Embed Size (px)
DESCRIPTION
ecg
Citation preview

ECG InterpretationECG Interpretation

DefinitionDefinition Test that records the electrical
activity of the heart Measure:
Rate and regularity of heartbeats Size and position of the chambers Presence of any damage to the heart Effects of drugs or devices used to
regulate the heart Systemic condition that gives effect
to the heart

How does it work?How does it work? The heart is a muscle with well-
coordinated electrical activity, so the electrical activity within the heart can be easily detected from outside of the body.
After the appropriate leads are attached to the body, a heated stylus moves upward with positive voltage and downward for negative voltage.
• On the moving heat-sensitive paper, voltage is traced out.

ECG leadECG lead Electrodes used to measure
electrical activity of the hearts 2 basic types
Bipolar leads (standard limb leads) utilize a single positive and a single negative electrode between which electrical potentials are measured.
Unipolar leads (augmented leads and chest leads) have a single positive recording electrode and utilize a combination of the other electrodes to serve as a composite negative electrode.

Limb lead (bipolar)Limb lead (bipolar)
I
II III
+/-
+
-

Extremity lead (unipolar)Extremity lead (unipolar)
Menggunakan terminal sentral sebagai titik nol

Precordial leadPrecordial lead

The Normal Conduction SystemThe Normal Conduction System

ECG TerminologyECG Terminology
P wave : the sequential activation (depolarization) of the right and left atria
PR interval: time interval from onset of atrial depolarization (P wave
QRS complex: right and left ventricular depolarization (normally the ventricles are activated simultaneously)
QRS duration: duration of ventricular muscle depolarization
PP interval: duration of atrial cycle (an indicator or atrial rate)
RR interval: duration of ventricular cardiac cycle (an indicator of ventricular rate
QT interval: duration of ventricular depolarization and repolarization

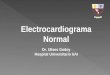
Normal ECGNormal ECG P wave
Width < 0.12 s Height < 0.3 milliVolt Always positive in lead II, negative in
aVR PR interval
From the start of P wave to the start of QRS
Normal duration 0.12 – 0.20 s QRS complex
Width 0.06 – 0.12 s (~ 0.10 s) Length varies among leads Q first negative deflection R first positive deflection S negative deflection after R
ST segment From the end of S to the start of T Normal : iso-electrical
T wave Positive in lead I, II, V3 – V6 and
negative in aVR

Normal ECGNormal ECG

Basic interpretationBasic interpretation
Rate Rhythm
Axis P wave morphology
PR interval QRS complex morphology ST segment morphology
T wave morphology U wave morphology
QTc interval

Determining the Heart RateDetermining the Heart Rate Rule of 300
300/[number of large boxes between two R waves]. only works for regular rhythms !!
300/7.5 large boxes = rate 40
Six second methods Count the number of R-R intervals in six seconds and multiply by 10 Useful for irregular rhythm average rate
There are 8 R-R intervals within 30 boxes. Multiply 8 x 10 = Rate 80

Determining the RhythmDetermining the Rhythm Source of depolarization
Sino-atrial (SA) node: sinus rhythm Depending on rate can be sinus bradicardi or sinus tachycardia
Non-sinus: atrial/ventricular rhythm (see arrhythmia section)
Sinus rhythm criteria P wave always followed by QRS complex

Normal ECGNormal ECG

AxisAxis
Defleksi positif Defleksi negatif

ECG abnormalitiesECG abnormalities
Hypertrophy Ischemia/infarct
Arrhythmia

HypertrophyHypertrophy
Right atrial enlargement Tall, peaked p wave
Left atrial enlargement Widening p wave, M-shape, notched Deep, negative component p wave in V1


Ventricular HypertrophyVentricular Hypertrophy
LVH (sokolow, Lyon) S di V1 + R di V5 atau V6 > 35 mm R di V5 atau V6 > 26 mm R + S di lead precordial > 45 mm
RVH R/S di V1 > 1 atau R/S di V6 < 1

R in V5 > 26 mm

R/S in V1 > 1 or R/S in V6 < 1

Infarct / IschemiaInfarct / Ischemia Evolution of MI
Hyperacute T wave changes - increased T wave amplitude and width; may also see ST elevation
Marked ST elevation with hyperacute T wave changes (transmural injury)
Pathologic Q waves, less ST elevation, terminal T wave inversion (necrosis)
Pathologic Q waves, T wave inversion (necrosis and fibrosis)
Pathologic Q waves, upright T waves (fibrosis)


•I, aVL, V5•V2-V4


Arrhythmia Arrhythmia
ClassificationSupraventrivular arrythmia
Sinus pause or arrest, SA block, PAC, atrial flutter, atrial fibrillation, etc
Ventricular arrythmia PVC, VT, torsade de pointes, VF, etc
AV conduction abnormalities AV block, WPW syndrome, etc

RhythmRhythm
Rhythm Guidelines: Check the bottom rhythm strip for regularity, i.e. - regular,
regularly irregular, and irregularly irregular. Check for a P wave before each QRS, QRS after each P. Check PR interval (for AV blocks) and QRS (for bundle
branch blocks). Check for prolonged QT. Recognize "patterns" such as atrial fibrillation, PVC's,
PAC's, escape beats, ventricular tachycardia, paroxysmal atrial tachycardia, AV blocks and bundle branch blocks

BlocksBlocks SA node block
Failure of the SA node to transmit an impulse Complete pause of 1 beat ("skipped beat")
AV node block Block which delays the electrical impulse as it
travels between the atria and the ventricles in the AV node
Presented by PR interval

Blocks…Blocks… 1st degree AV block
PR interval greater than 0.2 seconds (200ms or 1 large box)
2nd degree AV block Type I (Wenckebach) PR interval gets longer (by shorter
increments) until a nonconducted P wave occurs Type II (Mobitz) PR intervals are constant until a
nonconducted P wave occurs

Blocks…Blocks…
3rd degree AV block Complete block of signals from the atria to the
ventricles complete dissociation between the timing of the P-waves and the QRS complexes

Bundle branch blocksBlocks within the ventricular bundlesWide QRS complexConsist of
Right ventricular bundle branch block Left ventricular bundle branch block Left anterior fasicular block Left posterior fasicular block
Blocks…Blocks…

RBBBRBBB Complete
QRS duration > 0.12 s rSR’ in lead V1-V2 Slurred S wave in lead I, aVL,
V5-V6 Down sloping of ST segment
and T wave inversion in lead V1-V2
Incomplete rSR’ complex in lead V1 QRS duration of 0.12 s or less R or S waves are not broad or
slurred Normal QRS axis

LBBBLBBB Complete
QRS duration > 0.12 s Bizarre, wide rS or QS complex in lead V1 Wide R wave in lead V6, sometimes plateu or M-
shaped Discordant T wave Absence of normal septal Q wave in lead I, aVL, V6

LAFBLAFB Criteria
QRS duration < 0.12 Left axis deviation more than -45 degrees qR wave in leads I, aVL Small rS complex in leads II, III, aVF

LPFBLPFB
CriteriaQRS duration < 0.12 sRight axis deviation > +110 degreesSmall r wave and large S wave in leads I, aVLSmall q waves in inferior leadsNo other explanation for RAD (ex. RVH,
COPD, lateral myocardial infarction)

Supraventricular ArrythmiaSupraventricular Arrythmia Premature atrial contraction
Single or repetitive, unifocal or multifocal
Atrial fibrillation Atrial activity is poorly defined; may see course or fine
undulations or no atrial activity at all Ventricular response is irregularly irregular

Supraventricular…Supraventricular… Atrial flutter
Regular atrial activity with a "clean" saw-tooth appearance The ventricular response may be 2:1, 3:1 (rare), 4:1, or
irregular
Paroxysmal supraventricular tachycardia Arise from structure above his bundle Reciprocating tachycardias because they utilize the mechanism of reentry

Ventricular ArrythmiaVentricular Arrythmia Premature ventricular contraction
May be unifocal, multifocal or multiformed Occur as isolated single events or as couplets, triplets, and salvos (4-
6 PVCs in a row ~ brief VT) R-on-T PVCs vulnerable to ventricular tachycardia or fibrillation
Ventricular tachycardia Sustained (lasting >30 sec) vs. nonsustained Monomorphic (uniform morphology) vs. polymorphic vs. Torsade-de-
pointes

Ventricular…Ventricular…
Ventricular fibrillation Chaotic, wide, ventricular tachyarrythmia with
grossly irregular morphology No consistent identifiable QRS complexes