Upload
fciencias
View
225
Download
0
Embed Size (px)
Citation preview
8/13/2019 HDLdiabetes.pdf
1/19
8/13/2019 HDLdiabetes.pdf
2/19
1052
S. E. Borggreve et al.
2003 Blackwell Publishing Ltd, European Journal of Clinical Investigation
, 33
, 10511069
cholesterol and subsequent hepatobiliary transport is altered in insulin resistance and type2 diabetes mellitus is unknown.
Specic CETP inhibitors have been developed that exert major HDL cholesterol-raisingeffects in humans and retard atherosclerosis in animals. As an increased CETP-mediatedcholesteryl ester transfer represents a plausible metabolic intermediate between hightriglycerides and low HDL cholesterol, studies are warranted to evaluate the effects of these
agents in insulin resistance- and diabetes-associated dyslipidaemia.
Keywords
Cholesteryl ester transfer protein, high-density lipoproteins, insulin resistance,lecithin:cholesterol acyltransferase, lipases, phospholipid transfer protein, reverse cholesteroltransport, type 2 diabetes mellitus.
Eur J Clin Invest 2003; 33 (12): 10511069
Introduction
Dyslipidaemia represents one of the most important riskfactors for cardiovascular morbidity and mortality [1]. Aninverse relationship between plasma high-density lipopro-tein (HDL) cholesterol and atherosclerosis was alreadydescribed in the 1950s [2], but the importance of this rela-tionship was only realized in 1975 [3]. Many subsequentstudies have emphasized that low HDL cholesterol is asso-ciated with an increased cardiovascular risk [4]. Currentopinion is that next to high LDL cholesterol and low HDL cholesterol levels, high plasma triglycerides should beregarded as a risk factor for the development of cardiovas-cular disease [5].
Insulin sensitivity can be dened as a measure of thecapacity of insulin to exert its biological effects on insulin-
sensitive tissues. Insulin resistance that relates to whole-body glucose metabolism refers to the ability of insulin tolower blood glucose, consequent to either decreased cellularglucose uptake or increased hepatic glucose output. Insulinresistance is a harbinger of type 2 diabetes mellitus and ispathogenetically linked to an increased risk of cardiovascu-lar events [6]. The insulin resistance syndrome originallyincluded hyperinsulinaemia, impaired glucose tolerance,hypertension, increased plasma triglycerides and decreasedHDL cholesterol [7]. Later, other features were added suchas visceral adiposity, small dense LDL, exaggerated post-prandial lipaemia, increased plasma plasminogen activatorinhibitor-1 and decreased sex hormone binding globulinlevels [8]. Hypertension [9] and impaired brinolysis [10]possibly contribute to increased cardiovascular risk. Aboveall, a major cause of coronary heart disease associated withinsulin resistance is dyslipidaemia, hallmarked by lowHDL cholesterol and high plasma triglycerides [6,11].Importantly, low HDL cholesterol remains an independentcardiovascular risk factor once type 2 diabetes mellitus hasdeveloped [12].
The cardioprotective role of HDL is thought to be relatedat least in part to the role of HDL in reverse cholesteroltransport (RCT), the process by which cholesterol isremoved from peripheral cells and transported to the liverfor metabolism and excretion in the bile [13,14]. In addition,
HDL has important antioxidative and anti-inammatoryproperties [15,16] and may prevent adhesion of monocytesto the endothelial cells [17].
This review focuses on the causes of low HDL choles-terol, and on alterations in HDL metabolism and RCT ininsulin resistance and type 2 diabetes mellitus. Further-more, recently developed therapeutic strategies to raise HDL cholesterol are discussed.
High-density lipoprotein metabolism undernormolipidaemic circumstances
High-density lipoproteins comprise a heterogeneous classof lipoproteins with a density > 1063 g mL
1
[18,19]. High-
density lipoprotein particles contain various apolipoproteins(apos) of which apo A-I and apo A-II are qualitatively themost abundant [20]. In humans, liver and intestine areimportant sources of apo A-I, whereas apo A-II is predom-inantly produced by the liver [1820]. Some HDLs alsocontain apo E. High-density lipoproteins can be subdividedaccording to the density in HDL
2
, the less dense subfractionand HDL
3
[18]. Both HDL
2
and HDL
3
contain apo A-I,and migrate with
-mobility on electrophoresis [19]. TheseHDL subfractions can also be differentiated according totheir apolipoprotein composition in HDL particles that onlycontain apo A-I (LpA-I) and particles that contain apo A-I as well as apo A-II (LpA-I/A-II) [19,20]. A small fractionof HDL particles are lipid poor and very small sized [13].Most of these particles show pre
-mobility on electrophore-sis and are designated as pre
-HDL, which can be furthersubdivided into pre
1
- pre
2
- and pre
3
-HDL [13,19].These discoidal, nascent HDL particles contain apo A-I, aswell as some phospholipids [13,18,19].
High-density lipoprotein formation is regarded to beginwith pre
-HDL that are produced by liver and intestine aswell as extracellularly during the metabolism of triglyceride-rich lipoproteins and HDL remodelling [13,18,19,21].As these particles mature they become spherical with
-electrophoretic mobility with HDL
2
originating from HDL
3
[13,19,21]. High-density lipoprotein particles are constantly
8/13/2019 HDLdiabetes.pdf
3/19
HDL metabolism and reverse cholesterol transport in insulin resistance and type 2 diabetes mellitus
1053
2003 Blackwell Publishing Ltd, European Journal of Clinical Investigation
,33
, 10511069
remodelled as a result of many interrelated processes.As described later, several enzymes including lipoproteinlipase, hepatic lipase, the recently discovered endotheliallipase and lecithin:cholesterol acyltransferase, as well aslipoprotein transfer proteins including cholesteryl estertransfer protein and phospholipid transfer protein are
involved in HDL metabolism.
Lipoprotein lipase
Lipoprotein lipase (LPL) is predominantly present in adi-pose tissue, skeletal muscle and heart [22]. After synthesisby parenchymal cells, LPL is transferred to endothelial cellsand bound to heparan sulphate proteoglycans [22]. Lipo-protein lipase hydrolyses triglycerides contained withinlipoproteins. During the process of chylomicron and verylow-density lipoprotein (VLDL) triglyceride hydrolysis,surface fragments are transferred to maturing HDLs [18].Adipose tissue LPL mRNA expression as well as its activityare positively correlated with postprandial plasma triglycerideexcursions [23].
Genetic lipoprotein lipase deciency associates with severehypertriglyceridaemia and with very low HDL cholesterollevels [24], whereas the LPL-variant Ser447Stop isassociated with high LPL activity and high HDL cholesterol[24,25].
Hepatic lipase
Hepatic lipase (HL) is produced in hepatic cells, and isactive at the surface of hepatic endothelial cells [24,26]. By
hydrolysing HDL triglycerides as well as HDL phospholi-pids, HL contributes to the metabolism of HDL [19,24,26].Hepatic lipase has the ability to generate pre
-HDL fromspherical HDL [27], and is involved in the generation of HDL
3
from HDL
2
[24,27]. A high activity of HL as meas-ured in postheparin plasma is associated with lower HDL cholesterol and smaller HDL particles [24]. Apo A-II maystimulate HL activity, which is possibly result of a greaterafnity of HL towards apo A-II compared with apo A-I[20,28].
Genetic HL deciency results in a moderately elevatedplasma HDL cholesterol [19,24] and larger HDL particles[24]. A common polymorphism in the HL gene promoteris associated with low HL activity, high HDL cholesteroland triglyceride enrichment of all lipoprotein classes [26].
Endothelial lipase
Endothelial lipase (EL) is a recently discovered lipase. Itsgene, the endothelial lipase gene (LIPG), is predominantlyexpressed in endothelial cells but also in other tissues[29,30]. In vivo
studies in mice reveal that EL shows pri-marily phospholipase activity and relatively little triglyceridelipase activity [29,30]. One study showed that a high degreeof EL overexpression in mice liver results in a decrease in
HDL cholesterol and apo A-I [31]. In LIPG transgenic micean inverse relationship between HDL and EL-expressionwas found [30]. Therefore, it is possible that EL is a phys-iological regulator in HDL metabolism, but much researchis necessary to characterize its exact role.
Lecithin:cholesterol acyltransferase
Lecithin:cholesterol acyltransferase (LCAT) is mainly secre-ted by the liver [32], is particularly active on pre
2
-HDL and catalyses the transfer of 2-acyl groups from lecithinor phosphatidylethanolamine to free (unesteried) choles-terol [13,24]. The LCAT reaction, which requires apo A-Ias cofactor, thereby results in the generation of cholesterylester molecules that by their hydrophobic nature areretained in the core of HDL particles. As a consequence,new unesteried cholesterol molecules, either derived fromtriglyceride-rich lipoproteins or from peripheral cells, canbe transferred to the surface of HDL particles, causing anincrease in HDL size. As HDL grows, the afnity of LCATfor the HDL surface lessens. Eventually, large sphericalHDL
2
that contain little or no LCAT are generated [13,33].The cholesterol esterication reaction in plasma is deter-mined by the activity of LCAT, i.e. the amount of activeLCAT in plasma, as well as by the plasma triglyceride con-centration [34], although manoeuvres that decrease plasmatriglycerides do not necessarily affect plasma cholesterolesterication [35]. In humans, plasma LCAT activity ispositively correlated with the HDL
2
as well as with theLpA-I/A-II level but not with HDL
3
and LpA-I [33]. Withhigher concentrations of apo A-II, LCAT reactivity seemsto be diminished [20,28,36]. Moreover, plasma cholesterol
esterication has been shown to be a determinant of theHDL cholesteryl ester concentration [37].Familial LCAT deciency is the result of mutations in the
LCAT gene that leads to a total loss of catalytic activity of this enzyme [32]. This disease is associated with markedlyreduced HDL cholesterol and apo A-I levels [32]. Intrigu-ingly, it is unusual for patients with familial LCAT de-ciency to develop premature coronary atherosclerosis [32].Nonetheless, accelerated atherosclerosis has been describedin patients with sh eye disease, which is caused by muta-tions in the LCAT gene that result in a partial loss of LCATactivity [32].
Cholesteryl ester transfer protein
In contrast to species such as mice and rats, human andrabbit plasma contains cholesteryl ester transfer protein(CETP) [38]. This lipid transfer protein enables the masstransfer and exchange of cholesteryl ester and triglyceridemolecules among lipoproteins [13,39,40]. Liver and fat tis-sue appear to be important sources of circulating CETP inman [40]. Between lipoprotein particles with a high choles-teryl ester content, such as spherical HDL as well as LDL,and triglyceride-rich lipoproteins this neutral lipid transferprocess results in a net gain of triglycerides and a net loss
8/13/2019 HDLdiabetes.pdf
4/19
1054
S. E. Borggreve et al.
2003 Blackwell Publishing Ltd, European Journal of Clinical Investigation
, 33
, 10511069
of cholesteryl ester in HDL and LDL, with reciprocalchanges in triglyceride-rich lipoproteins [19,22,3941].Between HDL and LDL, exchange of neutral lipids pre-dominates, and there is little mass transfer [39]. Consequentto this process, the HDL cholesteryl ester concentration isdecreased, whereas the HDL triglyceride content is
increased. As triglyceride molecules are larger than choles-teryl ester molecules, HDL size is increased. SubsequentHDL triglyceride hydrolysis by HL results in smaller-sized,cholesteryl ester-poor HDL, although CETP by itself is ableto reduce HDL size [27]. Cholesteryl ester transfer proteinand HL are therefore considered to act in concert in HDL
2
HDL
3
remodelling. Likewise, the process of neutral lipidtransfer between LDL and triglyceride-rich lipoproteins(TRLs) results in triglyceride-rich LDLs that are remod-elled to small dense LDLs by lipase action [42]. Impor-tantly, cholesteryl ester transfer should be considered toprovide a metabolic intermediate between high plasmatriglycerides and low HDL cholesterol [39,4345]. Further-more, neutral lipid transfer enhances the accumulationof cholesterol in chylomicrons, VLDL and intermediate-density lipoproteins, especially when clearance of triglyceride-rich lipoproteins is diminished [13,39,40]. Of note,LPL-mediated lipolysis is thought to enhance cholesterylester transfer from HDL to VLDL by facilitating transferof free fatty acids (FFA) to the VLDL surface [40,46]. Thecholesteryl ester transfer reaction is not only determined bythe amount of active CETP in plasma (designated CETPactivity) but also by the constellation of cholesteryl esterdonor (predominantly HDL) and acceptor (triglyceride-rich)lipoproteins [37,39,43,45,47]. Large-sized triglyceride-rich lipoproteins are better acceptors of HDL-derivedcholesteryl ester than small-sized triglyceride-rich lipopro-
teins [45], whereas the rate of cholesteryl ester transfer ispositively correlated with the phospholipid and unesteriedcholesterol content in VLDL [39]. In normolipidaemia,the concentration of triglyceride-rich lipoproteins providesa driving force for net cholesteryl ester transfer, and the choles-teryl ester transfer rate is determined by the triglyceride-richlipoprotein concentration [43]. In severe hypertriglyc-eridaemia, in contrast, the amount of active CETP becomesrate limiting [43]. In turn, cholesteryl ester transferwith HDL that contain apo A-I and apo A-II is lower thanthat with HDL containing only apo A-I [28]. There is astrong positive correlation between plasma CETP concen-tration and CETP activity [4850]. In addition, theamount of active CETP in plasma may also be affectedby a lipid transfer inhibitor protein (LTIP), recentlyidentied as apo F [51]. LTIP is associated with LDL and may preferentially suppress the neutral lipid transferprocess between LDLs and other lipoprotein particles[52]. Thus, cholesteryl ester transfer from HDLstowards triglyceride-rich lipoproteins may be enhanced,thereby ne tuning CETP-mediated neutral lipid transfer.Apo C-I is another protein with CETP activity-inhibitingproperties. In normolipidaemic plasma, this apolipoproteinhas been demonstrated to diminish CETP activity in aconcentration-dependent manner with high efciency[53].
High-density lipoprotein cholesterol levels are 36-foldelevated in genetic CETP deciency [54]. In this situationplasma cholesterol and triglycerides are only slightlyincreased. High-density lipoprotein
2
is elevated, and theseparticles are enormously large. LDL particles are smalland heterogeneous [54]. Expectedly, HDL is cholesteryl
ester-rich and triglyceride depleted, whereas VLDL and LDL are triglyceride rich and cholesteryl ester-poor [54]. GeneticCETP deciency may impair cellular cholesterol efux[55], despite elevated HDL cholesterol, and may lead todecreased cholesterol esterication [55]. The diminishedcellular cholesterol efux in genetic CETP deciency couldaccelerate atherosclerosis [55]. However, data concerninghuman CETP deciency are confusing, with some but notall studies showing accelerated atherosclerosis [38,54,56].Of various biallelic CETP polymorphisms, the intronicTaqIB polymorphism (B1B2) has been most extensivelystudied [57,58]. This polymorphism is closely linked to the
629 A/C polymorphism and to a tetranucleotide repeat inthe CETP gene promoter [59,60]. The B2 allele is associ-ated with higher HDL cholesterol, larger HDL particles,and lower plasma CETP activity and mass [57,58,61,62].Interestingly, this TaqIB polymorphism may interact withenvironmental factors such as alcohol use, smoking, obesity,insulin-dependent diabetes mellitus, and gender on HDL cholesterol [6366]. The B2 allele may lower coronaryartery risk [57,61,62,66]. Another common polymorphismis the I405V mutation [58]. The less frequent V allele isrelated to higher HDL cholesterol and lower plasma CETPconcentration and activity [58,67]. Remarkably, the V allelemay be associated with higher risk for cardiovascular dis-ease compared with wildtype I allele [67]. Another CETPgene variant (R451Q) is reported to affect plasma CETP
activity, intima media thickness in men and cardiovascularrisk in women [68].
Phospholipid transfer protein
Plasma from humans contains a second lipid transferprotein, designated phospholipid transfer protein (PLTP).Phospholipid transfer protein is synthesized in the liver, lungand adipose tissue but its main source in human plasma isstill unknown [69]. Phospholipid transfer protein facilitatesphospholipid and free cholesterol transfer between lipopro-teins during lipolysis [70], and may promote cholesterylester transfer towards triglyceride-rich lipoproteins [37,40].Moreover, PLTP is able to convert HDL in larger andsmaller particles [71,72]. During this HDL remodelling,pre
-HDL particles are generated that act as initialacceptors of cell-derived cholesterol [13,14,19,73,74].Remarkably, human plasma PLTP activity is not correlatedwith PLTP mass at least when assayed using monoclonalcapture antibodies [75]. Indeed, evidence is accumulat-ing that in humans circulating PLTP is only in part active[76].
Human genetic PLTP deciency has not been unequivo-cally described as yet, nor is the effect of PLTP polymor-phisms on lipoprotein metabolism clearly delineated.
8/13/2019 HDLdiabetes.pdf
5/19
HDL metabolism and reverse cholesterol transport in insulin resistance and type 2 diabetes mellitus
1055
2003 Blackwell Publishing Ltd, European Journal of Clinical Investigation
, 33
, 10511069
Figure 1 schematically shows the effects of lipases, LCAT
and lipid transfer proteins on HDL remodelling and Fig. 2depicts the CETP-mediated process of neutral lipid transferbetween HDL, TRL and LDL under normolipidaemiccircumstances.
High-density lipoprotein metabolism in insulinresistance and type 2 diabetes mellitus
As alluded to later, many of the changes in HDL meta-bolism that occur in insulin resistance and type 2 diabetesmellitus are pathophysiologically linked to elevated plasmatriglycerides. An overview on the pathogenesis of abnormaltriglyceride metabolism in insulin-resistant conditions hasbeen recently outlined elsewhere [77] and is beyond thescope of this review. Obviously, defects in the ability of insulin to affect glucose, triglyceride and FFA metabolismare interdependent [77,78].
Insulin-resistant subjects with or without type 2 diabetesmellitus show elevations in fasting plasma triglycerides andlow HDL cholesterol [11,79,80]. Postprandial triglycerideexcursions are larger and triglyceride clearance is delayedin type 2 diabetes mellitus [81]. Increased plasma triglyc-erides are the result of elevated VLDL triglycerides, whichare 153-fold higher in type 2 diabetes mellitus. The
magnitude of this increase depends on the co-occurrenceof obesity and the degree of glycaemic control [80]. Plasmatriglycerides are not higher in adequately controlled type 2diabetic patients with similar insulin sensitivity comparedwith healthy subjects [82]. HDL cholesterol is 1020%lower in unselected type 2 diabetic patients, which is mainlythe result of a decrease in HDL
2
and to some extent inHDL
3
[80,83]. The low HDL cholesterol in type 2 dia-betes mellitus is partly the result of a decrease in HDL cholesteryl ester and is accompanied by higher HDL trig-lycerides [35,37]. This decrease in the HDL cholesterylester/triglyceride ratio is more pronounced in obese type 2diabetic patients [84]. Furthermore, even when metaboliccontrol is adequate, free cholesterol and phospholipidson the HDL surface are decreased, resulting in an alteredviscosity [85]. Moreover, both decreases in LpA-I concen-tration but not in LpA-I/A-II [86], as well as decreases inLpA-I/A-II but not in LpA-I [87], have been documented
Figure 1 Effects of lipases, lecithin:cholesterol acyltransferase and
lipid transfer proteins on high-density lipoprotein remodellingin normolipidaemia. HDL: high-density lipoproteins; TRL:triglyceride-rich lipoproteins; FC: free cholesterol; PL:phospholipids; LPL: lipoprotein lipase; HL: hepatic lipase;LCAT: lecithin:cholesterol acyltransferase; CETP: cholesterylester transfer protein; PLTP: phospholipid transfer protein. Arrowheads indicate delivery of FC and PL to pre -HDL and sphericalHDL. Dotted arrows indicate stimulating effects of lipases, LCATand lipid transfer proteins on pre -HDL generation and HDLremodelling. Long arrows indicate HDL remodellingpathways.
Figure 2 Cholesteryl ester transfer protein-mediated process ofneutral lipid transfer between high-density lipoproteins,triglyceride-rich lipoproteins and low-density lipoproteins innormolipidaemia. HDL: high-density lipoproteins; TRL:triglyceride-rich lipoproteins; LDL: low-density lipoproteins;CE: cholesteryl ester; TG: triglycerides; CETP: cholesteryl estertransfer protein; LTIP: lipid transfer protein inhibitor protein.
Dotted arrows indicate stimulating effect of CETP on CE andTG transfer. Dotted arrows with a cross indicate inhibitingeffect of LTIP. Long arrows indicate CE and TG transfer.There is less CE and TG transfer between HDL and LDL (thinnerarrows) than between HDL and TRL and between LDLand TRL.
8/13/2019 HDLdiabetes.pdf
6/19
1056
S. E. Borggreve et al.
2003 Blackwell Publishing Ltd, European Journal of Clinical Investigation
, 33
, 10511069
in type 2 diabetes mellitus. These discrepancies are probablyattributable to differences in methodology as well as to theextent of hypertriglyceridaemia [86]. Pre
-HDL levels arereported to be elevated in hypertriglyceridaemic states[88,89], but surprisingly there are no reports comparing pre
-HDL in unselected type 2 diabetic patients with healthy
subjects. In type 2 diabetic patients matched with healthysubjects for HDL cholesterol, we found no signicantincrease in pre
-HDL formation [90].
Lipoprotein lipase
Lipoprotein lipase (LPL) activity can be measured in post-heparin plasma, as well as in adipose tissue and muscle.Post-heparin plasma LPL activity is probably affected byinsulin resistance as such and by the diabetic state. PlasmaLPL activity is reported to be decreased in insulin-resistantsubjects without diabetes [91], although the difference withinsulin-sensitive subjects did not always reach signicance[82]. Early studies showed decreased LPL activities inpostheparin plasma and in type 2 diabetes mellitus [92].More recently, we observed a lower postheparin plasma LPL activity in adequately controlled, insulin-resistant type 2diabetic subjects compared with type 2 diabetic patientswith relatively normal insulin sensitivity [82]. In that study,no difference was observed in LPL activity between type 2diabetic patients and nondiabetic subjects with a similardegree of insulin sensitivity [82]. A decreased LPL activityhas been documented in adipose tissue from type 2 diabeticpatients [84], although the insulin resistance- and diabetes-associated lowering of adipose tissue LPL activity has beenquestioned [93]. Muscle LPL activity is negatively related
both to plasma triglycerides and to the degree of insulinresistance [93].
Hepatic lipase
Hepatic lipase (HL) is also measured in postheparin plasma.Post-heparin HL activity correlates positively with insulinresistance in nondiabetic subjects [94], and in type 2 dia-betic patients [82,95]. Therefore, hyperinsulinaemia mayunderlay enhanced HL activity, which results in low HDL cholesterol. However, insulin administration decreases HL activity [95]. Thus, the effects of insulin resistance and of short-term exogenous hyperinsulinaemia on the HL activityshould be discerned.
A decreased postheparin plasma LPL/ HL ratio has beenobserved in insulin-resistant subjects without and withdiabetes [82,91]. Such a decreased LPL/HL ratio is adeterminant of low HDL
2
cholesterol [91].
Endothelial lipase
As yet, no data are available with respect to possible abnor-malities in EL in insulin resistance and type 2 diabetesmellitus.
Lecithin:cholesterol acyltransferase
Established methods for assaying cholesterol estericationin total plasma include measurement of changes in plasma-free cholesterol mass after incubation of plasma [96] anddetection of radiolabelled cholesteryl ester after plasma
incubation with radiolabelled free cholesterol [97]. Suchassays depend on the chemical composition of the substratelipoproteins as well as on the amount of active LCAT,and reect the actual situation in vivo
[97]. Plasma LCATactivity can also be measured with exogenous substrateassays [98]. The effect of endogenous plasma lipoproteinsubstrates is minimized, so that the plasma LCAT activitylevel reects the amount of active protein. Accordingly, LCATactivity assayed by these latter methods are strongly cor-related with its plasma concentration [98], which can bemeasured with specic immunochemical assays [99]. Theterms plasma cholesterol esterication and LCAT activityare frequently used interchangeably. Obviously, one shoulddiscern between these two types of assay systems. We usethe terms plasma cholesterol esterication and LCAT activ-ity to indicate cholesterol esterication and LCAT activity
per se
, respectively. Plasma cholesterol esterication is unal-tered [100,101] or increased [37,102] in type 2 diabeticpatients. As plasma triglycerides determine the rate of cho-lesterol esterication [34,37], the absence of higher plasmatriglyceride levels in type 2 diabetes mellitus compared withhealthy subjects in some of these reports [101] may explainat least in part this discrepancy. Plasma cholesterol esteri-cation is increased in insulin-resistant type 2 diabeticpatients compared with insulin-sensitive healthy subjects,reecting the relationship between insulin sensitivity andplasma triglyceride levels [82]. Plasma LCAT activity is
reported to be increased in insulin-resistant subjects withoutdiabetes [11] and in type 2 diabetic subjects [37] but in thelatter study the difference disappeared after excludinghypertriglyceridaemic patients [37].
Cholesteryl ester transfer protein
Endogenous assay systems assess cholesteryl ester transferbetween HDL particles and apo B-containing lipoproteinsby measurement of changes in lipoprotein cholesteryl esterafter incubation of plasma under conditions of LCATinhibition, or by measurement of changes in specic radio-activity of cholesteryl ester donor or acceptor lipoproteins.Exogenous assays measure plasma CETP activity as transferof radiolabelled cholesteryl ester between LDL and HDL [103]. Exogenous substrates, i.e. is LDL or HDL, are addedin excess, minimizing the effect of endogenous lipoproteinson plasma CETP activity measurement. Plasma CETPactivity assayed this way is strongly correlated with CETPmass [48,49]. Clearly, the results obtained from endo-genous and exogenous substrate assays provide differentinformation about the process of cholesteryl ester transfer.We use the results from endogenous and exogenoussubstrate assays to designate plasma CETP activity andcholesteryl ester transfer, respectively. Plasma cholesteryl ester
8/13/2019 HDLdiabetes.pdf
7/19
HDL metabolism and reverse cholesterol transport in insulin resistance and type 2 diabetes mellitus
1057
2003 Blackwell Publishing Ltd, European Journal of Clinical Investigation
, 33
, 10511069
transfer is found to be increased in insulin-resistant subjectswithout diabetes with to insulin-sensitive individuals [82].With one exception [104] plasma cholesteryl ester transfereither between HDL and VLDL + LDL or between HDL and VLDL is elevated in adequately controlled type 2diabetic patients with moderately elevated triglycerides
compared with healthy subjects [37,105,106]. Plasmacholesteryl ester transfer, if evaluated, was positivelycorrelated with plasma triglycerides in all these studies[37,104,105]. While cholesteryl ester transfer from HDL toVLDL is enhanced, the transfer from HDL to LDL isdecreased in type 2 diabetes mellitus [105]. The enhancedcholesteryl ester transfer from HDL to VLDL is the resultof an increased ability of VLDL to accept cholesteryl esterfrom HDL [106]. Generally, there is no difference in plasmaCETP activity between insulin-sensitive and insulin-resistant subjects [11], and between type 2 diabetic andhealthy subjects [37,84,104,105,107]. Some data point toa slightly lower plasma CETP activity in type 2 diabetesmellitus [108]. These studies emphasize the importance of insulin resistance-related and diabetes-related changes inthe constellation of cholesteryl ester acceptor lipoproteinsto explain the enhanced plasma cholesteryl ester transfer.Plasma CETP activity is unaltered or decreases modestlyafter insulin infusion [84,107,108]. In accordance withincreased cholesteryl ester transfer in hypertriglyceridae-mia, plasma cholesteryl ester transfer decreases in parallelwith a decrease in plasma triglycerides after exogenousinsulin [35]. Finally, it is noteworthy that together with theplasma triglyceride concentration plasma CETP activity isa determinant of small dense LDL in type 2 diabetesmellitus [109].
Phospholipid transfer protein
Plasma PLTP activity can be measured with radio-isotopesusing a phospholipid vesicles-exogenous HDL system[110]. Plasma PLTP activity so assayed specically reectsthe amount of active PLTP [111,112]. As yet, it appearsthat there is only a weak positive correlation between PLTPmass and activity when applying polyclonal rabbit anti-bodies against human PLTP [113]. Plasma PLTP activity hasbeen reported to be elevated [84] in type 2 diabetic patientsin association with high plasma triglycerides and obesity[37]. Likewise, when comparing insulin-resistant withinsulin-sensitive subjects without diabetes mellitus, a higherplasma PLTP activity is related to insulin resistance in men[84,94] and in women only [114]. In another study, wefound no increase in plasma PLTP activity in type 2 diabeticpatients but they were matched for HDL cholesterol withhealthy subjects [115]. Plasma PLTP mass, measured withpolyclonal antibody ELISA, is elevated in type 2 diabetesmellitus [113], but we did not observe a higher plasmaPLTP mass, measured with a monoclonal antibody ELISA,despite elevated plasma PLTP activity levels [50]. So, theremay be relatively more active PLTP in diabetic plasma.Interestingly, various studies reported relationships betweenhigh plasma PLTP activity, elevated plasma triglycerides
[37,84,105,111] and indexes of obesity [84,111,116,117].Indeed, plasma PLTP activity is not elevated in type 2diabetic patients with a relatively normal body mass index[84,108]. However, given the interrelationships betweenobesity, insulin resistance and high plasma triglycerides,it is difcult to discern between the independent effects of
these parameters on PLTP regulation. Manoeuvres decreasingplasma FFA and triglycerides like insulin infusion and acip-imox administration decrease PLTP activity [84,108,115].In (obese) type 2 diabetic patients the decrease in plasmaPLTP activity after insulin appears to be blunted [84], sug-gesting that high plasma PLTP activity levels in insulin-resistant states could be in part due to a diminishedlowering by insulin. Conversely, an intravenous fat loadraises plasma PLTP activity [94]. Insulin resistance on lipidmetabolism may be a common denominator for theseinterrelationships between the regulation of plasma FFA,triglycerides and PLTP activity but the responsible mole-cular mechanisms remain to be explained. Of interest, anincreased HDL triglyceride content coinciding withhigh plasma triglycerides enhances pre
-HDL formation[88,118]. Thus, high plasma triglycerides and PLTP activitylevels possibly act together in promoting HDL conversion.
Figure 3 shows abnormalities in HDL remodelling in rela-tion to lipases, LCAT and lipid transfer proteins in insulin
Figure 3 Effects of lipases, lecithin:cholesterol acyltransferaseand lipid transfer proteins on altered high-density lipoproteinremodelling in insulin resistance and type 2 diabetes mellitus.HDL: high-density lipoproteins; TRL: triglyceride-richlipoproteins; FC: free cholesterol; PL: phospholipids; LPL:lipoprotein lipase; HL: hepatic lipase; LCAT: lecithin:cholesterolacyltransferase; CETP: cholesteryl ester transfer protein; PLTP:phospholipid transfer protein. TRL pool is increased (larger circle);pre -HDL is depicted as increased (larger area), but note that datain insulin resistance and type 2 diabetes mellitus are limited; bothHDL 2 and HDL 3 are decreased but this is more pronounced forHDL 2 (smaller circles) than for HDL 3 (smaller circles).Lipoprotein lipase-mediated TRL hydrolysis is diminished resultingin less transfer of FC and PL from TRL to pre -HDL and sphericalHDL (shorter dotted arrow and smaller arrow head). Stimulatoryeffects of HL and PLTP on HDL remodelling are increased(thicker dotted arrows). Effects of LCAT and CETP are depictedas unaltered. Pre -HDL generation from HDL 3, as well as HDL 2 towards HDL 3 remodelling are increased (thicker long arrows).
8/13/2019 HDLdiabetes.pdf
8/19
1058
S. E. Borggreve et al.
2003 Blackwell Publishing Ltd, European Journal of Clinical Investigation
, 33
, 10511069
resistance and type 2 diabetes mellitus. Figure 4 illustratesalterations in the CETP-mediated process of neutral lipidtransfer in insulin resistance and type 2 diabetes mellitus.
Reverse cholesterol transport
That HDL has important cardioprotective properties isundisputed [3,21,119]. One of the antiatherogenic proper-
ties of HDL is exerted by its function to scavenge peripheraltissue-derived cholesterol in the RCT pathway [120]. Indeed,infusion of heterologous or acetylated LDL increases cir-culating HDL cholesterol in rabbits, suggesting that theselipoproteins are able to clear LDL-derived cholesterol fromtissues [121]. Two lines of in vivo
evidence directly indicate
that in mammals a system exists, which is capable of effectively removing cholesterol from the arterial wall. Thisevidence also indicates that HDL has this ability, therebyretarding or even reversing atherosclerosis. Firstly, cholesteroluxes were studied in the aortic intima-media of normo-lipidaemic humans who underwent aortic valve replacementand were free of visible atherosclerosis [122]. Applying infusionof homologous radiolabelled plasma, the mean cholesterolturnover time in the aortic intima-media layer amounted to17 years, providing a measure of cholesterol inux [122].In comparison with the mean age of 62 years of the studysubjects these observations indicate that removal of choles-terol must be a major determinant of aortic tissue cholesterolcontent. Second, it was demonstrated that weekly HDL infusions in rabbits during the last 30 days of a 90-day cho-lesterol feeding period reduces aortic cholesterol content by55% and the atherosclerotic lesion area by 50% [123]. Thus,direct in vivo
evidence exists that HDL administration doesnot only inhibit progression but also reverses establishedatherosclerosis. Although HDL is cardioprotective [3,21,119],it is important to realize that the level of circulating HDL cholesterol cannot be regarded as a measure of the dynamicsof HDL cholesterol transport and thus will not necessarilyindicate the efcacy of HDL-mediated RCT. High-densitylipoprotein cholesterol elevations could therefore reectdiminished HDL clearance and, hence, an impaired RCT[119]. Conversely, low HDL cholesterol could in theory
also be attributable to increased HDL removal in terms of hepatic cholesterol metabolism and biliary excretion.It is commonly thought that the RCT pathway consists
of the following different steps: (i) efux of cholesterol fromperipheral cells to extracellular acceptors, mainly pre
-HDL, (ii) subsequent LCAT-mediated esterication of freecholesterol within HDL contributing to HDL remodelling,(iii, a) direct uptake of HDL-derived cholesterol by the liver,(iii, b) indirect uptake of HDL-derived cholesteryl ester bythe liver via CETP-mediated transfer to apo B-containinglipoproteins, and (iv) metabolism of cholesterol in the liver,followed by biliary excretion (IV).
Efux of cholesterol from peripheral cells toextracellular acceptors
Cholesterol efux out of plasma membranes of peripheralcells to extracellular acceptors can occur through variousmechanisms including fast specic energy-dependent andpassive slow diffusion-type processes [19,28]. Apo A-I onpre
1
-HDL promotes cellular cholesterol efux. Its uniqueconformation on these particles [13] allows for bothmechanisms [28]. However, pre
1
-HDL is not essentialfor cholesterol efux out of broblasts and macrophages
in vitro
[124]. Also, scavenger receptor class B type I (SR-BI)
Figure 4 Abnormalities in cholesteryl ester transfer protein-mediated neutral lipid transfer between high-density lipoproteins,triglyceride-rich lipoproteins and low-density lipoproteins ininsulin resistance and type 2 diabetes mellitus. HDL: high-densitylipoproteins; TRL: triglyceride-rich lipoproteins; LDL: low-densitylipoproteins; CE: cholesteryl ester; TG: triglycerides; CETP:cholesteryl ester transfer protein; LTIP: lipid transfer proteininhibitor protein. TRL pool is increased (larger circle); HDL CEis decreased (smaller circle); LDL size is decreased (smaller circle)consequent to enhanced CE and TG transfer with TRL andsubsequent triglyceride hydrolysis. Cholesteryl ester transferprotein activity is depicted as unchanged (dotted arrows);LTIP action is depicted as unchanged (dotted arrows) with aquestion mark, as there are no data on insulin resistance and type2 diabetes mellitus. There is more CE and TG transfer betweenHDL and TRL (thicker arrows) and between LDL and TRL(thicker arrows), and less CE and TG transfer between HDL andLDL (thinner arrows).
8/13/2019 HDLdiabetes.pdf
9/19
HDL metabolism and reverse cholesterol transport in insulin resistance and type 2 diabetes mellitus 1059
2003 Blackwell Publishing Ltd, European Journal of Clinical Investigation, 33 , 10511069
[14,125] and ATP binding cassette transporter 1 (ABCA1)[19,126] seem to be important in fast, specic cholesterolefux. SR-BI can promote free cholesterol efux by a mech-anism where cell-surface-acceptor binding is relativelyunimportant [14]. ABCA1 is a key factor in intracellularlipid transport and in subsequent transmembrane lipid ux
to extracellular apo A-I by forming an aqueous pore on thecell surface [126]. Besides apo A-I, apo A-II is complexlyinvolved in cellular cholesterol efux. LpA-I/A-II particlesonly induce non-specic cholesterol efux [28], accountingfor the reduced efux to such particles [20,28,127]. ApoA-II binds well to SR-BI [20,127,128], and may negativelymodulate SR-BI-mediated cholesterol efux in vitro [127].In contrast, Apo A-II enhances efux after binding toABCA1 [127]. Furthermore, apo A-II may stimulate HL activity in vitro [28] and is able to displace apo A-I fromHDL, thereby contributing to the generation of pre -HDL [20]. It seems that apo A-II could therefore haveboth cellular cholesterol efux inhibiting and stimulatingproperties.
LCAT-mediated esterication of free cholesterolwithin HDL and HDL remodelling
Cell-derived free cholesterol, contained within pre -HDL-particles, is subsequently esteried by LCAT, allowingpre -HDL to become a migrating HDL 3 [13]. Cholesterylester is more hydrophobic than free cholesterol and migratesaway from the HDL surface, enabling uptake of other freecholesterol molecules [13]. The LCAT reaction was initiallyhypothesized to be the rate-limiting step in the RCT path-way [120,129]. It is now clear that LCAT is able to impede
cellular cholesterol inux rather than to stimulate efux[130,131]. Moreover, the plasma cholesterol estericationrate is not correlated with the efux of radiolabelledcholesterol from Fu5AH cells [132], a cell line that exp-resses SR-BI but hardly any ABCA1. As outlined earlierand depicted in Fig. 1, enlargement of HDL requires accept-ance of more phospholipids and apolipoproteins, whereasfurther lipid loading results in HDL 2 generation [18].
Direct uptake of HDL-derived cholesterol bythe liver
Direct hepatic removal of HDL-derived cholesterol involvesinteraction with several receptors on the hepatocyte cellmembrane. SR-BI stimulates uptake of HDL. In a pro-posed process called selective transcytosis [133], HDL par-ticles bind reversibly to SR-BI [14,125] leading to selectivetransfer of cholesteryl ester into the cellular cholesterol pool[133]. SR-BI-mediated cholesteryl ester uptake is impairedin apo A-I knock-out mice [128], and is diminished withLpA-I/A-II compared with LpA-I particles [134]. Apo Emay increase SR-BI-mediated selective cholesterol uptake[135]. Hepatic lipase enhances the binding of HDL toSR-BI [136], thereby indirectly promoting uptake of HDL cholesterol in the liver [24,27,137]. HDL also binds to a
recently described apo A-I receptor, which is the ectopicallyexpressed -chain of ATP synthase [138], resulting in gen-eration of extracellular ADP and in subsequent endocytosis.This endocytosis does not involve SR-BI or ABCA1 [138].The importance of this receptor for hepatic removal of HDL-derived cholesterol is not known.
Indirect uptake of HDL-derived cholesteryl ester by the liver via CETP-mediated transfer to apoB-containing lipoproteins
The CETP-mediated cholesteryl ester transfer from HDL towards apo B-containing lipoproteins such as LDL andVLDL provides a second route transporting HDL-derivedcholesterol to the liver. As cholesteryl ester mass transfer ismost outspoken between HDL and triglyceride-richlipoproteins [39], it is likely that HDL-derived cholesterolwill be predominantly cleared by hepatocyte receptors thatinteract with chylomicron remnants, VLDL and VLDL rem-nants [41,139141]. Its seems plausible that the interactionbetween LDL and its receptor plays a relatively minor rolein RCT. Very low-density lipoprotein is cleared via endo-cytosis by the LDL receptor [40], and by the LDL receptor-related protein (LRP), also designated as the VLDL receptor[139]. Chylomicron and VLDL remnants are also taken upin the liver via the LRP [139]. The initial binding site maybe formed by cell-surface heparan sulphate proteoglycans[140]. Binding of VLDL is stimulated by HL and by LPL,which acts as a ligand when contained within these lipopro-tein particles, but for subsequent degradation apo E isrequired [140]. The small fraction of HDL that contains apoE is also cleared via the LDL receptor and the LRP [141].
Note that in quantitative terms the relative importanceof the indirect route for hepatic uptake of HDL-derivedcholesterol via apo B-containing lipoproteins vs. the directroute for hepatic uptake of cholesterol contained in HDL isnot known.
Metabolism of cholesterol in the liver, followed by biliary excretion
Ultimately, cholesterol is excreted in the biliary tract, largelyafter conversion to bile acids. Microsomal cholesterol7- -hydroxylase facilitates the rst cholesterol conversionstep in the liver [142]. After various subsequent hydroxyl-ation and oxido-reduction steps, chenodeoxycholic acid andcholic acid are formed. Conjugation of these bile acids withtaurine and glycine renders them more hydrophilic, facili-tating their biliary excretion. Intestinal bacterial enzymesconvert chenodeoxycholic acid and cholic acid in secondarybile acids, which can re-enter the circulating bile acid poolafter reabsorption. Hepatic 7- -hydroxylase activity appearsto be the rate-limiting step for bile acid synthesis, providinga regulatory mechanism for hepatic cholesterol removal[142]. Interestingly, human PLTP overexpression in miceenhances the cholesteryl ester content of hepatic tissueand increases faecal bile acid excretion [143]. Hepatobiliary
8/13/2019 HDLdiabetes.pdf
10/19
1060 S. E. Borggreve et al.
2003 Blackwell Publishing Ltd, European Journal of Clinical Investigation, 33 , 10511069
cholesterol transport was found to be unaltered in experi-mental ABCA1 deciency [144].
Figure 5 schematically depicts the RCT pathway undernormolipidaemic circumstances.
Reverse cholesterol transport in insulin resistanceand type 2 diabetes mellitus
Current knowledge is far from complete but it is likely
that there are multiple abnormalities in various steps of theRCT pathway in insulin resistance and type 2 diabetesmellitus.
Efux of cholesterol from peripheral cells to
extracellular acceptors
In general, the impact of metabolic disorders on cholesterolefux to plasma can be studied in two ways. First, the effectof extracellular acceptors on cellular cholesterol efux canbe evaluated while leaving the in vitro cell characteristicsunaltered. Second, cells can be obtained from diseased sub-jects or be modied in vitro to document the effect of specicmetabolic abnormalities on cholesterol efux at the cellularlevel. Cholesterol efux from Fu5AH model cells, a widelyused cell system [14,132], is positively correlated with HDL phospholipids, HDL cholesterol, apo A-I as well as with pre-HDL [89,90,127,132]. Using these cells, it is suggestedthat cellular cholesterol efux to plasma from insulin-resistantsubjects is maintained despite lower HDL cholesterol [89].This may be attributable to higher pre -HDL formationin association with increased plasma triglycerides andplasma PLTP activities in insulin resistance. Elevatedplasma triglycerides coincide with a relative increase in theHDL phospholipid content [145]. As cell cholesterol efuxis positively related to HDL phospholipids [89], this mayexplain why cholesterol efux from Fu5AH cells to hyper-triglyceridaemic plasma can be unaltered [145]. Althoughthese data suggest that low HDL cholesterol does notnecessarily imply an impaired rst RCT step, cholesterolefux from Fu5AH cells to plasma with low HDL cholesterolis reported to be diminished [146]. Importantly, the cell line
used probably affects the extent and dynamics of cellularcholesterol efux, as evidenced by different results whenusing Fu5AH cells compared with macrophage-like J774cells, a cell line that predominantly expresses ABCA1[127,146]. Cholesterol net transport from cultured bro-blasts to severely hyperglycaemic plasma may be impaired,an abnormality that is reversed after blood glucose loweringwith insulin [147]. Cholesterol efux out of Fu5AH cellsto diabetic plasma is also diminished [86,148]. However,when comparing efux from Fu5AH cells to plasma of diabetic and healthy subjects matched for HDL cholesterol,no differences in efux appeared [90]. Cellular cholesterolefux is not correlated to plasma apo A-I in type 2 diabeticpatients in contrast to healthy subjects [90]. Instead, efuxout of Fu5AH cells is positively related to the plasma LpA-I/A-II concentration in type 2 diabetes mellitus [86,148].Decreased LpA-I/A-II levels [87] may therefore contributeto a lower cellular cholesterol efux in type 2 diabetesmellitus. The effect of HDL glycation is controversial. In vitroglycation of HDL 3 impairs cholesterol efux from humanskin broblasts [149]. The ability of glycated LpA-I topromote efux out of Fu5AH cells is also diminished [150].However, no effect of HDL 3 glycation on cholesterol efuxout of mouse peritoneal macrophages was observed [151].
Concerning cell-related changes on cholesterol efux,supraphysiological concentrations of insulin impair cellular
Figure 5 Reverse cholesterol transport in normolipidaemia.HDL: high-density lipoproteins; LDL: low-density lipoproteins;TRL: triglyceride-rich lipoproteins. FC: free cholesterol; CE:cholesteryl ester; HL: hepatic lipase; LCAT: lecithin:cholesterolacyltransferase; CETP: cholesteryl ester transfer protein; PLTP:phospholipid transfer protein; SR-BI: scavenger receptor B-I;ABCA-1: ATP-binding cassette transporter A1; LRP: LDLreceptor-related protein; *other mechanisms including unmediatedaqueous diffusion and apolipoprotein interactions with the plasmamembrane. Note that only pre -HDL as acceptor of cell-derivedcholesterol is shown. The importance of the ectopically expressed-chain of ATP synthase for removal of HDL-associated cholesterolis not known (?). Long arrows indicate cholesterol transport routes.Dotted arrows indicate stimulatory effects of HL, LCAT and lipidtransfer proteins.
8/13/2019 HDLdiabetes.pdf
11/19
HDL metabolism and reverse cholesterol transport in insulin resistance and type 2 diabetes mellitus 1061
2003 Blackwell Publishing Ltd, European Journal of Clinical Investigation, 33 , 10511069
HDL binding as well as HDL-mediated cholesterol efuxfrom broblasts in vitro , suggesting that very high levels of insulin decrease the rst step in RCT [152]. Moreover, ithas been shown that advanced glycation end products,as accumulating in the diabetic state, may interfere withSR-BI-mediated cholesterol efux in vitro [125,153].
Furthermore, when J774 macrophages are incubated withunsaturated FFA, in order to mimic elevated FFA levels asobserved in insulin resistance and type 2 diabetes mellitus,cellular cholesterol efux is decreased, consequent todiminished cellular ABCA1 expression [154]. In peritonealmacrophages from insulinopenic diabetic mice, ABCA1mRNA expression is markedly decreased [155]. Thisabnormality is reversed by adding insulin, but is unlikelyowing to an effect of insulin itself [156]. In both studies,coincubation with saturated FFA had no effect on cellularABCA1 abundancy nor on cellular cholesterol efux[154,156]. ATP binding cassette transporter 1 mRNAexpression in circulating mononuclear cells from type 2diabetic patients is reduced compared with healthy subjects[155].
Taken together, these ndings suggest that cholesterolefux from peripheral cells to plasma is impaired in the dia-betic state, consequent to lipoprotein acceptor changes andto cellular abnormalities. In insulin resistance, however, theability of plasma to stimulate cellular cholesterol efux maybe unaltered. In this situation, it is uncertain whethercellular abnormalities, consequent to hyperinsulinaemiaand FFA elevations, will result in a diminished cholesterolremoval.
LCAT-mediated esterication of free cholesterol
within HDL and HDL remodelling
As described earlier and depicted in Fig. 3, several mecha-nisms are probably involved in altered HDL remodelling ininsulin resistance and type 2 diabetes mellitus. Pre -HDL formation may be increased as a result of higher plasmaPLTP and HL activities, HDL triglyceride enrichment andenhanced PLTP-mediated phospholipid transfer from theenlarged triglyceride-rich lipoprotein pool to pre -HDL [27,72,73,118]. Free cholesterol transport from this pool toHDL 3 may be increased. Moreover, higher plasma PLTPand HL activities stimulate HDL 2 towards HDL 3 remod-elling. In view of the to some extent inconclusive data con-cerning plasma cholesterol esterication [37,82,100102],we assume that the cholesterol esterication-related effectson HDL remodelling are unchanged in insulin resistanceand type 2 diabetes mellitus. Furthermore, elevated plasmatriglycerides in insulin resistance and type 2 diabetesmellitus increase the cholesteryl ester transfer process out of HDL, thereby causing cholesteryl ester depletion and trig-lyceride enrichment of these particles [35,37]. This effectcould be accentuated by glycation of (apo) lipoproteins indiabetes, which may further enhance plasma cholesterylester transfer [157]. High-density lipoprotein catabolism isincreased as a result of HDL triglyceride enrichment [158].The consequence of all these abnormalities is a decreased
HDL cholesterol which is more pronounced for HDL 2 thanfor HDL 3 [83].
Direct uptake of HDL-derived cholesterol by the liver
Apart from effects of changes in circulating HDL (subfrac-tion) levels, the direct pathway of HDL-derived cholesterolbinding and uptake in the liver may be abnormal in insulinresistance and type 2 diabetes mellitus in vivo . Although SR-BI mRNA expression is unaltered in circulating mononu-clear cells from type 2 diabetic patients [155], selectiveHDL cholesteryl ester uptake via SR-BI may be modiedin type 2 diabetes mellitus. It is possible that high plasmaHL activity as found in insulin resistance and type 2 diabetesmellitus [11,82,95] stimulates HDL binding to SR-BI. Onthe other hand, advanced glycation end products can inhibitSR-BI-mediated selective HDL cholesteryl ester uptake inHepG2 cells by interference with intracellular processing[153]. However, the consequences for these apparentlyopposite effects of high plasma HL activity and of elevationsin advanced glycation end products in diabetes on thedynamics and efcacy of SR-BI-mediated HDL cholesterylester uptake in the liver are still unknown.
Indirect uptake of HDL-derived cholesteryl ester by the liver via CETP-mediated transfer to apoB-containing lipoproteins
Data concerning uptake of apo B-containing lipoproteinsvia the LDL receptor and the LRP in insulin resistance andtype 2 diabetes mellitus are limited. Using HepG2 cells,
LDL receptor-mediated uptake and degradation of LDL obtained from hypertriglyceridaemic diabetic plasma is lesseffective than that of LDL isolated from plasma of nondi-abetic hypertriglyceridaemic subjects and that of in vitro gly-cated LDL [159]. Moreover, the latter two LDL fractionsbind less effectively to this receptor than normal LDL [159].As LDL receptor mRNA expression in mononuclear cellsfrom type 2 diabetic patients is unchanged [155], the dimin-ished LDL receptor-mediated LDL degradation [159] maypoint to post-translational modication of LDL receptoraction. Insulin resistance-associated and type 2 diabetesmellitus-associated alterations in the LDL receptor pathwayare possibly less important for RCT than abnormalitiesin the LRP pathway, because net cholesteryl ester masstransfer out of HDL is much greater to triglyceride-richlipoproteins than to LDL [39]. The scanty data concerningLRP-mediated cholesterol uptake in insulin resistance andtype 2 diabetes mellitus are inconclusive. LDL receptor-related protein mRNA expression in skeletal tissue fromtype 2 diabetic patients is lower [160], whereas its expressionin mononuclear cells is unaltered [155]. Nonetheless, VLDL catabolism is probably impaired in type 2 diabetes mellitusas witnessed by a decreased fractional catabolic rate of VLDL triglycerides and apo B in type 2 diabetes mellitus[161], which is compatible with a decreased VLDL-mediatedtransport of HDL-derived cholesteryl ester to the liver [162].
8/13/2019 HDLdiabetes.pdf
12/19
1062 S. E. Borggreve et al.
2003 Blackwell Publishing Ltd, European Journal of Clinical Investigation, 33 , 10511069
Metabolism of cholesterol in the liver, followed by biliary excretion
Early data have shown that cholesterol synthesis, faecalbile acid excretion and bile acid pool size are elevatedduring uncontrolled hyperglycaemia in type 2 diabeticpatients [163]. However, the interpretation of these changesin terms of altered RCT is unclear. To date no studies haveevaluated hepatic cholesterol metabolism of HDL-derivedcholesterol and subsequent hepatobiliary cholesterol andbile acid transport in insulin resistance and type 2 diabetesmellitus. It is unknown whether elevated PLTP activityassociated with these conditions affects this step in RCT, asdemonstrated by experimental PLTP overexpression [143].
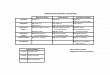
Table 1 summarizes available data with respect to abnormali-ties in RCT in insulin resistance and type 2 diabetes mellitus.
Strategies to inhibit plasma cholesteryl estertransfer and cholesteryl ester transfer proteinactivity
As discussed earlier in this review CETP is able to lowercholesteryl ester in HDL and to raise cholesteryl ester in
triglyceride-rich lipoproteins. Moreover, an enhanced choles-teryl ester transfer provides a plausible metabolic inter-mediate for the exchange between high plasma triglyceridesand low HDL cholesterol as observed in insulin resistanceand type 2 diabetes mellitus. Of interest, experimental datain rats transgenic for human CETP show that CETP maybe proatherogenic [164]. It is therefore of clinical relevanceto ascertain the effects of lipid-lowering drugs (statins andbrates) on plasma cholesteryl ester transfer and CETPactivity. Moreover, the effects of recent approaches tospecically inhibit CETP on HDL metabolism and onatherosclerosis will be outlined.
Evidence for an effect of statin treatment on plasmacholesteryl ester transfer and CETP activity is derived fromthe following studies. In hypertriglyceridaemic [165] andcombined hyperlipidaemic subjects [166], LDL cholesterollowering in response to atorvastatin is accompanied by asmall decrease in plasma CETP activity. In familiar hyper-cholesterolaemia, pravastatin markedly decreases plasmacholesteryl ester transfer without affecting plasma CETPconcentration [167]. A drop in plasma cholesteryl estertransfer after pravastatin treatment has also been demon-strated in type 2 diabetes mellitus [168]. Finally, simvastatindecreases plasma CETP concentration in normolipidaemicsubjects [169], whereas this treatment results in a
Table 1 Abnormalities in reverse cholesterol transport in insulin resistance and type 2 diabetes mellitus
Efux of cholesterol from peripheral cells to extracellular acceptorsResulting from abnormalities in extracellular acceptors
Insulin resistance May be unalteredType 2 diabetes mellitus Impaired
Resulting from cellular abnormalitiesInsulin resistance UnknownType 2 diabetes mellitus Impaired
LCAT-mediated esterication of free cholesterol within HDL and HDL remodellingInsulin resistance Cholesterol esterication proposedly unchanged, multiple abnormalities
in HDL remodellingType 2 diabetes mellitus Idem
Direct uptake of HDL-derived cholesterol by the liverUptake of HDL-derived cholesterol via scavenger receptor class B type I
Insulin resistance Stimulatory effect of high hepatic lipase activity possibleType 2 diabetes mellitus Stimulatory effect of high hepatic lipase activity possible;
Inhibitory effect of advanced glycation end products possible; net effectunknown
Indirect uptake of HDL-derived cholesteryl ester by the liver via CETP-mediated transfer to apo
B-containing lipoproteinsVia LDLLDL receptor interaction
Insulin resistance UnknownType 2 diabetes mellitus Impaired LDL receptor-mediated LDL degradation
Via TRLLRP interactionInsulin resistance Unknown; effect of high hepatic lipase activity unknownType 2 diabetes mellitus Possibly impaired as reected by diminished VLDL catabolism
Via TRLLDL receptor interactionInsulin resistance UnknownType 2 diabetes mellitus Unknown
Metabolism of cholesterol in the liver, followed by biliary excretionInsulin resistance UnknownType 2 diabetes mellitus Unknown
8/13/2019 HDLdiabetes.pdf
13/19
HDL metabolism and reverse cholesterol transport in insulin resistance and type 2 diabetes mellitus 1063
2003 Blackwell Publishing Ltd, European Journal of Clinical Investigation, 33 , 10511069
nonsignicant decrease in plasma CETP activity in rabbits[170].
In general, plasma CETP concentration remains unalteredafter treatment with gembrozil or bezabrate [171,172],whereas plasma CETP activity has been variably reported todecrease [173175], to remain unchanged [176] or to increase
slightly [177] after brate treatment. Plasma cholesterylester transfer is lowered in response to gembrozil, beza-brate and fenobrate therapy, probably as a consequenceof a fall in triglyceride-rich lipoproteins [171,174]. A studyin normolipidaemic subjects showed a diminished ability of HDL to provide cholesteryl esters for neutral lipid transferafter gembrozil [176].
Plasma CETP activity can be specically inhibited withchemical agents [170,178181], and with antisense oligo-nucleotides [182]. Furthermore in rabbits, administrationof CETP antibodies [183] and active vaccination againstCETP [184] lower its activity in plasma. Chemical agentsthat specically inhibit CETP include JTT-705, SC 71952and CGS 25159 [170,178181]. JTT-705 and SC 71952act by forming disulphide bonds with Cys-13 of CETP[170,179,181], which is probably located near its neutrallipid-binding site [179]. Orally administered CETP inhi-bitors increase apo A-I and HDL cholesterol with a greaterrise in HDL 2 than in HDL 3, and decrease VLDL + LDL cholesterol in both rabbits [170] and humans [181]. In rab-bits, JTT-705 treatment decreases plasma CETP activity by95% [170]. Of major importance, this treatment in rabbitsinhibits progression of aortic atherosclerosis [170]. Further-more, the ability of HDL to promote cholesterol efux from
J774 macrophages in vitro remains unaffected after JTT-705treatment [180]. In view of the rise in HDL cholesterol afterCETP inhibitor and the efux-promoting effects of a high
HDL cholesterol concentration, this suggests that JTT705treatment may stimulate the rst step of RCT. Treatmentwith this CETP inhibitor at a daily dose of 300900 mgincreases HDL cholesterol by 1530% in a dose-dependentfashion in healthy humans [181]. Plasma CETP activityis lowered by 37% after several weeks of daily treatmentwith 900 mg of JTT-705 but CETP mass concentration isincreased, which could be owing to a diminished CETPclearance [181]. In humans, plasma PLTP activity is unaf-fected by JTT-705 administration, indicating that this agentdoes not crossreact with PLTP [181]. The isoavan deriv-ative, CGS 25159, increases HDL cholesterol and HDL particle size in hamsters [178]. Further data are neededto show its action in man. In rabbits, administration of antisense oligonucleotides against CETP targeted to liverinhibits CETP transcriptionally [182]. As a result, plasmaCETP activity and CETP concentration are decreased, andHDL cholesterol is increased [182]. This approach alsoreduces the aortic atherosclerotic lesion area after 16 weekson a cholesterol enriched diet [182].
Taken together, the above-mentioned studies show thatthe effects of statins as well as brates on the cholesterylester transfer process are modest. Therefore, it will be of great clinical interest to combine these drugs with specicCETP inhibitors to reduce plasma cholesteryl ester transferand to raise HDL more profoundly. Indeed, clinical trials
with CETP inhibitors using surrogate end-points such asintima media thickness will soon be started. We propose thatdyslipidaemia as occurring in insulin resistance and type 2diabetes mellitus will become an important target for CETPinhibitor therapy.
Conclusions and future research
HDL cholesterol is decreased whereas HDL subfractionlevels and HDL remodelling are altered in insulin resistanceand type 2 diabetes mellitus in conjunction with highplasma triglycerides. These abnormalities are likely to beexplained at least in part by a low postheparin plasma LPL/HL ratio and by an increased CETP-mediated plasmacholesteryl ester transfer, a process that provides a meta-bolic intermediate between low HDL cholesterol and highplasma triglycerides. Elevated plasma PLTP activity in asso-ciation with high plasma triglycerides and obesity will affectHDL remodelling as well, including enhanced pre -HDL formation.
High-density lipoprotein plays a pivotal role in the anti-atherogenic RCT pathway, whereby cholesterol is trans-ported from peripheral cells to the liver for metabolism andsubsequent biliary excretion. Much has to be discernedabout the exact defects and perhaps compensatory mecha-nisms that are operative in this pathway in insulin resistanceand type 2 diabetes mellitus. Efux of cholesterol fromperipheral cells to extracellular acceptors is considered torepresent the rst step of RCT. In insulin resistance the abil-ity of plasma to promote cellular cholesterol efux may bemaintained. It is uncertain whether insulin resistance leads
to cellular abnormalities that affect cholesterol removal. Inthe diabetic state, it is likely that cellular cholesterol efuxis impaired as a result of changes in HDL subfraction levelsas well as of cell-related defects. As yet, data with respectto abnormalities in the uptake of HDL-derived cholesterolby the liver (both directly and via CETP-mediated transferto apo B-containing lipoproteins) and subsequent hepaticmetabolism and biliary excretion in insulin resistance andtype 2 diabetes mellitus are far from complete. Therefore, theextent to which these steps in RCT are abnormal in thesecommon disorders is uncertain at present, and much researchconcerning hepatic metabolism of HDL-derived cholesterolas well as with respect to HDL dynamics in vivo is needed.
One promising new pharmacological approach to treatinsulin resistance-associated and diabetes-associateddyslipidaemia will be the administration of specic CETPinhibitors that have been recently demonstrated to raise HDL cholesterol to a relevant extent in normolipidaemic humans,and to retard atherosclerosis development experimentally.
Acknowledgement
The valuable comments of Dr Arie van Tol are highlyappreciated.
8/13/2019 HDLdiabetes.pdf
14/19
1064 S. E. Borggreve et al.
2003 Blackwell Publishing Ltd, European Journal of Clinical Investigation, 33 , 10511069
References
1 Kannel WB, Castelli WP, Gordon T, McNamara PM. Serumcholesterol, lipoproteins, and the r isk of coronary heartdisease. The Framingham Study. Ann Intern Med 1971; 74 :1 12.
2 Barr DP, Russ EM, Eder HA. Protein-lipid relationship inhuman plasma in atherosclerosis and related conditions. Am
J Med 1951; 11 :48093.3 Miller GJ, Miller NE. Plasma-high-density-lipoprotein
concentration and development of ischaemic heart-disease.Lancet 1975; 1 :169.
4 Assmann G, Schulte H, von Eckardstein A, Huang Y. Highdensity lipoprotein cholesterol as a predictor of coronary heartdisease. The PROCAM experience and pathophysiologicalimplication for reverse cholesterol transport. Atherosclerosis 1996; 124 :S11S20.
5 Criqui MH, Heiss G, Cohn G, Cowan LD, Suchindran CM,Bangdiwala S et al. Plasma triglyceride level andmortality from coronary heart disease. N Engl J Med 1993; 328 :12205.
6 DeFronzo RA, Ferrannini E. Insulin resistance: amultifaceted syndrome responsible for NIDDM, obesity,hypertension, dyslipidemia, and atheroscleroticcardiovascular disease. Diabetes Care 1991; 14 :17394.
7 Reaven GM. Banting Lecture. role of insulin resistance inhuman disease. Diabetes 1988; 37 :1595607.
8 Haffner SM, Miettinen H. Insulin resistance implications fortype II diabetes mellitus and coronary heart disease. Am J Med 1997; 103 :15262.
9 Ferrannini E, Buzzigoli G, Bonadonna R, Giorico MA,Oleggini M, Graziadei L et al. Insulin resistance in essentialhypertension. N Engl J Med 1987; 317 :3507.
10 Juhan-Vague I, Alessi MC, Vague P. Increased plasmaplasminogen activator inhibitor-1 levels. a possible linkbetween insulin resistance and atherothrombosis. Diabetologia 1991; 34 :45762.
11 Riemens SC, van Tol A, Stulp BK, Dullaart RPF. Inuenceof insulin sensitivity and the TaqIB cholesteryl ester transferprotein gene polymorphism on plasma lecithin: cholesterolacyltransferase and lipid transfer protein activities and theirresponse to hyperinsulinemia in non-diabetic men. J Lipid Res 1999; 40 :146774.
12 Lehto S, Rnnemaa T, Haffner SM, Pyrl K, Kallia V,Laakso M. Dyslipidemia and hyperglycemia predict coronaryheart disease events in middle-age patients with NIDDM.Diabetes 1997; 46 :13549.
13 Fielding CJ, Fielding PE. Molecular physiology of reversecholesterol transport. J Lipid Res 1995; 36 :21128.
14 Rothblat GH, Llera-Moya M de la, Atger V, Kellner-WeibelG, Williams DL, Phillips MC. Cell cholesterol efux:integration of old and new observations provides new insights.
J Lipid Res 1999; 40 :78196.15 Watts GF, Playford DA. Dyslipoproteinaemia and
hyperoxidative stress in the pathogenesis of endothelialdysfunction in non-insulin dependent diabetes mellitus: anhypothesis. Atherosclerosis 1998; 141 :1730.
16 Bonnefont-Rousselot D, Thrond P, Beaudeux JL, Peynet J,LeGrand A, Delattre J. High density lippoproteins (HDL)and the oxidative hypothesis of atherosclerosis. Clin Chem Lab
Med 1999; 37 :93948.17 Navab M, Imes SS, Hama SY, Hough GP, Ross LA, Bork
RW et al. Monocyte transmigration induced by modicationof low density lipoprotein in cocultures of human aortic wall
cells is due to induction of monocyte chemotactic protein 1synthesis and is abolished by high density lipoprotein. J ClinInvest 1991; 88 :203946.
18 Eisenberg S. High density lipoprotein metabolism. J Lipid Res 1984; 25 :101758.
19 Eckardstein A, Nofer JR, Assmann G. High densitylipoproteins and arter iosclerosis. Role of cholesterol efux and
reverse cholesterol transport. Arterioscler Thromb Vasc Biol 2001; 21 :1327.
20 Tailleux A, Duriez P, Fruchart JC, Clavey V. ApolipoproteinA-II, HDL metabolism and atherosclerosis. Atherosclerosis 2002; 164 :113.
21 Nofer JR, Kehrel B, Fobker M, Levkau B, Assmann G,von Eckardstein A et al. HDL and arteriosclerosis: beyondreverse cholesterol transport. Atherosclerosis 2002; 161 :116.
22 Preiss-Landl K, Zimmermann R, Hmmerle G, Zechner R.Lipoprotein lipase. the regulation of tissue specic expressionand its role in lipid and energy metabolism. Curr Opin Lipidol 2002; 13 :47181.
23 Panarotto D, Rmillard P, Bouffard L, Maheux P. Insulinresistance affects the regulation of lipoprotein lipase in thepostprandial period and in an adipose tissue-specic manner.Eur J Clin Invest 2002; 32 :8492.
24 Jin W, Marchadier D, Rader DJ. Lipases and HDLmetabolism. Trends Endocrinol Metab 2002; 13 :1748.
25 Kuivenhoven JA, Groenemeyer BE, Boer JMA, Reymer PWA,Berghuis R, Bruin T et al. Ser447stop mutation in lipoproteinlipase is associated with elevated HDL cholesterol levels innormolipidemic males. Arterioscler Thromb Vasc Biol 1997; 17 :5959.
26 Perret B, Mabile L, Martinez L, Terc F, Barbaras R,Collet X. Hepatic lipase: structure/function relationship,synthesis and regulation. J Lipid Res 2002; 43 :11639.
27 Rye KA, Clay MA, Barter PJ. Remodelling of high densitylipoproteins by plasma factors. Atherosclerosis 1999; 145 :227 38.
28 Blanco-Vaca F, Escol-Gil JC, Martn-Campos JM, Julve J.Role of apo A-II in lipid metabolism and atherosclerosis:advances in the study of an enigmatic protein. J Lipid Res 2001; 42 :172739.
29 Hirata K, Dichek HL, Ciof JA, Choi SY, Leeper NJ,Quintana L et al. Cloning of a unique lipase from endothelialcells extends the lipase gene family. J Biol Chem 1999; 274 :141705.
30 Ishida T, Choi S, Kundu RK, Hirata K, Rubin EM,Cooper AD et al. Endothelial lipase is a major determinantof HDL level. J Clin Invest 2003; 111 :34755.
31 Jaye M, Lynch KJ, Krawiec J, Marchadier D, Maugeais C,Doan K et al. A novel endothelial-derived lipase thatmodulates HDL metabolism. Nature Med 1999; 21 :4248.
32 Kuivenhoven JA, Pritchard H, Hill J, Frohlich J, Assmann G,Kastelein J. The molecular pathology of lecithin: cholesterolacyltransferase (LCAT) deciency syndromes. J Lipid Res 1997; 38 :191205.
33 Mowri HO, Patsch JR, Ritsch A, Fger B, Brown S, PatschW. High density lipoproteins with differing apolipoproteins.relationships to postprandial lipemia, cholesteryl ester lipase,hepatic lipase, and lecithin: cholesterol acyltransferase. J LipidRes 1994; 35 :291300.
34 Murakami T, Michelagnoli S, Longhi R, Gianfrancheschi G,Pazzucconi F, Calabresi L et al. Triglycerides are majordeterminants of cholesterol esterication/transfer and HDLremodeling in human plasma. Arterioscler Thromb Vasc Biol 1995; 15 :181928.
8/13/2019 HDLdiabetes.pdf
15/19
HDL metabolism and reverse cholesterol transport in insulin resistance and type 2 diabetes mellitus 1065
2003 Blackwell Publishing Ltd, European Journal of Clinical Investigation, 33 , 10511069
35 Dullaart RPF, Riemens SC, Scheek LM, van Tol A. Insulindecreases plasma cholesteryl ester transport but notcholesterol esterication in healthy subjects as well as innormotriglyceridemic patients type 2 diabetes. Eur J ClinInvest 1999; 29 :66371.
36 Pastier D, Dugu S, Boisfer E, Atger V, Quang Tran N,van Tol A et al. Apolipoprotein A-II/A-I is a key determinant
in vivo of HDL concentration and formation of pre - HDLcontaining apolipoprotein A-II. Biochemistry 2001; 40 :12243 53.
37 Riemens S, van Tol A, Sluiter W, Dullaart R. Elevated plasmacholesteryl ester transfer in NIDDM. Relationships withapolipoprotein B-containing lipoproteins and phospholipidtransfer protein. Atherosclerosis 1998; 140 :719.
38 Barter PJ, Rye KA. Cholesteryl ester transfer protein, highdensity lipoprotein and arterial disease. Curr Opin Lipidol 2001; 12 :37782.
39 Dullaart RPF, Groener JEM, Erkelens DW. Cholesteryl estertransfer between lipoproteins. Diab Nutr Metab 1991; 14 :329 43.
40 Tall AR. Plasma cholesteryl ester transfer protein. J Lipid Res 1993; 34 :125574.
41 Karpe F. Postprandial lipoprotein metabolism andatherosclerosis. J Intern Med 1999; 246 :34155.
42 Lagrost L, Gambert P, Lallemant C. Combined effect of lipidtransfers and lipases on gradient gel patterns of human plasmaLDL. Arterioscler Thromb 1994; 14 :132736.
43 Mann CJ, Yen FT, Grant AM, Bihain BE. Mechanism ofplasma cholesteryl ester transfer in hypertriglyceridemia. JClin Invest 1991; 88 :205966.
44 Eisenberg S, Gavish D, Oschry Y, Fainaru M, Deckelbaum R.Abnormalities in very low, low and high density lipoproteinsin hypertriglyceridemia. Reversal toward normal withbezabrate treatment. J Clin Invest 1984; 74 :47082.
45 Eisenberg S. Preferential enrichment of large-sized very lowdensity lipoprotein with transferred cholesteryl esters. J LipidRes 1985; 26 :48794.
46 Tall AR, Sammett D, Vita GM, Deckelbaum R, OlivecronaT. Lipoprotein lipase enhances the cholesteryl ester transferprotein-mediated transfer of cholesteryl esters from highdensity lipoproteins to very low density lipoproteins. J BiolChem 1984; 259 :958794.
47 Ahnadi CE, Masmoudi T, Berthezne F, Ponsin G.Decreased ability of high density lipoproteins to transfercholesterol esters in non-insulin-dependent diabetes mellitus.Eur J Clin Invest 1993; 23 :45965.
48 Hannuksela ML, Marcel YL, Kesaniemi YA, Savolainen MJ.Reduction in the concentration and activity of plasmacholesteryl ester transfer protein by alcohol. J Lipid Res 1992; 33 :73744.
49 Venrooij FV, Stolk RP, Banga JD, Sijmonsma TP, van Tol A,Erkelens DW et al. Common cholesteryl ester transfer proteingene polymorphisms and the effect of atorvastatin therapy intype 2 diabetes. Diab Care 2003; 26 :121623.
50 Vries R, van Gent T, Borggreve SE, Ito M, Sluiter WJ,Dallinga-Thie GM et al. Diabetes mellitus is associated withdifferential effects on plasma cholesteryl ester transfer proteinand phospholipid transfer protein activities andconcentrations. Eur J Clin Invest 2003; 33 :401 (Abstract).
51 Wang X, Driscoll DM, Morton RE. Molecular cloning andexpression of lipid transfer inhibitor protein reveals its identitywith apolipoprotein F. J Biol Chem 1999; 274 :181420.
52 Morton RE. Cholesteryl ester transfer protein and its plasmaregulator: lipid transfer inhibitor protein. Curr Opin Lipidol 1999; 10 :3217.
53 Gautier T, Pais de Barros JP, Athias A, Gambert P, Aunis D,Metz-Boutigue MH et al. Human apolipoprotein C-Iaccounts for the ability of plasma high density lipoproteins toinhibit the cholesteryl ester transfer protein activity. J BiolChem 2000; 275 :375049.
54 Hirano K, Yamashita S, Nakajima N, Arai T, Maruyama T,Yoshida Y et al. Genetic cholesteryl ester transfer protein
deciency is extremely frequent in the Omagari area of Japan.Marked hyperalphalipoproteinemia caused by CETP genemutation is not associated with longevity. Arterioscler ThrombVasc Biol 1997; 17 :10539.
55 Zhang Z, Yamashita S, Hirano K, Nakagawa-Toyama A,Nishida M, Sakai N et al. Expression of cholesteryl estertransfer protein in human atherosclerotic lesions and itsimplication in reverse cholesterol transport. Atherosclerosis 2001; 159 :6775.
56 Zhong S, Sharp DS, Grove JS, Bruce C, Yano K, Curb JDet al. Increased coronary heart disease in Japanese-Americanmen with mutation in the cholesteryl ester transfer proteingene despite increased HDL levels. J Clin Invest 1996; 97 :291723.
57 Cuchel M, Wolfe ML, deLemos AS, Rader DJ. The frequencyof the cholesteryl ester transfer protein-TaqI B2 allele is lowerin African Americans than in Caucasians. Atherosclerosis 2002; 163 :16974.
58 Boekholdt SM, Thompson JF. Natural genetic variation as atool in understanding the role of CETP in lipid levels anddisease. J Lipid Res 2003; 44 :108093.
59 Talmud PJ, Edwards KL, Turner CM, Newman B, Palmen JM,Humphries SE et al. Linkage of the cholesteryl ester transferprotein (CETP) gene tot LDL particle size. Use of a noveltetranucleotide repeat within the CETP promoter. Circulation 2000; 101 :24616.
60 Dachet C, Poirier O, Cambien F, Chapman MJ, Rouis M.New functional promoter polymorphism, CETP/-629, incholesteryl ester transfer protein (CETP) gene related toCETP mass and high density lipoprotein cholesterol levels.role of Sp1/Sp3 in transcriptional regulation. ArteriosclerThromb Vasc Biol 2000; 20 :50715.
61 Goto A, Sasai K, Suzuki S, Fukutomi T, Ito S, Matsushita Tet al. Cholesterol ester transfer protein and atherosclerosis in
Japanese subjects: a study based on coronary angiography. Atherosclerosis 2001; 159 :15363.
62 Ordovas JM, Cupples A, Corella D, Otvos JD, Osgood D,Martinez A et al. Association of cholesteryl ester transferprotein-TaqIB polymorphism with variations in lipoproteinsubclasses and coronary heart disease risk. The FraminghamStudy. Arterioscler Thromb Vasc Biol 2000; 20 :13239.
63 Dullaart RPF, Hoogenberg K, Riemens SC, Groener JE,van Tol A, Sluiter WJ et al. Cholesteryl ester transfer proteingene polymorphism is a determinant of HDL cholesterol andof the lipoprotein response to a lipid-lowering diet in type 1diabetes. Diabetes 1997; 46 :20827.
64 Hannuksela ML, Liinamaa MJ, Kesaniemi YA, Savolainen MJ.Relation of polymorphisms in the cholesteryl ester transferprotein gene to transfer protein activity and plasmalipoprotein levels in alcohol drinkers. Atherosclerosis 1994; 110 :3544.
65 Kauma H, Savolainen MJ, Heikkila R, Rantala AO, Lilja M,Reunanen A et al. Sex difference in the regulation of plasmahigh density lipoprotein cholesterol by genetic andenvironmental factors. Hum Genet 1996; 97 :15662.
66 Fumeron F, Betoulle D, Luc G, Behague I, Ricard S,Poirier O et al. Alcohol intake modulates the effect of apolymorphism of the cholesteryl ester transfer protein gene
8/13/2019 HDLdiabetes.pdf
16/19
1066 S. E. Borggreve et al.
2003 Blackwell Publishing Ltd, European Journal of Clinical Investigation, 33 , 10511069
on plasma high density lipoprotein and the risk of myocardialinfarction. J Clin Invest 1995; 96 :166471.
67 Agerholm-Larsen B, Nordestgaard BG, Steffensen R, JensenG, Tybjaerg-Hansen A. Elevated HDL cholesterol is a riskfactor for ischemic heart disease in white women when causedby a common mutation in the cholesteryl ester transfer proteingene. Circulation 2000; 101 :190712.
68 Agerholm-Larsen B, Tybjaerg-Hansen A, Schnohr P,Steffensen R, Nordestgaard BG. Common cholesteryl estertransfer protein mutations, decreased HDL cholesterol, andpossible decreased risk of ischemic heart disease. TheCopenhagen City Heart Study. Circulation 2000; 102 :2197 203.
69 Day JR, Albers JJ, Lofton-Day CE, Gilbert TL, Ching AFT,Grant FJ et al. Complete cDNA encoding humanphospholipid transfer protein from human endothelial cells.
J Biol Chem 1994; 269 :938891.70 Nishida HI, Nishida T. Phospholipid transfer protein
mediates transfer of not only phosphatidylcholine but alsocholesterol vesicles to high density lipoproteins. J Biol Chem 1997; 272 :695964.
71 Jauhiainen M, Metso J, Pahlman R, Blomqvist S, van Tol A,Ehnholm C. Human plasma phospholipid transfer proteincauses high density lipoprotein conversion. J Biol Chem 1993; 268 :40326.
72 Tu AY, Nishida HI, Nishida T. High density lipoproteinconversion mediated by human plasma phospholipid transferprotein. J Biol Chem 1993; 268 :23098105.
73 Castro GR, Fielding CJ. Early incorporation of cell-derivedcholesterol into pre- -migrating high-density lipoprotein.Biochemistry 1988; 27 :259.
74 Eckardstein A, Jauhiainen M, Huang Y, Metso J, Langer C,Pussinen P et al. Phospholipid transfer protein mediatedconversion of high density lipoproteins generates pre 1-HDL.Biochim Biophys Acta 1996; 1301 :25562.
75 Huuskonen J, Ekstrm M, Tahvanainen E, Vainio A,Metso J, Pussinen P et al. Quantication of human plasmaphospholipid transfer protein (PLTP): relationship betweenPLTP mass and phospholipid transfer activity. Atherosclerosis 2000; 151 :45161.
76 Krkkinen M, Oka T, Olkkonen VM, Metso J, Hattori H, Jauhiainen M et al. Isolation and par tial characterizationof the inactive and active forms of human plasmaphospholipid transfer protein (PLTP). J Biol Chem 2002; 277 :154138.
77 Taskinen MR. Diabetic dyslipidaemia: from basic research toclinical practice. Diabetologia 2003; 46 :73349.
78 Roden M, Price TB, Perseghin G, Petersen KF, Rothman DL,Cline GW et al. Mechanism of free fatty acid-induced insulinresistance in humans. J Clin Invest 1996; 97 :285965.
79 Howard BV, Howard WJ. Dyslipidemia in non-insulin-dependent diabetes mellitus. Endocrine Rev 1994; 15 :26374.
80 Taskinen MR. Hyperlipidaemia in diabetes. Ballires ClinEndocrinol Metabolism 1990; 4:74375.
81 Syvnne M, Hilden H, Taskinen MR. Abnormal metabolismof postprandial lipoproteins in patients with non-insulin-dependent diabetes mellitus is not related to coronary ar terydisease. J Lipid Res 1994; 35 :1526.
82 Riemens SC, van Tol A, Scheek LM, Dullaart RPF. Plasmacholesteryl ester transfer and hepatic lipase activity are relatedto high-density lipoprotein cholesterol in association withinsulin resistance in type 2 diabetic and non-diabetic subjects.Scand J Clin Lab Invest 2001; 61 :110.
83 Laakso M, Voutilainen E, Sarlund H, Aro A, Pyrl K,Perret B. Serum Lipids and lipoproteins in middle-aged
non-insulin-dependent diabetics. Atherosclerosis 1985; 56 :271 81.
84 Riemens SC, van Tol A, Sluiter WJ, Dullaart RPF. Plasmaphospholipid transfer protein activity is related to insulinresistance: impaired acute lowering by insulin in obeseNIDDM patients. Diabetologia 1998; 41 :92934.
85 Berthezne F. Non-insulin dependent diabetes and reverse
cholesterol transport. Atherosclerosis 1996; 124 (Suppl.):S39 S42.
86 Brites FD, Cavallero E, Geitere C de, Nicolaew N, Jacotot B,Rosseneu M et al. Abnormal capacity to induce cholesterolefux and a new LpA-I pre- particle in type 2 diabeticpatients. Clin Chim Acta 1999; 279 :114.
87 OBrien T, Nguyen TT, Hallaway BJ, Hodge D, Bailey K,Kottke BA. HDL subparticles and coronary artery disease inNIDDM. Atherosclerosis 1996; 121 :28591.
88 Ishida BY, Frolich J, Fielding CJ. Prebeta-migrating highdensity lipoprotein: quantitation in normal andhyperlipidemic plasma by solid phase radioimmunoassayfollowing electrophoretic transfer. J Lipid Res 1987; 28 :778 86.
89 Dullaart RPF, van Tol A. Role of phospholipid transfer proteinand prebeta-high density lipoproteins in maintainingcholesterol efux from Fu5AH cells to plasma frominsulin-resistant subjects. Scand J Clin Lab Invest 2001; 61 :69 74.
90 Dullaart RPF, van Tol A. Twenty four hour insulin infusionimpairs the ability of plasma from healthy subjects and type2 diabetic patients to promote cellular cholesterol efux.
Atherosclerosis 2001; 157 :4956.91 Knudsen P, Eriksson J, Lahdenper S, Kahri J, Groop L,
Taskinen MR et al. Changes of lipolytic enzymes cluster withinsulin resistance syndrome. Diabetologia 1995; 38 :34450.
92 Pykalisto OJ, Smith PH, Brunzell JD. Determinants of humanadipose tissue lipoprotein lipase. Effect of diabetes and obesityon basal- and diet-induced activity. J Clin Invest 1975; 56 :110870.
93 Pollare T, Vessby B, Lithell H. Lipoprotein lipase activity inskeletal muscle is related to insulin sensitivity. ArteriosclerThromb 1991; 11 :1192203.
94 Riemens SC, van Tol A, Sluiter WJ, Dullaart RPF. Acute andchronic effects of a 24-hour intravenous triglyceride emulsionchallenge on plasma lecithin: cholesterol acyltransferase,phospholipid transfer protein, and cholesteryl ester transferprotein activities. J Lipid Res 1999; 40 :145966.
95 Baynes C, Henderson AD, Anyaoku V, Richmond W,Hughes CL, Johnston DG et al. The role of insulininsensitivity and hepatic lipase in the dyslipidaemia oftype 2 diabetes. Diabet Med 1991; 8:5606.
96 Stokke KT, Enger SC. Plasma HDL cholesterol and the invitro esterication of cholesterol. Scand J Clin Lab Invest 1979; 39 :597600.
97 Channon KM, Clegg RJ, Bhatnagar D, Ishola M, Arrol S,Durrington PN. Investigation of lipid transfer in humanserum leading to the development of an isotopic method forthe determination of endogenous cholesterol estericationand transfer. Atherosclerosis 1990; 80 :21726.
98 Floren CH, Chen CH, Franzen J, Albers JJ. Lecithin:cholesterol acyltransferase in liver disease. Scand J Clin LabInvest 1987; 47 :6137.
99 Albers JJ, Adolphson JL, Chen CH. Radioimmunoassay ofhuman plasma lecithin-cholesterol acyltransferase. J ClinInvest 1981; 67 :1418.
100 Bhatnagar D, Durrington PN, Kumar S, Mackness MI,Boulton AJM. Plasma lipoprotein composition and
8/13/2019 HDLdiabetes.pdf
17/19
HDL metabolism and reverse cholesterol transport in insulin resistance and type 2 diabetes mellitus 1067
2003 Blackwell Publishing Ltd, European Journal of Clinical Investigation, 33 , 10511069
cholesteryl ester transfer from high density to very low densitylipoproteins in patients with non-insulin dependent diabetesmellitus. Diabet Med 1996; 13 :13944.
101 Durlach V, Attia N, Zahouani A, Leutenegger M,Girard-Globa A. Postprandial cholesteryl ester transfer andhigh density lipoprotein composition in normotriglyceridemicnon-insulin-dependent diabetic patients. Atherosclerosis
1996; 120 :15565.102 Jones RJ, Owens D, Brennan C, Collins PB, Johnson AH,
Tomkin GH. Increased esterication of cholesterol andtransfer of cholesteryl ester to apo B-containing lipoproteinsin Type 2 diabetes. relationship to serum lipoproteins A-I andA-II. Atherosclerosis 1996; 119 :1517.
103 Groener JE, Pelton RW, Kostner GM. Improved estimationof cholesteryl ester transfer/exchange activity in serum orplasma. Clin Chem 1986; 32 :2836.
104 Lottenberg SA, Lottenberg AMP, Nunes VS, McPherson R,Quintao ECR. Plasma cholesteryl ester transfer proteinconcentration, high-density lipoprotein cholesterolesterication and transfer rates to lighter density lipoproteinsin the fasting state and after a test meal are similar intype II diabetics and normal controls. Atherosclerosis 1996; 127 :8190.
105 Gurin M, le Goff W, Lassel TS, van Tol A, Steiner G,Chapman MJ. Proatherogenic role of elevated CE transferfrom HDL to VLDL1 and dense LDL in type 2 diabetes.Impact of the degree of triglyceridemia. Arterioscler ThrombVasc Biol 2001; 21 :2828.
106 Bagdade JD, Lane JT, Subbaiah PV, Otto ME, Ritter MC.Accelerated cholesteryl ester transfer in noninsulin-dependentdiabetes mellitus. Atherosclerosis 1993; 104 :6977.
107 Arii K, Suehiro T, Yamamoto M, Ito H, Hashimoto K.Suppression of plasma cholesteryl ester transfer proteinactivity in acute hyperinsulinemia and effect of plasmanonesteried fatty acid. Metabolism 1997; 46 :116670.
108 Riemens SC