Embed Size (px)
Citation preview

Unidad del Dolor José Luis Aguilar
Jefe Servicio Anestesiología, Reanimación y Unidad del Dolor

Tratamiento del Dolor Lumbar
• Procedimientos farmacológicos
• Procedimientos invasivos: – predominio lumbalgia – predominio radiculalgia
• Procedimientos No farmacológicos:
– rehabilitación - autocuidados – TENS – Acupuntura – terapias cognitivo-conductuales, relajación – terapia ocupacional – apoyo social

• El nivel de evidencia da una idea de la solidez del fundamento científico de una aseveración
• Depende del número de estudios, calidad
y consistencia de sus resultados

Level of Evidence
Benefit due to effectiveness of treatment GREATER than risk and burden of potential complications, value 1 is given
Value 2 is given when benefit of effect is
closely balanced with the risk and burden of possible side effects

Level of evidence
• A (highest) (Various high quality RCTs) • B (evidence from large observational
studies or RCTs with methodological limitations)
• C (observational studies or case series) • 0 = only case reports positive outcome + negative outcome or – … outcome ±

Objetivos del tratamiento
Aliviar el dolor
Minimizar la incapacidad funcional
Reinserción laboral Retardar la progresión del proceso

Epidemiología y lumbalgia
• Cronicidad 10 - 40%
• > 12 semanas recuperación lenta e incierta:
– inhabilitación > 6 meses… <50% reincorporación
laboral
– inhabilitación 2 años… ~ 0% reincorporación laboral

Epidemiología y etiología
Dolor lumbar específico 15%
tratamiento etiológico
Dolor lumbar inespecífico 85%
Sin relación: grado de afectación exploración física estudios de imagen neurofisiológicos laboratorio
“Bravo et al . Rev Soc Esp Dolor 2001”

AFERENTE PRIMARIA RAIZ DORSAL
TRANSMISIÓN
VÍAS ASCENDENTES
MODULACIÓN
VÍAS DESCENDENTES
TRANSDUCCIÓN
PERCEPCIÓN
Estímulo nociceptivo
Dolor lumbar específico

Lumbalgia crónica
Sensorial Afectivo
Modelo biopsicosocial Emocional
• Pain 2008. “Back Pain. An update review” IASP Syllabus Glasgow.
Sociolaboral

Lumbalgia y Cronificación
• Edad avanzada
• Sexo femenino
• EVA alto
• Clínica prolongada
• Episodios previos
• Radiculalgia
• Estatus socioeconómico deprimido
• Bajo nivel educacional • IMC elevado • Tabaquismo • Salud deteriorada • Sedentarismo • Insatisfacción laboral • Depresión • Variaciones anatómicas
espinales

Clasificación etiológica
• Mecánicas – Inespecíficas: sobrecarga funcional o
postural. – Alteraciones estructurales: hernia de disco,
estenosis de canal, espondilolisis-listesis…
• No mecánico – Inflamatorio: Espondilitis, artritis, EII…. – Neoplásico – Infeccioso: osteomielitis, discitis – Enfermedad de Paget
• Dolor lumbar referido
– Aneurisma de Aorta – Patología genitourinaria – Enfermedades digestivas – Coxalgia


Lumbalgia

Radiculalgia

Lumbalgia

Radiculalgia


Información Medidas Preventivas Educación sanitaria
AUTOCUIDADOS
Educación Sanitaria Medidas preventivas

Postlaminectomy syndrome 113,823 errors, $9,863 per error, $1.123 billion total. Shreve J, Van Den Bos J, Gray T, Halford M, Rustagi K, Ziemkiewicz E. The economic measurement of medical errors. Society of Actuaries. 2010. Milliman.

Unidad funcional
• Dos cuerpos vertebrales
• Un disco intervertebral
• Articulación zigoapofisaria
• Ligamentos y músculos
“Clinical Anatomy of the Lumbar Spine ands Sacrum”
Nikolai Bogduk 2005

Unidad funcional vs diagnóstico
• Cuerpo vertebral
• Disco intervertebral
• Articulación zigoapofisaria
• Ligamentos y músculos
Osteoporosis, espondilolistesis,
fracturas
Dolor discogénico
Síndrome facetario
Síndrome miofascial
“Clinical Anatomy of the Lumbar Spine ands Sacrum”
Nikolai Bogduk 2005

Origen miofascial
• Punto gatillo miofascial: – zona hiperirritable en un músculo esquelético. – asociada a un nódulo palpable e hipersensible. – localizado en una banda tensa.
• dolor local y referido • Músculos profundos:
– Piriforme – Cuadro lumbar – Iliopsoas

Síndrome Miofascial
• En el caso de la lumbalgia los músculos cuadrado lumbar, iliopsoas y piriforme pueden justificar lumbalgia con o si dolor irradiado.
• En estas ocasiones se habla de pseudociático (como en el caso del síndrome miofascial del músculo piriforme)



Inervación lumbar
Ramo posterior nervio raquídeo
– Medial:
• faceta del nivel e inferior
– Intermedia: • músculos y
aponeurosis – Lateral:
• cutánea
80% del dolor raquídeo



Inervación lumbar
Nervio sinovertebral de Luschka
• Cara posterior de cuerpos vertebrales
• Ligamento vertebral común posterior
• Anillo discal
Dolor protrusion discal
Dolor inestabilidad vertebral

”Baron R, Binder A. 2004 Orthopade. 2004;33(5):568-75 ”
Disco Fibra C
Fibra C Fibra A
Componente nociceptivo: Ramificación de las fibras C en el disco
Componente neuropático I: Lesión de una rama de la fibra C debida a compresión y a mediadores inflamatorios
Componente neuropático II: Compresión de la raíz nerviosa
Componente neuropático III: Lesión de la raíz nerviosa por mediadores inflamatorios
Sensibilización central

Dolor lumbar etiopatogenia
• Se han encontrado neoterminaciones nerviosas propioceptivas y nociceptivas en patologías degenerativas.
• Se han identificado neurotransmisores nociceptivos en membranas y cartílagos de articulaciones degeneradas: – Sust P, CGRP, Fosfolipasa A – Neuropéptido Y (implicaría la presencia de fibras
simpáticas eferentes) – PGs, IL1-β, IL6, TNF α



39% del Dolor Bajo de Espalda es por disrupción discal: 28% población alteraciones del disco SIN dolor
Schwarzer et al, 1995, Adams et al, 2000

Discos lumbares en cadáver Sección en plano medio sagital
Disco joven: varón 35 años Disco maduro: varón 47 años
Disrupción discal: varón 51 años Disrupción discal grave: varón 71 años.
Colapso de la altura discal . Prolapso discal inducido en laboratorio:
varón 40 años. Núcleo pulposo herniado por fisura radial del anillo posterior
“Churchill Livingstone; 2002.”

Dolor discogénico
Osteofitos Esclerosis platillo vertebral
Pérdida del hueso trabecular
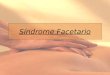
Afectación facetaria

• Hipertrofia / artrosis facetaria
• Ausencia signos neurológicos
– estenosis foraminal
• Dolor unilateral o bilateral
• Contractura muscular
Origen zigoapofisario

SINDROME FACETARIO LUMBAR

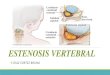
Estenosis de canal
•Degeneración discal •Degeneración e hipertrofia facetaria •Hipertrofia y calcificación de ligamento amarillo


Estenosis de canal
Estenosis en autopsias • 90–100% mayores de 64 años Estenosis en RMN • 80% mayores de 70 años
“Lumbar spinal stenosis in the elderly:an overview” Eur Spine J (2003) 12: S170–S175

Tratamiento del Dolor Lumbar….
• Procedimientos farmacológicos
• Procedimientos invasivos: – predominio lumbalgia – predominio radiculalgia
• Procedimientos No farmacológicos:
– rehabilitación - autocuidados – TENS – Acupuntura – terapias cognitivo-conductuales, relajación – terapia ocupacional – apoyo social

+ Paracetamol
Abordaje del Dolor
Paracetamol AINES
Codeína TRAMADOL
Opiáceos Potentes
1º Escalón 2º Escalón 3º Escalón
+ Coadyuvantes
Tratamiento invasivo: Bloqueos nervioso Opioides espinales Neuroestimulación Radiofrecuencia…
4º Escalón

Tratamiento del Dolor Crónico
• Procedimientos farmacológicos
• Procedimientos invasivos: – predominio lumbalgia – predominio radiculalgia
• Procedimientos No farmacológicos:
– rehabilitación - autocuidados – TENS – terapias cognitivo-conductuales, relajación – terapia ocupacional – apoyo social


Bloqueos espinales: epidurales interlaminares, transforaminales - caudales

Transforaminal

Voluminosa imagen de 18 mm de diámetro y aspecto líquido situada pegada a la articular izda de L4-L5, intra-canal (quiste sinovial?)



Infiltración o Radiofrecuencia ramo post. Faceta Lumbar (Artic. Zygapofisaria)

Radiofrecuencia Ramo medial n = 53 Dra. Raquel Peláez

RF GRD

Heavner et al • Effect of Radiofrequency on Thermocoagulation of Egg White. Pain Physician Vol. 9, No. 2, 2006
Basal 42ºC pRDF 60ºC pRDF 60-65ºC pRDF
65ºC pRDF 70ºC pRDF 80ºC cRDF

HSLL Unidad Dolor Radiofrecuencia GRD

Los pacientes sometidos a radiofrecuencia presentaron una disminución del dolor del 40% en el caso de una radiofrecuencia, y del 55% cuando se aplicaron dos radiofrecuencias. Teniendo en cuenta que la reducción del dolor ≥50 % es señal de una mejora del paciente, vemos que el dolor tiende a reducirse en mayor grado cuando se alarga el tiempo de radiofrecuencia

El 94,7% de los pacientes que tienen una disminución del dolor mayor del 50% consideran que el tratamiento es eficaz. Representa el 52,9% del total de pacientes con RF GRD Las variables están relacionadas (p<0.05).

Pearson Chi.Square. P>0.05. No significativo
Disminución de la medicación

CIRUGÍA FALLIDA DE ESPALDA

Cirugía Fallida de Espalda = CFE

• Dificultad micción • Incontinencia rectal o ↓ tono esfínter anal • Pérdida fuerza ee.ii., alteración marcha • Déficit neurológico progresivo • Hipoestesia en silla de montar
Sospecha síndrome de cola de caballo

Neuroestimulación

Neuromodulación farmacológica


Dr. Javier Mata Dr. Pere Valentí

“… el único dolor soportable, es el dolor..
ajeno …”

Gracias


•Población activa estabilizándose
•Cuarta edad sigue aumentando
•2050

¿Cómo empleamos la RF?

72
Estimulador de n. periférico • Estimulación sensitiva a 50 Hz
–Estimulación en contacto*: 0.25 v –Estimulación a 1 cm del nervio*: 2 v –NO EN EL N. NEUROPÁTICO
• Estimulación motora a 2 Hz –Mide proximidad a fibras motoras –Es segura a intensidad del DOBLE de la
sensitiva (*)Ford DJ, Pither C, Raj PP: Comparison of insulated and uninsulated needles for locating peripheral nerves with a peripheral nerve stimulator: Anesth Analg 63:925-928, 1884.

PRDF: A.-Efectos No térmicos
• Fuerzas dielectroforéticas en moléculas cargadas: stress, distorsión y movimiento que pueden ocurrir a nivel subcelular

PRDF: A.-Efectos No térmicos
• Electroporation: Alteración en las canales iónicos de las membranas celulares

“Evidencia de daño ultraestructural de axones nociceptores sensoriales tras la exposición a PRF”
Erdine S. “Ultrastructural changes in axons following exposure to pulsed radiofrequency fields”. Pain Practice, 9:6.2009.

Erdine S. “Ultrastructural changes in axons following exposure to pulsed radiofrequency fields”. Pain Practice, 9:6.2009.
“La PRF actúa principalmente sobre fibras A-delta y C” Daño mitocondrial: no regeneración tubular
Porcentaje de fibras de cada tipo dañadas y no dañadas con PRF

Placebo en Dolor = 33%
Coste de oportunidad

Gracias

Modelo biopsicosocial
• Epidemiología: – Lown et al 2007, Dagenais et al 2008
• Clase social: – Poleshuck et al 2008
• Factores psicológicos: – Jemella et al 2005
• Formación académica: – Johnson 2007
• Fisioterapia: – Frost et al 2004
Pain 2008. “Back Pain. An update review”

Objetivos
• Definición
• Epidemiología
• Clasificación temporal y etiológica
• Fisiopatología
• Algoritmos diagnóstico - terapéuticos
• Rol de pruebas de imagen
• Tratamiento farmacológico y no farmacológico

¿Qué es el DOLOR?
1. Dolor: El dolor es una experiencia sensorial y emocional desagradable, asociada a un daño tisular, real o potencial, o descrita en términos de dicho daño (Asociación Internacional para el Estudio del Dolor, IASP)
2. Dolor: “Sociopatía” … Sueño Ánimo Dolor Serotonina, Noradrenalina, Endorfinas…
Hambre


• BLOQUEOS DIAGNOSTICOS • SE ACEPTA QUE SON EL MÉTODO MÁS
FIABLE PARA EL DIAGNÓSTICO: • Bloqueo ramo medial del ramo dorsal del n.
raquídeo • Inyecciones intraarticulares…

• Tratamiento Multimodal • Iniciar con tratamiento no invasivo: • FARMACOLÓGICO • PSICOTERAPIA • TENS • REHABILITACION • MANIPULACION OSTEOPATICA • YOGA • Si fracaso terapéutico, indicar tratamiento
invasivo: • ramo medial ramo dorsal: bloqueos/
radiofrecuencia

• A comparison of conventional and pulsed radiofrequency denervationa in the treatment of chronic facet joint pain Clin J Pain 2007 Jul-Aug;23 (6): 524-9:
• Boswell. A systematic review of therapeutic facet joint interventions in chronic spinal pain. Pain Physician 2007;10:229-253
• Boswell. Systematic review of diagnostic utility of facet (zygapophysial) joint injections in chronic spinal pain: an update. Pain Physician 2007;10:213-228
• Cohen. Pathogenesis, diagnosis and treatment of lumbar zygapophysial (facet) joint pain.Anesthesiology 2007;106:591-614
• Manchikanti. Age-related prevalence of facet-joint involvement in chronic neck an low back pain. Pain Physician 2008;11:67-75
• Manchikanti. Influence of psychological variables on the diagnosis of facet joint involvement in chronic spinal pain. Pain Physician 2008; 11:145-160
• Wilde. Indicators of lumbar zygapophyseal joint pain: survey of an expert panel with the Delphi technique. Phys Ther 2007 Oct; 87(10):1348-61
• Gómez-Pombo A et al Tratamiento del Síndrome de Dolor Miofascial con Toxina Botulínica tipo A. Rev Soc Esp Dolor 13: 2006;2 :96 – 102

• Raj P. Botulinum Toxin in the treatment of pain Associated with musculoskeletal Hyperactivity. Current Review of pain 1997; 1: 1403-416.
• Wheeler AH et al. Myofascial pain disorders: therapy to therapy. Drugs 2004; 64(1):45-62.
• Abram SE: Does the botulinum toxin have a role in the management of myofascial pain? Anesthesiology 2005;103(2):223-4
• Freund B et al. Temporal relationship of muscle weakness and pain reduction in subjects treatment with botulinum toxin A. J Pain 2003; 4 (3); 159-65
• Jabbari et al. Treatment of refractory chronic low back pain with botulinum neurotoxin A: an open label pilot study. Pain Med 2006;7:260-4.
• Ney JP et al. Treatment of chronic low back pain with successive injections of botulinum toxin a over 6 months; a prospective trial of 60 patients. Clin J Pain 2006;22(4):363-9

• Lang AM. Botulinum toxin type B in piriformis syndrome. Am J Phys Med Rehabil. 2004;83(3):198-202
• De Andres et al. Use of botulinum toxin in the treatment of chronic myofascial pain. Clin J Pain 2003;19(4):269-75
• Foster L et al. Botulinum toxin A and chronic low back pain: a randomized, double blind study. Neurology 2001;56(10):1290-3.
• Difazio M et al. A focused review of the use of botulinum toxins for low back pain. Clin J Pain 2002;18(6 suppl):S155-162

• Edad presentación: < 20 años ó >55 años • Síndrome tóxico o mal estado general • Limitación severa y persistente flexión lumbar • Dolor intenso, progresivo • Dolor de tipo no mecánico, no mejora con reposo • Dolor torácico o cuadro vegetativo acompañante • Antecedente traumático • ADVP, alcoholismo • Deterioro neurológico • Tratamiento crónico con corticoides • Antecedentes de neoplasia • Inmunosupresión (VIH) • Sospecha de síndrome de cola de caballo

Nervio raquídeo
a) Ramo ventral (formará los plexos lumbar y sacro) b) Ramo dorsal
– Rama medial: FACETAS, MULTIFIDUS, MÚSCULO Y LIGAMENTO
INTERESPINOSO, PERIOSTIO ARCO NEURAL – Ramo medio: LONGISSIMUS – Rama lateral: CUTÁNEO SENSITIVO: MÚSCULO ILIOCOSTALIS,
FASCIA TORACOLUMBAR, PIEL LUMBAR BAJA, SACROILIACA Y NALGA
c) N. sinuvertebral recurrente: cara posterior cuerpo vertebral, ligamento vertebral común posterior, annulus fibrosus
d) Ramos comunicantes: anastomosis con tronco simpático.

Dolor discogénico
• 39% del DBE disrupción discal: – 28% población alteraciones del disco SIN dolor
• Lesión del platillo vertebral degeneración
discal
• Menor aporte vascular al anillo fibroso y núcleo pulposo
• Degeneración discal afectación de la unidad funcional
“Schwarzer et al, 1995, Adams et al, 2000”

Inervación artic. zigapofisaria
• Cada art. facetaria recibe doble inervación: • ramo medial del ramo dorsal del n. raquídeo
del mismo nivel • ramo medial del ramo dorsal del n. raquídeo
del nivel inmediatamente superior • Algunos autores proponen que además recibe
inervación de : • ramo medial art. inferior • gg raíz dorsal • gg simpáticos paravertebrales





Analgesia multimodal o balanceada
• Actuar en las distintas “estaciones” por las que pasa
el estímulo nociceptivo – periférico – medular – talámico-límbico – cortical
con diferentes fármacos y técnicas
• Combinando fármacos – AINEs + analgésicos menores + opiáceos + coadyuvantes
» efecto sinérgico » menos dosis, menos efectos secundarios

Intraarticulares Bloqueos RM RF RM
Cervical LIMITADA MODERADA MODERADA
Torácico MODERADA ¿?
Lumbar MODERADA MODERADA MODERADA
Grados de evidencia
• CIRUGIA • No se ha encontrado relación entre la respuesta a bloqueos
diagnósticos y los resultados de la cirugía. Una razón de respuesta positiva a la artrodesis sería la rizotomía inadvertida/intencionada del ramo medial durante la colocación del material de osteosíntesis en pedículo.

Disc Radiofrequency Treatment
Lesion: P- RF 41º 60-90 sec.

Tratamientomédico
Aguda<6 semanas
RX PA-LATTratamiento
según RX
Subaguda6 semanasa 3 meses
Remitir RHB(Recaidas*)
RX PA-LATactual o
antigua<1a
Crónica*>3 meses
LUMBALGIAMECANICA
Analisis±RXRemitir aREUMA
LUMBALGIAINFLAMATORIA
Tratamientomédico
Sin deficitneurológico
RemitirCOT
preferente
RX PA-LatPosibilidad
RMN
Con déficitneurológico
<6 semanas
RemitirCOT
ordinaria
RX PA-LatPosibilidad
RMN
>6 semanas
RADICULOPATIA
RemitirCOT
ordinaria
RXPA-LAT
CLAUDICACIÓN
DOLOR LUMBAR




Red flags = signos de alarma
• < 20 años ó >55 años • Síndrome tóxico o MEG • Limitación severa y
persistente flexión lumbar
• Intenso, progresivo • No mecánico • No mejora con reposo • Sospecha síndrome de
cola de caballo
• Antecedente traumático • ADVP, alcoholismo • Deterioro neurológico • Antecedentes de
neoplasia • Inmunosupresión • Dolor torácico o cuadro
vegetativo acompañante
Estudio radiológico preferente Remisión hospitalaria

Definición IASP
Dolor bajo de espalda
• Dolor lumbar: – Espinosa T12- S1 – Bordes laterales mm. erector
espinae
• Dolor sacro: – Espinosa S1-unión sacrococcígea – Espinas ilíacas posteriores

Mixto


•Vértebra Lumbar
•Hernia discal
•Activación de nociceptores periféricos –causa del componente nociceptivo del
dolor1
•Compresión e inflamación de la raíz nerviosa–causa del componente neuropático
del dolor2
•1. Brisby H. J Bone Joint Surg Am 2006;88 (Suppl 2):68–71 2. Freynhagen R, Baron R. Curr Pain Headache Rep 2009;13:185–90
Dolor MIXTO Nociceptivo y neuropático: hernia discal

German Acupuncture Trials (GERAC) for Chronic Low Back Pain
Haake M, Müller HH, Schade-Brittinger C, Basler HD, Schäfer H, Maier C,Endres HG, Trampisch HJ, Molsberger A. Arch Intern Med. 2007;167(17):1892-1898
1162 patients 18 to 86 years (mean±SD age, 50±15 years) Randomized, Multicenter, Blinded, Parallel-Group Trial With 3 Groups
• Verum ACU (n=387) according to principles of TCM
• Sham ACU (n=387) consisting of superficial needling at nonacupuncture points
• Conventional therapy (n=388), a combination of drugs, physical therapy, and exercise
Primary outcome was response after 6 months
• 33% improvement • Better on 3 pain-related items on the CPGS • 12% improvement or better on the back-specific HFAQ
Dr. J. Mata

Dr. J. Mata
German Acupuncture Trials (GERAC) for Chronic Low Back Pain
Haake M, Müller HH, Schade-Brittinger C, Basler HD, Schäfer H, Maier C,Endres HG, Trampisch HJ, Molsberger A. Arch Intern Med. 2007;167(17):1892-1898
Results:
Response rate
• 47.6% in the verum ACU group • 44.2% in the sham ACU group • 27.4% in the conventional therapy group.
Differences among groups
• verum vs sham, 3.4% (95% c.i., −3.7% to 10.3%; P=.39) • verum vs conventional therapy, 20.2% (95% c.i., 13.4% to 26.7%; P<.001); • sham vs conventional therapy, 16.8% (95% c.i., 10.1% to 23.4%; P<.001)
Conclusions: Low back pain improved after ACU treatment for at least 6 months. Effectiveness of ACU,either verum or sham, was almost twice that of conventional therapy

Witt CM, Jena S, Selim D, et al. Pragmatic randomized trial evaluating the clinical and economic effectiveness of acupuncture for chronic low back pain. Am J Epidemiol 2006;164:487-496
Dr. J. Mata
A large trial in Germany, 3093 patients with chronic low back pain for a mean of 7 years Randomly assigned to receive either acupuncture or no acupuncture in addition to usual medical care. The primary end point was back function, as assessed with the use of the Hannover Functional Ability Questionnaire, which generates a score ranging from 0 to 100, with 100 representing perfect back function. At 3 months, the mean back-function score in the acupuncture group had increased from 61.8 to 74.5 (a mean increase of 12.1 points), and the mean score in the control group had increased from 63.3 to 65.1 (a mean increase of 2.7 points), for a difference in mean between-group improvement of 9.4 points (95% confidence interval, 8.3 to 10.5; P<0.001).

OBJECTIVES To evaluate the analgesic effect of ACU and sham ACU To assess the relationship between sham and ACU effect
METODOLOGY Searching to the end of 2007
Cochrane MEDLINE EMBASE Biological Abstracts PsycLIT
13 RCTs (n= 3025 (30 - 1039)
RESULTS
Statistically significant benefit for acupuncture over sham
Statistically significant benefit for sham ACU over no ACU
Significant statistical heterogeneity was
detected
CONCLUSIONS
A small analgesic effect of acupuncture was found
Acupuncture treatment for pain: systematic review of randomised clinical trials with acupuncture, placebo
acupuncture, and no acupuncture groups.
Madsen M V, Gotzsche P C, Hrobjartsson A BMJ 2009; 338(a3115)
Dr. J. Mata

OBJECTIVE To evaluate the effectiveness of ACU, sham ACU and usual care
METODOLOGY 638 adults (60% ♀)
70% back pain for ≥ 1 year Randomised
Individualised ACU Standardised ACU Sham acupuncture Usual care
10 treatments Assessments were made at 8, 26, and 52 weeks
RESULTS
No difference between individualised ACU, standardised ACU, or sham ACU. RMDQ scores fell from 11 to 6 for ACU of any sort sort by 52 weeks, compared with 7.9 for usual care. Use of medications (about 65% at baseline) fell to 47% with ACU, but remained at 59% with usual care. Cutting down on usual activities ≥ 7 days in the last month at 52 weeks was more common with usual care (18%) than with ACU More participants with usual care missed work or school for more than a day (16%) than with ACU (5%-10%).
A randomized trial comparing acupuncture, simulated acupuncture, and usual care for chronic low back pain. .
DC Cherkin et al Archives of Internal Medicine 2009 169: 858-866.
Dr. J. Mata
CONCLUSION: ACU is no better than sham for treating back pain

Meta-Analysis: Acupuncture for Low Back Pain
Dr. J. Mata

A randomised controlled trial of acupuncture care for persistent low
back pain
Dr. J. Mata

Yuan J, Purepong N, Kerr DP, Park J, Bradbury I, McDonough S. Effectiveness of acupuncture for low back pain: a systematic review. Spine2008;33:E887-E900
Dr. J. Mata
A meta-analysis in 2008, which involved a total of 6359 patients Showed that real acupuncture treatments were no more effective than sham acupuncture treatments. There was nevertheless evidence that both real acupuncture and sham acupuncture were more effective than no treatment and that acupuncture can be a useful supplement to other forms of conventional therapy for low back pain.

Dr. J. Mata

Dr. J. Mata

A Multicenter, Randomized, Patient-Assessor Blind, Sham-Controlled Clinical Trial
Dr. J. Mata

Assessment and management of chronic pain
Institute for Clinical Systems Improvement (ICSI). Assessment and management of chronic pain. Bloomington (MN): Institute for Clinical Systems Improvement (ICSI); 2011 Nov. 112 p.
Acupuncture Clinical research with randomized, placebo-controlled trials supports the use of acupuncture for certain chronic pain conditions such as fibromyalgia [High Quality Evidence], [Low Quality Evidence], headache [Low Quality Evidence], back pain [Low Quality Evidence], neck pain [Low Quality Evidence], and osteoarthritis of the knee [Low Quality Evidence].
High Quality Evidence = Further research is very unlikely to change confidence in the estimate of effect. Low Quality Evidence = Further research is very likely to have an important impact on confidence in the estimate of effect and is likely to change the estimate or any estimate of effect is very uncertain.
Dr. J. Mata

Dr. J. Mata

Rubinstein SM, van Middelkoop M, Kuijpers T, et al. A systematic review on the effectiveness of complementary and alternative medicine for chronic non-specific low-back pain. Eur Spine J 2010 March 14 (Epub ahead of print).
Dr. J. Mata

Dr. J. Mata

GUIDELINES
Dr. J. Mata
The American College of Physicians and the American Pain Society have issued joint clinical practice guidelines recommending that clinicians consider acupuncture as one possible treatment option for patients with chronic low back pain who do not have a response to self-care. The level of supporting evidence for this recommendation was characterized as fair, and it was noted that recommendations may change as new studies become available.
•Chou R, Qaseem A, Snow V, et al. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann Intern Med 2007;147:478-491 •Chou R, Huffman LH. Nonpharmacologic therapies for acute and chronic low back pain: a review of the evidence for an American Pain Society/American College of Physicians clinical practice guideline. Ann Intern Med 2007;147:492-504[Erratum, Ann Intern Med 2008;148:247-8.

GUIDELINES
Dr. J. Mata
the North American Spine Society recently concluded that acupuncture provides better short-term pain relief and functional improvement than no treatment and that the addition of acupuncture to other treatments provides a greater benefit than other treatments alone. This review also identified a need for additional high-quality, randomized, controlled trials comparing acupuncture with no treatment and with sham acupuncture.
•Ammendolia C, Furlan AD, Imamura M, Irvin E,van Tulder M. Evidence-informed management of chronic low back pain with needle acupuncture.Spine J 2008;8:160-172

Dr. J. Mata
the U.K. National Institute for Health and Clinical Excellence has recommended acupuncture as a treatment option for patients with low back pain. As a result, the U.K. National Health Service now provides a maximum of 10 sessions of acupuncture over a period of 12 weeks for people with low back pain that has persisted for more than 6 weeks.
Low back pain: early management of persistent non-specific low back pain. Clinical guideline no. 88. London: National Institute for Health and Clinical Excellence, 2009.
GUIDELINES

Dr. J. Mata

Is Placebo Acupuncture What It is Intended to Be?
Lundeberg T,Lund I,Sing A, Na J eCAM 2009; doi:10.1093/ecam/nep049
Dr. J. Mata
Results, treatment of migraine
Results, treatment of low back pain

Is Placebo Acupuncture What It is Intended to Be?
Lundeberg T,Lund I,Sing A, Na J eCAM 2009; doi:10.1093/ecam/nep049
Dr. J. Mata
Results, treatment of knee osteoarthritis pain
• ACU sham procedures applied are not inert.
• Should therefore not be interpreted as placebo-controls in RCTs for the test of efficacy
• The evaluated effects of acupuncture could be compared with standard treatment
Conclusions

Sham interventions in randomized clinical trials of acupuncture – a review.
Dincer F, Linde K Complement Ther Med 2003, 11:235-242.
47 randomised controlled trials
Sham interventions Trials
Superficial needling of 'true' points
superficial needling of the acupoints for the treated condition 2
‘Irrelevant' acupoints
needling of the acupoints not for
the treated condition 4
‘Non-acupuncture' points
needling non-acupoints 27
‘Placebo needles'
devices that mimic acupuncture
without skin penetration 5
Pseudo-interventions
interventions that are not 'true' acupuncture e.g. use of switched-off laser
acupuncture devices)
9
Dr. J. Mata

Dr. J. Mata

Minimal acupuncture is not a valid placebo control in randomised controlled trials of acupuncture: a physiologist's perspective
Lund I, Näslund J, Lundeberg T. Chinese Medicine 2009, 4:1 doi:10.1186/1749-8546-4-1
Dr. J. Mata

Minimal acupuncture is not a valid placebo control in randomised controlled trials of acupuncture: a physiologist's perspective
Lund I, Näslund J, Lundeberg T. Chinese Medicine 2009, 4:1 doi:10.1186/1749-8546-4-1
Dr. J. Mata

Minimal acupuncture is not a valid placebo control in randomised controlled trials of acupuncture: a physiologist's perspective
Lund I, Näslund J, Lundeberg T. Chinese Medicine 2009, 4:1 doi:10.1186/1749-8546-4-1
Dr. J. Mata