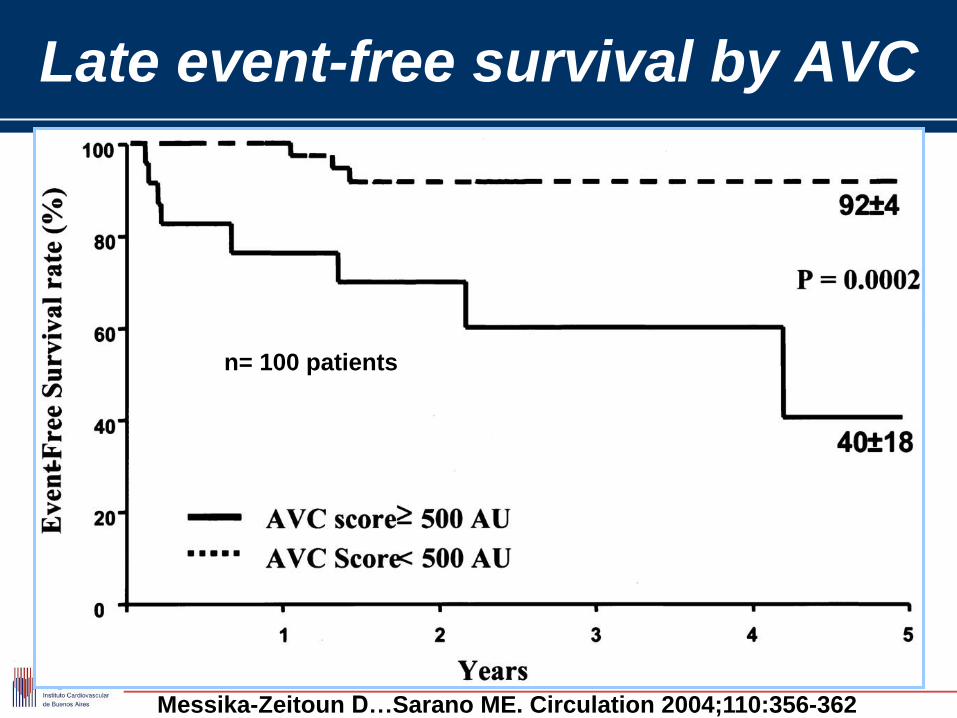
Messika-Zeitoun D…Sarano ME. Circulation 2004;110:356-362
Late event-free survival by AVC
n= 100 patients
ESTENOSIS AORTICA
CONTROVERSIAS
• Pacientes sintomáticos con estenosis
aórtica moderada de acuerdo a los
parámetros hemodinámicos
• Asintomáticos con baja capacidad
funcional ? Ejercicio!
BAUMGARTNER, OTTO : JACC: 2009: 54; 11; 1012
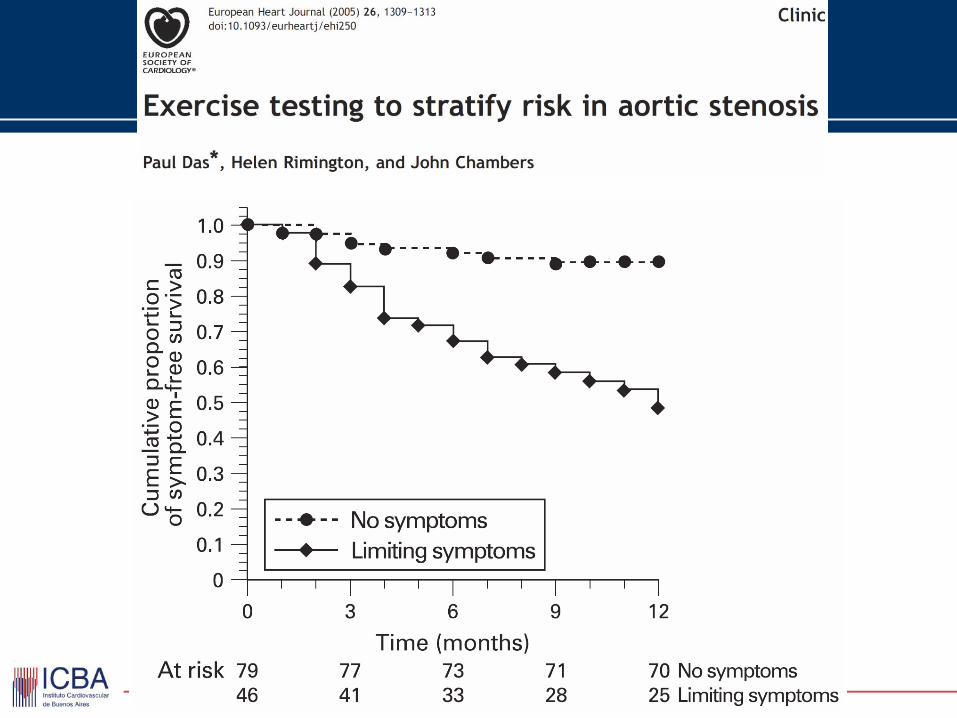
PRUEBA DE ESFUERZO
STRESS TEST
1. Stress testing in
asymptomatic severe aortic
stenosis
2. Dobutamine stress testing
in low gradient-low EF
aortic stenosis
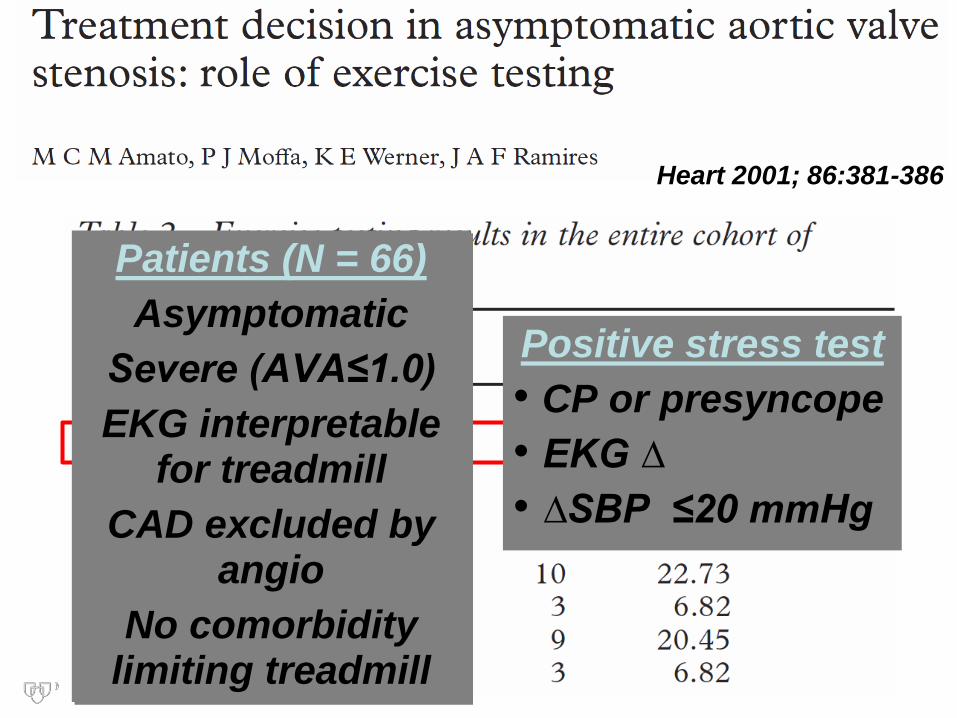
Heart 2001; 86:381-386
Patients (N = 66)
Asymptomatic
Severe (AVA≤1.0)
EKG interpretable for treadmill
CAD excluded by angio
No comorbidity limiting treadmill
Positive stress test
• CP or presyncope
• EKG ∆
• ∆SBP ≤20 mmHg
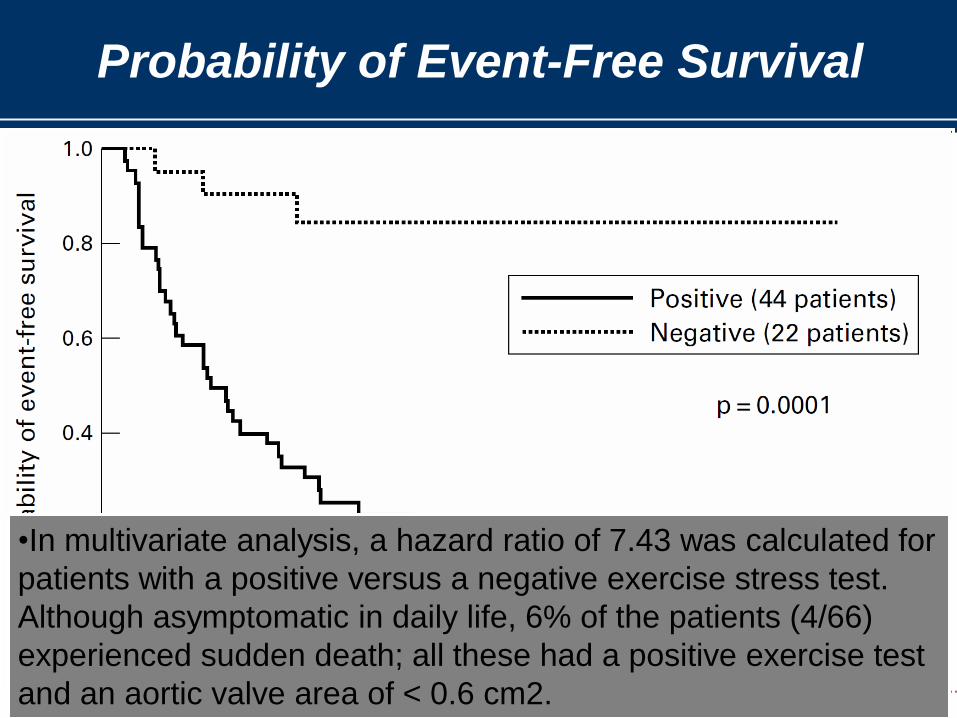
Probability of Event-Free Survival
•In multivariate analysis, a hazard ratio of 7.43 was calculated for
patients with a positive versus a negative exercise stress test.
Although asymptomatic in daily life, 6% of the patients (4/66)
experienced sudden death; all these had a positive exercise test
and an aortic valve area of < 0.6 cm2.
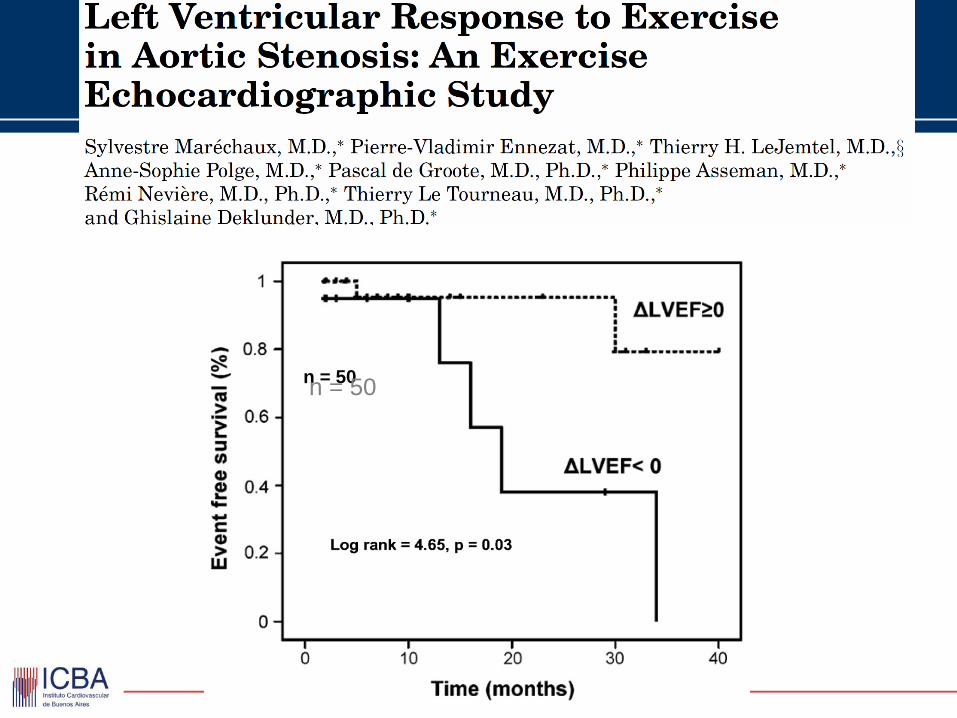
n = 50 n = 50
Circulation. 2005;112[suppl I]: I-377–I-382
Patients (n=69)
• Asymptomatic
• Severe (AVA ≤ 1 cm2)
• Normal LV EF
Positive Stress Test
• CP or dyspnea
• EKG ∆
• ∆SBP ≤20 mmHg
Lancellotti, P. et al. Circulation 2005;112:I-377-I-382
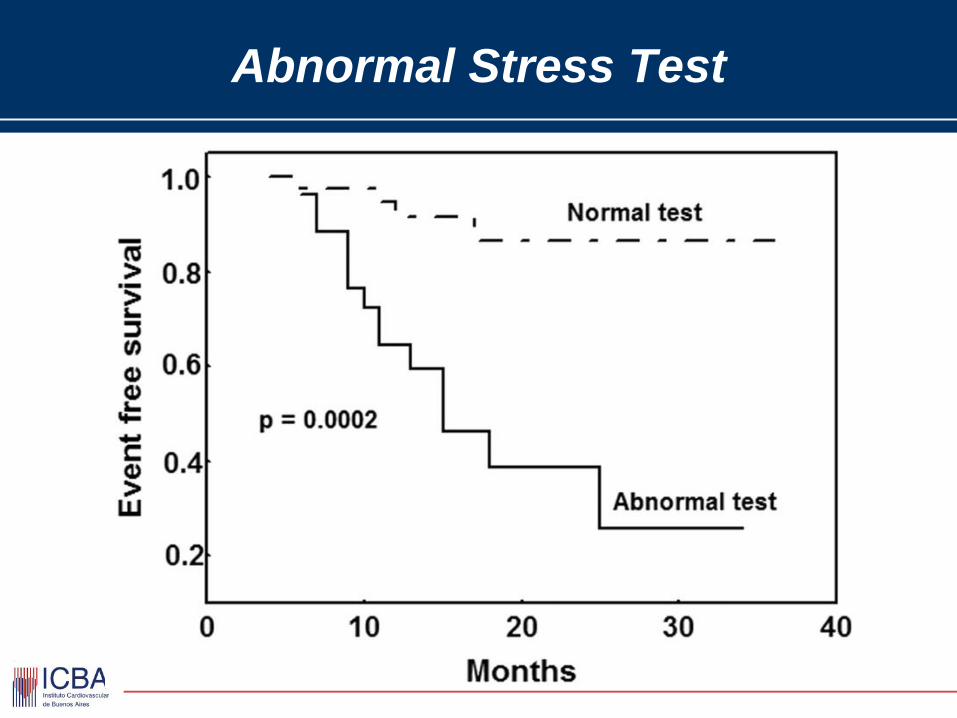
Abnormal Stress Test
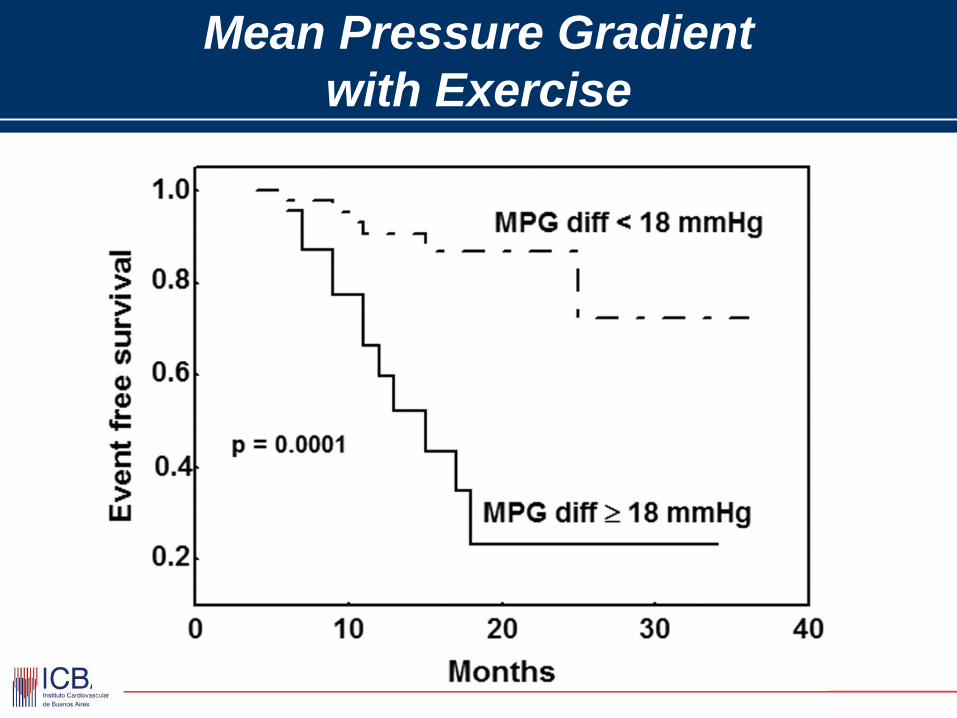
Mean Pressure Gradient
with Exercise
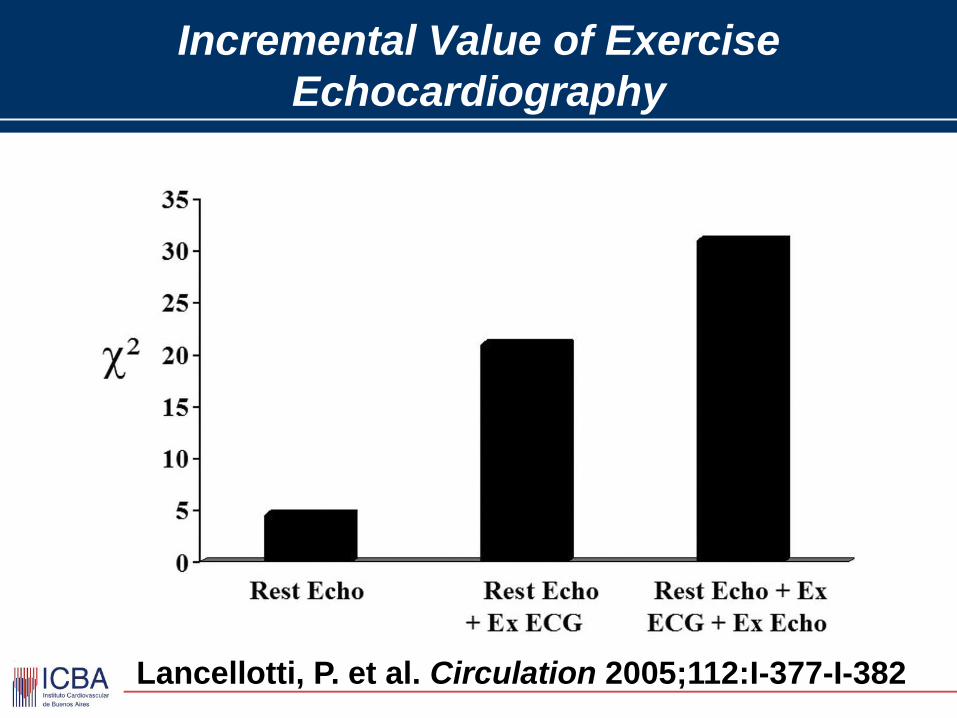
Incremental Value of Exercise
Echocardiography
Lancellotti, P. et al. Circulation 2005;112:I-377-I-382
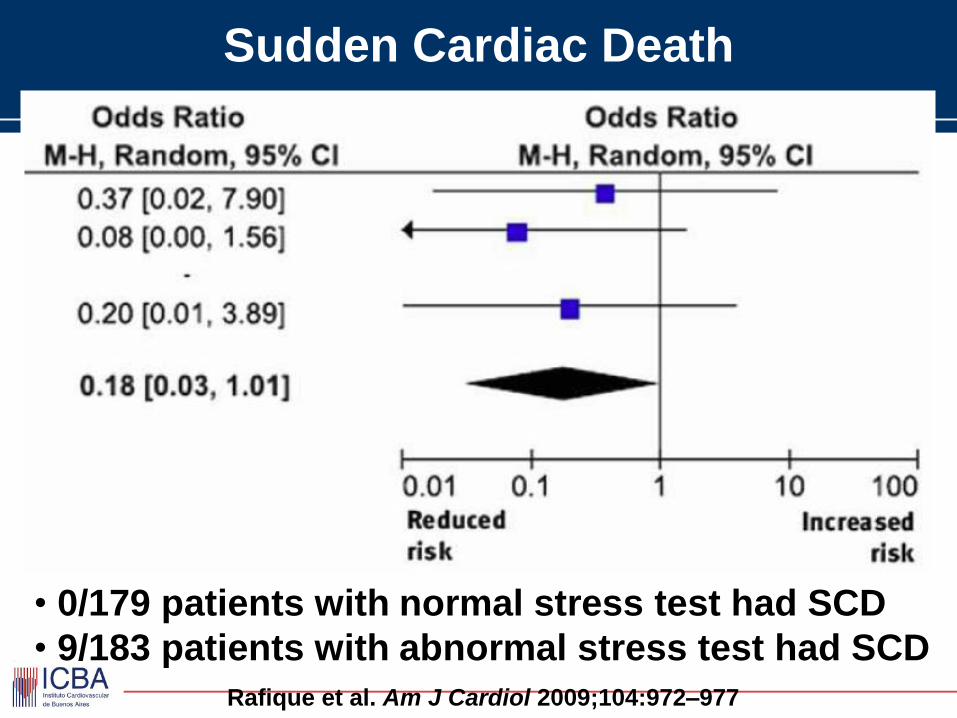
Sudden Cardiac Death
Rafique et al. Am J Cardiol 2009;104:972–977
• 0/179 patients with normal stress test had SCD
• 9/183 patients with abnormal stress test had SCD
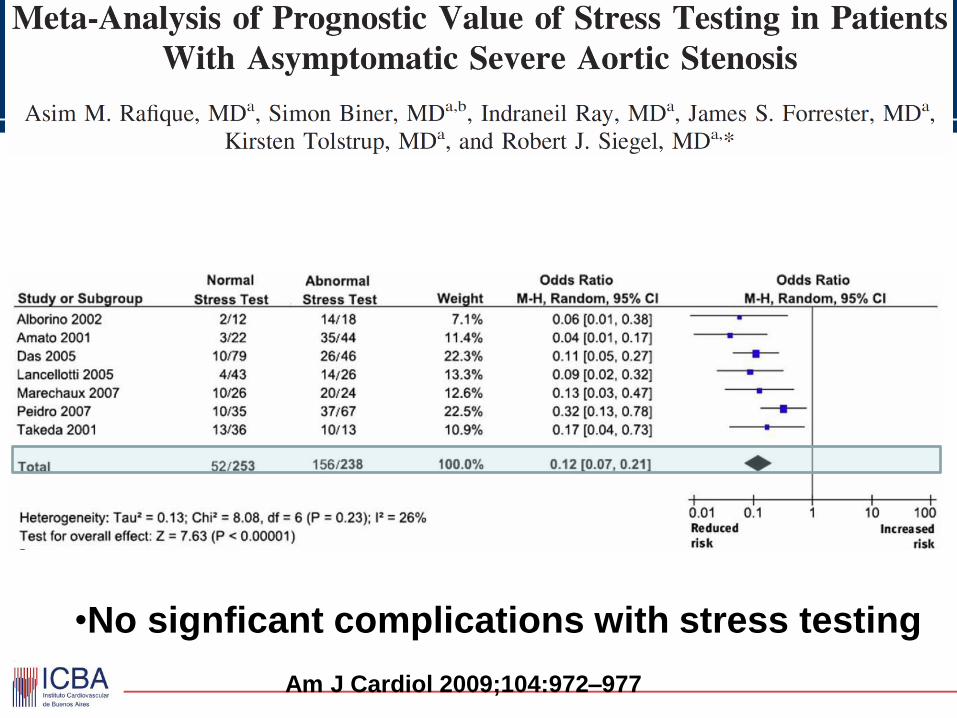
Am J Cardiol 2009;104:972–977
•No signficant complications with stress testing
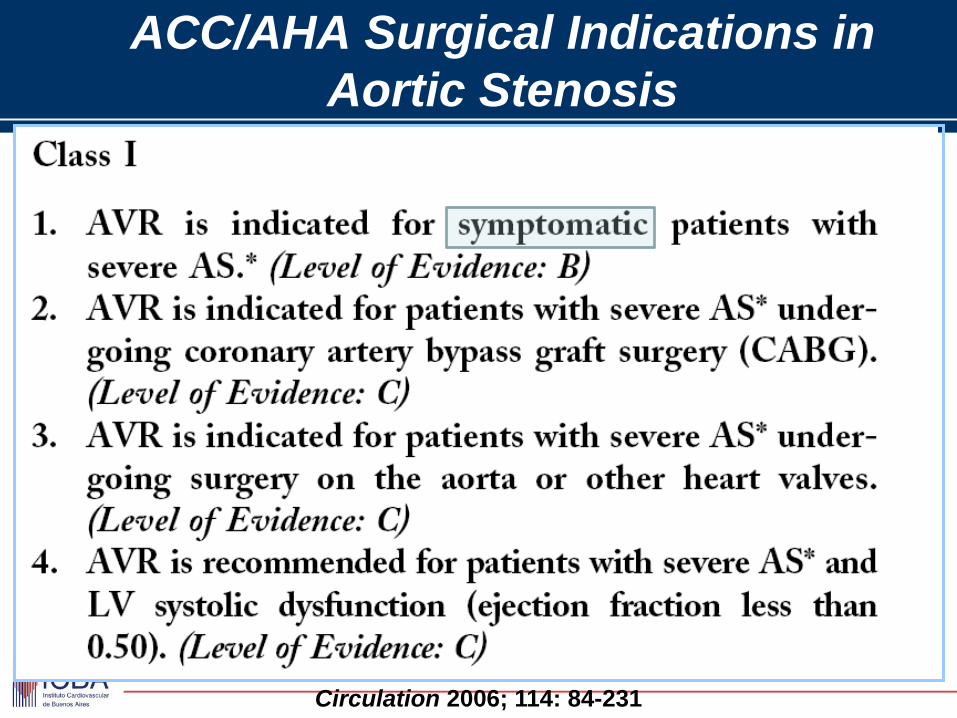
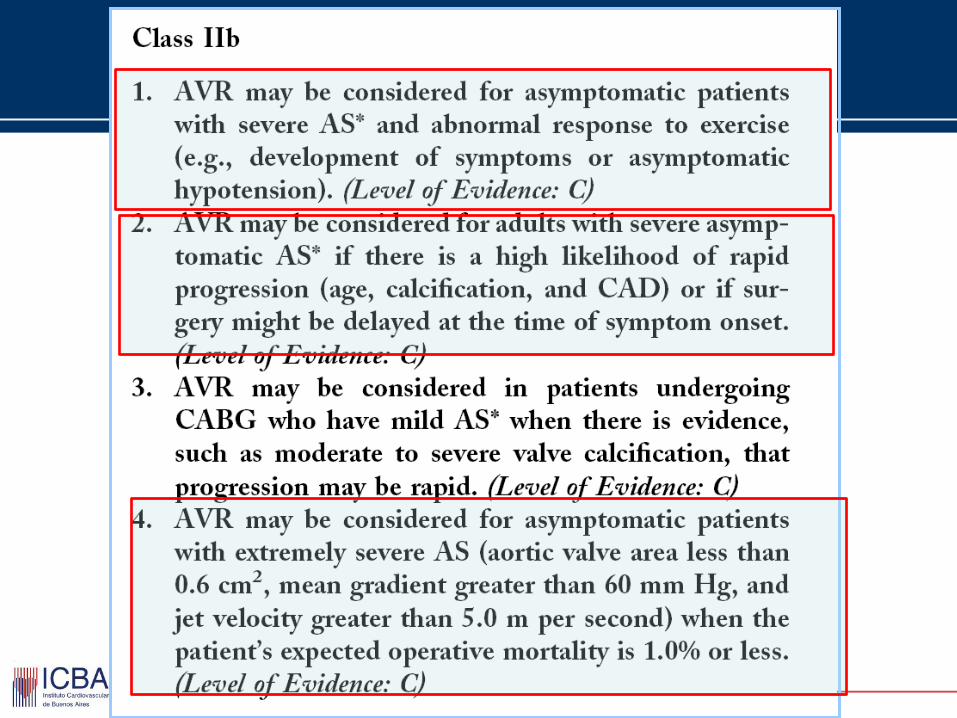
ACC/AHA Surgical Indications in
Aortic Stenosis
Circulation 2006; 114: 84-231
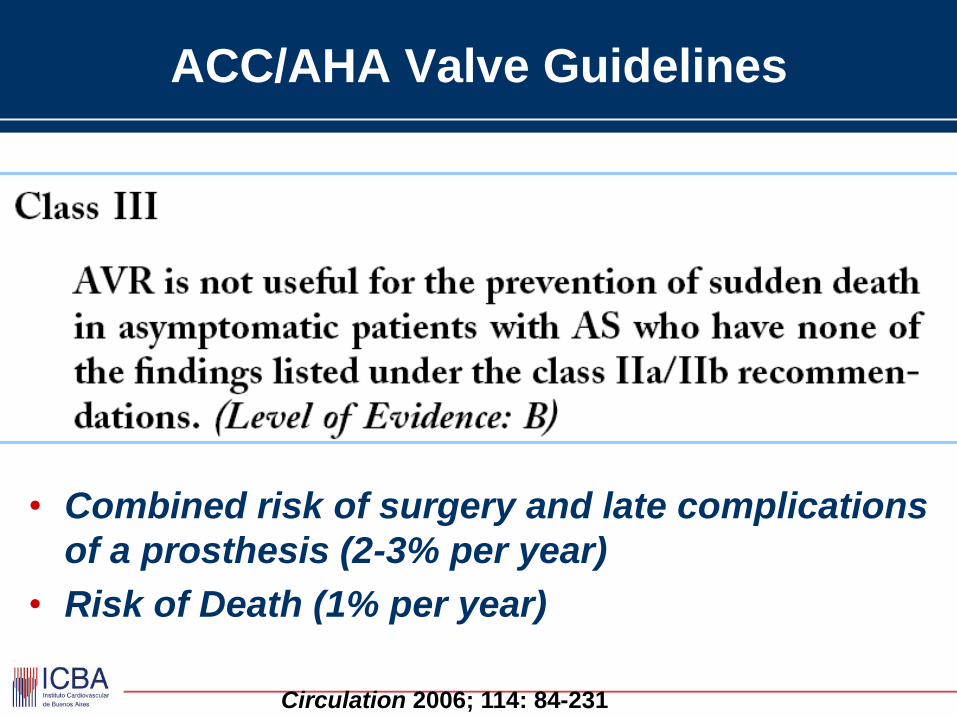
ACC/AHA Valve Guidelines
• Combined risk of surgery and late complications
of a prosthesis (2-3% per year)
• Risk of Death (1% per year)
Circulation 2006; 114: 84-231
REFLEXIONES
• La cuantificación de la severidad de la
estenosis aórtica presenta inconsistencias y
deberian revisarse las Guias ( < 0,7 cm2 ?)
• Las características anatómicas deben se
tenidas en cuenta al momento de interpretar
datos inconsistentes
• El cálculo de las variables utilizadas en la
cuantificación debe ser cuidadoso
metodológicamente
ESTENOSIS AORTICA
CONCLUSIONES
• El cálculo del área valvular es la medida mas confiable
para determinar la severidad de la estenosis aórtica
• Las diferentes técnicas de medición deben ser
aplicadas cuando existen dudas, pero la ecuación de
continuidad parece la más sólida
• La coincidencia con magnitud de los gradientes es
frecuente, pero su ausencia NO debe excluir el
diagnóstico. Altos gradientes en válvulas con escaso
deterioro, es posible en aortas pequeñas
ESTENOSIS AORTICA
CONCLUSIONES
• Las condiciones hemodinámicas y la función
ventricular deben ser consideradas aunque no se
calculen parámetros como impedancia vascular
• Los sintomáticos deben someterse a RVAO. La
ausencia de síntomas debe corroborarse con ejercicio,
observando tiempo libre de disnea y P Arterial
• La edad es un factor de riesgo para el RVAO, pero NO
CONTRAINDICACION !. Cirugía y Reemplazo
percutáneo alternativas posibles
ESTENOSIS AORTICA SEVERA
ASINTOMATICOS
PARAMETROS DE RIESGO
Menos de 6 minutos libres de disnea en
treadmill protocolo Naughthon
Caida de la Presion arterial sistolica > 15
mmHg durante esfuerzo en treadmill
Arritmias ventriculares inducidas por el
esfuerzo y/ o severa depresion del
segmento ST
INDICACIONES DE CIRUGIA
• EAO SINTOMATICA
• ESTENOSIS AORTICA CRITICA
• EAO ASINTOMATICA CON TEST FUNCIONAL
+ ( caida TA en max, angina y/o disnea en el
max esfuerzo)