-
8/4/2019 desordenes de NA
1/24
Clinical approach to disorders of salt and
water balance
Emphasis on integrative physiology
Mitchell L. Halperin, MD, FRCPC
a,*,Desmond Bohn, MB, FRCPC b
a Division of Nephrology, St. Michaels Hospital and the
University of Toronto,
St. Michaels Hospital Annex, 38 Shuter Street, Toronto, Ontario,
M5B 1A6, CanadabDepartment of Critical Care Medicine of the
Hospital for Sick Children,
and the Department of Anaesthesia, The University of Toronto,
555 University Ave.,
Toronto, Ontario, M5G 1X8 Canada
With our current emphasis on subspecialty medicine, consultants
suggest
possible diagnoses and treatments for patients who have
abnormalities withintheir areas of expertise. The medical team
responsible for the care of that patient
must integrate these suggestions into an overall management
plan. Therefore,
teamwork is especially important for the care of a patient.
The underlying basis for a given disorder may be revealed when
an integrative
analysis is performed. Some defects may only become evident
during therapy.
These challenges are especially important for problems in fluid
and electrolyte
balance in an intensive care unit (ICU) setting because they may
become life-
threatening very rapidly. How to anticipate and avoid these
dangers is illustrated
in the context of case examples selected for presentation in
this article.There are two different, but not mutually exclusive,
ways to arrive at a
clinical diagnosis and to design its therapy when the problem is
in the salt and
water area. The more traditional approach begins with data from
the history,
physical examination, and laboratory tests. This information is
used to generate
a list of possible causes of the disorder. Our approach differs
in that it begins
with the application of simple principles of physiology at the
bedside (Table 1)
[5]. It relies on deductive reasoning and a quantitative
analysis. The starting
point is defined by the consulting service what they believe to
be most
critical for their patient.
0749-0704/02/$ - see front matterD 2002, Elsevier Science (USA).
All rights reserved.
PII: S 0 7 4 9 - 0 7 0 4 ( 0 1 ) 0 0 0 0 8 - 2
* Corresponding author.
E-mail addresses: [email protected] (M.L. Halperin),
[email protected] (D. Bohn).
Crit Care Clin 18 (2002) 249272
-
8/4/2019 desordenes de NA
2/24
To make this article interactive, we pause periodically and ask
the readerquestions to consider prior to providing our discussion
of that issue. In
each case, there is an abnormal plasma sodium (Na+ )
concentration (PNa) in
an ICU setting.
Polyuria and hypernatremia
Illustrative case 1
Polyuria (current urine flow rate 10 ml/min) developed suddenly
in a
14-year-old boy (weight 50 kg, total body water 30 liters)
during resection
of a craniopharyngeoma. His PNa rose from 140 to 155 mmol/ over
6 hours. He
was given 3 liters of isotonic saline intravenously and his
urine output was
4 liters. He had also received an infusion of mannitol. The aim
of the consult
was to define goals of therapy for this patient.
Table 1
Physiologic principles used at the bedside
Physiologic principle Use at the bedside
Polyuria Divide polyuria into:
Urine volume = Osm/UOsm Osmotic diuresis if > 1000 mOsm/d
Organic solutes
Examine filtered load
Seek metabolic origin (e.g., urea)
Electrolytes (were they infused?)
Water diuresis (Uosm < Posm)
UOsm a osm excretion and flow rate
Impact of a change in PNa Main threat is change in brain ICF
volume
PNa inversely related to ICF volume Na+ content reflects the ECF
volume
Hypernatremia Basis revealed by tonicity balanceCaused by Na+
gain or water deficit Identify cause for the release of
vasopressin
Calcium receptor in the loop of Henle NaCl, K+ wasting and
concentrating defect
Creates furosemide-like effect Can be induced by cations
(gentamicin)
Catabolic state Confirmed by urea (572 mmol/100 g protein)
Protein oxidation causes urea appearance Therapy with exogenous
protein anabolics
Hyponatremia Ask if acute ( < 48 h) = increased brain
ICF volume
Find source of EFW and vasopressin Risk factors = young age,
women,
increased ECF volume
Calculate new ICF volume Urgent therapy 3% saline
Calculate ECF Na+ content Retained lavage fluid = different
Assess possible K+ deficiency Most are chronic (danger is
ODS)
Seek reason for vasopressin, especially
if a reversible cause might be present
Treat slowly ( < 9 mmol/L/d); slower if K+
deficit or malnourished
Abbreviations: U=urine; P=plasma.
M.L. Halperin, D. Bohn / Crit Care Clin 18 (2002) 249272250
-
8/4/2019 desordenes de NA
3/24
Initial quantitative analysis
The urine flow rate of 10 ml/min, if extrapolated over 24 hours,
is
equivalent to 14.4 liters per day. This volume exceeds the
patients extracellularfluid (ECF) volume and is virtually equal to
half of total body water. Faced
with this medical emergency, we ask the reader: What was
responsible for this
massive polyuria?
What was responsible for this massive polyuria?
Physiology principle 1. The urine flow rate is a function of two
factors
(Eq. 1). Hence polyuria has two causes, a larger than normal
solute excretion rate
(osmotic diuresis) and/or an inability to raise the
concentration of solutes in the
urine appropriately (water diuresis). In an osmotic diuresis,
each liter of urinecontains at least 300 milliosmoles of the
causative solute (and other solutes as
well) [32].
Urine f low rate liters=day
Number of Solutes excreted=Solutesurine 1
Return to the bedside. Using the values from surgery, 3
milliosmoles of extra
solutes (10 ml/min a minimum of 300 milliosmoles/l in an osmotic
diuresis)
would need to be excreted each minute if this was a glucose,
urea, or mannitol-induced osmotic diuresis. This would require the
presence of very high concen-
trations of these organic solutes in plasma if one of them
caused the polyuria. If the
urine composition were not available, the following calculation
could be
performed to determine whether enough solutes were filtered to
cause the osmotic
diuresis. With a normal glomerular filtration rate (GFR), the
concentration of
glucose in the filtrate would have to be 27 mmol/l (486 mg/dl)
higher than the
renal threshold of 10 mmol/l (180 mg/dl) to filter 3 mmol of
glucose per min to
permit it to cause this degree of osmotic diuresis (24 mmol/l
0.125 l/min).
Hence the blood sugar levels would need to be 666 mg/dl (37
mmol/l) for this to bea glucose-induced osmotic diuresis [14]. If
urea were the principal urine osmole,
its concentration in plasma would have to be close to 60 mmol/l
(BUN 168 mg/dl)
because close to half of the filtered urea is normally
reabsorbed [9]. Even higher
plasma concentrations would be needed if the GFR were lower than
125 ml/min.
For mannitol, at least 50 g ($ 290 mmol) would have to be
infused for every literof urine excreted.
Based on this, extra information was sought. Because the blood
sugar and
BUN were both in the normal range and the quantity of mannitol
infused was too
small, an osmotic diuresis due to organic solutes was ruled out.
The fact that theurine Na+ + potassium (K+ ) concentration was only
50 mmol/l ruled out a saline-
induced osmotic diuresis. Therefore the basis for the polyuria
was a water
diuresis, a diagnosis that was confirmed when his urine
osmolality was known
(120 mOsm/kg H2O).
The next question is, What was the cause of the large water
diuresis? It is
essential to recall that his PNa was 155 mmol/l during the
polyuria.
M.L. Halperin, D. Bohn / Crit Care Clin 18 (2002) 249272 251
-
8/4/2019 desordenes de NA
4/24
What was the cause of the large water diuresis?
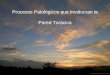
Physiology principle 2. The control system for water has its
sensor
(specialized area of the hypothalamus) in a different location
from one of itsresponse elements (excretion of water by the
kidney). Therefore a messenger
(vasopressin) must communicate between these two locations (Fig.
1). The cell
volume of the central osmostat shrinks sufficiently when the PNa
exceeds
140 mmol/l and this leads to an augmented release of
vasopressin. Vasopressin
causes the distal segments of the nephron to become permeable to
water due to
the insertion of water channels [27], causing the urine to
become maximally
concentrated (the urine osmolality should be 34-fold higher than
the plasma
osmolality) [29].
Return to the bedside. A lesion releasing vasopressinase was
unlikely in thispatient. There were two factors suggesting that the
likely diagnosis was central
diabetes insipidus (DI). First, there was the neurosurgery and a
disease process
(craniopharyngeoma) that could have compromised the ability to
release vaso-
pressin from the hypothalamus. Second, there was a large water
diuresis (the
urine osmolality was 120 mOsm/kg H2O) despite the presence of a
stimulus for
the release of vasopressin (hypernatremia). To confirm that the
DI was central
rather than nephrogenic in origin, vasopressin was administered.
Bearing in mind
that vasopressin acts in a matter of minutes [27], we ask the
reader, How low
should the urine flow rate be when vasopressin acts?The measured
value forthis urine flow rate was 6 ml/min.
Fig. 1. Control system for water excretion. The circles
represent structures in the hypothalamus. The
tonicity stat (osmostat) detects a change in the PNa. Because of
hypernatremia (box on the left), this
center leads to the release of vasopressin (VP). Vasopressin
acts on the distal nephron to cause it to
become permeable to water leading to the excretion of
concentrated urine. There are also non-osmotic
stimuli that influence the release of vasopressin.
M.L. Halperin, D. Bohn / Crit Care Clin 18 (2002) 249272252
-
8/4/2019 desordenes de NA
5/24
How low should the urine flow rate be when vasopressin acts?
Application of physiology principle 1. First, the urine flow
rate depends on
two factors, the number of impermeable solutes (effective or
non-urea osmoles) inthe lumen of the terminal collecting duct and
the effective osmolality (non-urea
osmolality) of the papillary medullary interstitium (Eq. 1)
[11]. Second, a typical
diet leads to the excretion of 800 mosmoles/day, with half being
urea and the other
half, electrolytes. Third, because the non-urea osmolality can
rise to 600 mOsm/kg
H2O when vasopressin acts, the expected urine flow rate is close
to 0.67 ml/min
under these conditions (400 mosmoles of electrolytes excreted at
a concentration
of 600 mosmoles per liter). Fourth, the maximum total and
effective osmolalities
in the renal interstitial compartment decline during a prior
water diuresis and it
takes time to reconstitute this environment after vasopressin
acts. Return to the bedside. A urine osmolality of 120 mOsm/kg H2O
is not the
expected value during a water diuresis when the urine flow rate
is 10 ml/min.
Rather, the urine osmolality should have been 50 60 mOsm/kg H2O
if 800
milliosmoles were excreted in 1440 min (0.50.6 milliosmoles/min)
[5]. More-
over, in a water diuresis, water is largely impermeable in the
distal nephron.
Therefore a high rate of excretion of osmoles should not
influence the urine flow
rate when there is a lack of vasopressin. In contrast, when
vasopressin acts, the
osmole excretion rate will exert a major effect on the urine
flow rate (Eq. 1).
A change in urine flow rate is obvious at the bedside whereas a
delay isexpected before the laboratory reports the urine
osmolality. Therefore clinical
decision making will be based initially on the decline in urine
flow rate. On the
one hand, normal subjects have a minimum urine flow rate of
close to 0.5 ml/min
when vasopressin acts [30]. Accordingly, one might anticipate
that the urine
volume should fall to 0.5 ml/min after vasopressin was given. A
surprise is in
store if this were the logic used. The error would be to rely on
data obtained from
one setting (normal subjects) and apply them to this patient in
the ICU.
Comment. Had a physiologic analysis been performed at the time
when the
urine flow rate was 10 ml/min, the observed decrease to 6 ml/min
aftervasopressin administration could have been anticipated if
three facts were taken
into account. First, the patient was excreting effective osmoles
(urine electrolytes)
at a rate that was close to 3-fold that of subjects consuming a
typical Western diet
(10 ml/min 50 mmol Na+ + K+ /l = 0.5 mmol/min) vs. the expected
225 mmolNa+ + K+ /day or 0.15 mmol/min. Second, the huge water
diuresis that occurred
prior to the administration of vasopressin should diminish the
medullary inter-
stitial osmolality and this would take time to be reconstituted.
Thus the maximum
urine osmolality would be similarly reduced. Third, the peak
natriuresis might not
have been reached at the time that the first urine osmolality
was measured. Indeed,the rate of osmole (Na+ + K+ ) excretion
continued to rise after vasopressin was
given. Thus a urine flow rate after vasopressin that was more
than 10-fold that of
subjects consuming a typical Western diet was a more realistic
expectation. Hence,
by not applying physiologic principles to the bedside, a series
of compounding
errors were set into motion that had grave consequences for the
patient. One of the
errors was to give multiple doses of a long-acting preparation
of vasopressin,
M.L. Halperin, D. Bohn / Crit Care Clin 18 (2002) 249272 253
-
8/4/2019 desordenes de NA
6/24
dDAVP. The grave consequences of this error in therapy will be
discussed in the
response to the question, what was the occult threat to
survival?
Now we ask the reader to consider, What is the basis of
hypernatremia in this patient with central DI?
What is the basis of hypernatremia in this patient with central
DI?
Physiology principle 3. To raise the PNa by 10%, there must
either be a gain
of Na+ and/or a deficit of water in the ECF compartment (Table
1). In quan-
titative terms, the gain of Na+ is calculated in total body
water terms so a rise in
PNa of 15 mmol/l requires a positive balance of approximately
450 mmoles of
Na+ (15 mmol/l 30 liters total body water (i.e., 60% of body
weight in this
patient). On the other hand, because water distributes across
all body fluidcompartments in proportion to their volumes [33], the
deficit of water must be
close to 10% of total body water (10% 30 liters, or 3 liters) to
cause theobserved 10% rise in PNa.
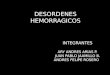
Return to the bedside. We begin with an analysis based on
electrolyte-free
water (water without Na+ + K+ ) to illustrate its limitations
(Fig. 2). To think in
electrolyte-free water terms [10,23,28], an imaginary
calculation is performed
where the 4 liters of urine in our patient are divided into 1.3
liters of isotonic saline
(use 150 mmol of Na+ + K+ /liter for simplicity) and the
remaining 2.7 liters is
called electrolyte-free water (Fig. 2). It is important to
calculate an electrolyte-free water balance rather than focus on
either excretion or input to determine why
the PNa changed. This can easily be done in our patient because
the input
contained 0 liters of electrolyte-free water while 2.7 liters of
electrolyte-free water
were excreted. This negative balance of 2.7 liters of
electrolyte-free water should
raise the PNa by close to 15 mmol/l (140 mmol/l (30/27.3
liters). If anelectrolyte-free water balance were used to design
therapy, a positive balance of
Fig. 2. Calculation of electrolyte-free water. The urine volume
in Case 1 was 4 liters (large rectangle)
and its Na+ + K+ concentration was 50 mmol/l (left of arrow).
This solution can be divided into two
imaginary components, 1.3 liters of isotonic saline (150 mmol
Na+ + K+ /liter) and 2.7 liters of
electrolyte-free water (EFW). (From RossMark Medical Publishers,
The Acid Truth and Basic Facts,
4th ed, 1997; with permission) [13].
M.L. Halperin, D. Bohn / Crit Care Clin 18 (2002) 249272254
-
8/4/2019 desordenes de NA
7/24
2.7 liters of electrolyte-free water should be induced to
correct the hypernatremia.
Notwithstanding, there are many ways to achieve a negative
balance of 2.7 liters
of electrolyte-free water [3]. For example, if we made a change
only to thevolume of isotonic saline infused during the period in
which hypernatremia
developed (now 4 liters instead of 3 liters), there is still no
electrolyte-free water
administered so the balance for electrolyte-free water is still
minus 2.7 liters.
Therefore the rise in PNa would be identical, but its basis
would be different
(Table 2). Obviously, the goals of therapy should also be
different in these
examples despite the fact that the negative balance of
electrolyte-free water and
rise in PNa were identical. Therefore one cannot rely on an
electrolyte-free water
balance to guide therapy (Table 2). [3].
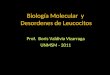
A better way to determine why the PNa changed is to calculate a
tonicity balance (Fig. 3) where all inputs and outputs are also
divided into two
components, total volume of water and Na+ + K+ each of which is
analyzed
separately [3]. Mass balance for Na+ plus K+ rather than just
Na+ must be
included because Na+ may enter cells in conjunction with the
exit of K+ [8].
Thus the loss of K+ with chloride (Cl ) or bicarbonate can be
thought of as a
loss of their Na+ salts from the ECF compartment. When
considering Na+ + K+
in isolation, for every mmol retained per liter of total body
water, the rise in PNawill be 1 mmol/l [33]. Similarly, a gain of 1
liter of water, when considered in
isolation should lower the PNa by the formula: PNa (1/total body
water).In addition to predicting the rise in PNa [3], the tonicity
balance also provides
reliable information about its cause (Table 2). In our patient,
the volume of water
infused was 1 liter less than the urine volume. Recall that 3
liters of net water loss
would be required to raise the PNaby 10%. Therefore
hypernatremia in our patient
was not due solely to a water deficit despite the large
electrolyte-free water
diuresis. Since the patient was given 450 mmol Na+ and excreted
200 mmol Na+
(+ K+ ) in his urine, there was a net gain of 250 mmol of Na+ +
K+ . The
Table 2Hypernatremia and a negative balance of 2.7 L of
electrolyte-free watera
Na+ + K+Therapy from balances
(mmol) Water (L) EFW (L) EFW Tonicity
Case 1
Input 450 3 0
Output 200 4 2.7
Balance + 250 1 2.7 + 2.7 L H2O + 1 L H2O 250 mmol Na+
Change IV to 4L of isotonic saline
Input 600 4 0
Output 200 4 2.7
Balance + 400 0 2.7 + 2.7 L H2O 0 L H2O 400 mmol Na+
a The PNa rose from 140 to 155 mmol/L in each setting. The only
difference is the volume of
isotonic saline infused over the time period of observation. In
both settings, there is a negative balance
of 2.7 liters of electrolyte-free water (EFW). The goals of
therapy to correct the hypernatremia were
clear only after a tonicity balance was calculated.
M.L. Halperin, D. Bohn / Crit Care Clin 18 (2002) 249272 255
-
8/4/2019 desordenes de NA
8/24
combination of a deficit of 1 liter of water and a gain of 250
mmol of Na+ would
explain the rise in PNa. In contrast to information provided by
an electrolyte-free
water balance, the tonicity balance revealed the goals for
therapy create a
negative balance of 250 mmol of Na+
(+ K+
) along with a positive balance of1 liter of water (Table 2).
This therapy will correct hypernatremia and return both
the ICF and ECF compartment volumes to normal. Moreover, the
tonicity balance
provides a physiologic basis for the clinical implications of
hypernatremia. When
a tonicity balance is used in the hypothetical example (i.e.,
when 4 liters of isotonic
saline were administered), it is clear that the goals of therapy
are to create a
negative balance for Na+ + K+ of 400 mmol and a nil balance of
water. Given the
short time interval, insensible losses would be relatively
small. Therefore, because
of the absence of fever, we would not include them in this
patient.
Clinical course. After administration of vasopressin, the
measured concen-trations of Na+ + K+ in the urine rose to 175
mmol/l. The intravenous fluid
therapy was half-isotonic saline (close to 75 mmol Na+ /liter)
at volumes equal
to the urine output this caused a deficit of almost 100 mmol of
Na+ per liter
of throughput. After the excretion of 2.5 liters of urine, the
desired negative
balance of 250 mmol of Na+ would have occurred. The other goal
of therapy
was to expand his body water by 1 liter and this was achieved by
giving a
positive balance of 1 liter of electrolyte-free water (i.e., 1
liter of D5W if
hyperglycemia was not present). At this point, both his ICF and
ECF volumes
and composition would be restored to normal (PNa would be 140
mmol/l). Asuccessful clinical outcome was anticipated. We ask the
reader,What is the
occult threat to survival?
What was the occult threat to survival?
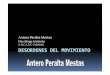
Application of physiology principle 3. The PNa is used to
reflect the volume
of the ICF compartment for three reasons (Fig. 4). First, water
crosses cell
Fig. 3. Calculation of a tonicity balance. The rectangle
represents the body with its concentration of
Na + . The input of Na+ + K+ and of water are shown on the left;
the output of Na+ + K+ and of water
are shown on the right of this rectangle in Case 1. Balances are
shown in dashed boxes inside
the rectangle.
M.L. Halperin, D. Bohn / Crit Care Clin 18 (2002) 249272256
-
8/4/2019 desordenes de NA
9/24
membranes rapidly to achieve osmotic equilibrium. Second, the
number ofeffective osmoles (osmoles other than urea) in the ICF
compartment remains
constant in most acute settings. Third, in the absence of
hyperglycemia and/or
mannitol accumulation in the ECF compartment, the effective ECF
osmoles are
Na+ and its attendant anions, Cl and bicarbonate. Therefore when
hyper-
natremia develops, the volume of cells will be smaller unless
there was a
gain in ICF osmoles in muscle for example due to a recent
seizure [36] or
rhabdomyolysis [15].
The target organ of clinical importance is the brain because it
is in a
confined rigid space and it cannot gain intracellular particles
in an acute setting.The main danger in this setting is an
intracerebral hemorrhage. In contrast,
hyponatremia usually implies that its ICF volume is expanded and
ultimately may
lead to cerebral herniation because of the rigidity of the skull
and the fact that
close to 67% of total brain water is in its ICF compartment.
Return to the bedside. Once the PNa has returned to 140 mmol/l,
progressive
acute hyponatremia from ongoing negative Na+ balance is a real
danger unless
therapy is modified quickly. One can anticipate that the urine
Na+ concentration
may be almost as high as the medullary interstitial Na+ + K+
concentration
when vasopressin acts because of the low urea concentration in
the renalmedullary interstitium (the result of the low urine urea
concentration). Because
a long-acting ($ 10 h) form of vasopressin (dDAVP) was given and
the vastmajority of urine osmoles were Na+ + K+ salts, it is not
surprising that the urine
Na + concentration rose to 300 mmol/l (Fig. 5). Therefore it is
easy to anticipate
why hyponatremia would develop during therapy to correct
hypernatremia
because half-isotonic saline (75 mmol Na+ /l) was given at a
rate equal to urine
Fig. 4. PNa Concentration reflects the ICF volume in the absence
of hyperglycemia and mannitol
infusion. The circle represents the ICF compartment that
contains macromolecular anions (P ) and its
major effective osmole, the cation K+ . Urea, shown on the left,
is not an effective osmole because it
virtually always has an equal concentration in the ECF and ICF
compartments. The osmoles restricted
to the ECF compartment are Na+ and its attendant anions. Osmotic
equilibrium is achieved because
water can cross this cell membrane rapidly.
M.L. Halperin, D. Bohn / Crit Care Clin 18 (2002) 249272 257
-
8/4/2019 desordenes de NA
10/24
output. Because this strategy was not changed when the PNa fell
to 140 mmol/l,
the patient became progressively hyponatremic and died due to
brain swelling thatled to herniation. We ask the reader, How could
this fatal outcome be avoided?
How could this fatal outcome be avoided?
Application of physiology principle 3. To prevent a change in
the PNa, the
input must be identical to the output both in terms of volume
and electrolyte
content (Fig. 5).
Return to the bedside. There are two ways to achieve a tonicity
balance
(Fig. 5). First, one could infuse saline at the same
concentration and flow rate as
in the urine; second, one could administer a loop diuretic to
lower urine Na
+
+K+ concentration to approximate that of plasma. With this
latter strategy, giving
isotonic saline at the same rate as the urine output could have
replaced all renal
losses other than K+ while preventing a fall in the PNa. At any
point before the
tragic end, his PNa could have been raised to a non-threatening
level easily by the
administration of 1 mmol Na+ (without water) per liter of total
body water times
the desired change in the PNa. Raising his PNa from 125 mmol/l
to 130 mmol/l
would have required a positive balance of 150 mmol of Na+ (5
mmol/l 30 liters) which could have been accomplished by the rapid
infusion of close to
0.3 liters of 3% NaCl. It is important to recognize that a
reasonably rapid rate ofcorrection of hyponatremia is not a risk
factor for osmotic demyelination in a
patient with acute hyponatremia [31].
Concluding remarks for case 1
Using simple whole body physiology (Table 1), deductive
reasoning, and a
quantitative analysis emphasizing mass balance, the basis of the
polyuria was
Fig. 5. Options of therapy to prevent the development of
hyponatremia. The actions of vasopressin led
to the urinary excretion of 1 liter of hypertonic saline (300
mmol/l) in Case 1. To avoid the
development of hyponatremia, the intravenous infusion and urine
output must have the same
concentrations of Na+ (+ K+ ) and the same volume. Thus either
the concentration of saline infused
must be 300 mmol/l or the urine must be adjusted so that it
becomes close to isotonic saline (give a
loop diuretic). (From RossMark Medical Publishers, The Acid
Truth and Basic Facts, 4th ed, 1997;
with permission.)
M.L. Halperin, D. Bohn / Crit Care Clin 18 (2002) 249272258
-
8/4/2019 desordenes de NA
11/24
clearly a water diuresis due to central DI. By calculating the
osmole excretion rate
and deducing that there was an excessive excretion of
electrolytes, it was important
to predict that the urine flow rate might only decline to around
6 ml/min aftervasopressin was given. Armed with these insights, the
patient would not have been
given so large a dose of this hormone. For therapy, the
objectives were also clear
return the body compartment volumes and composition to normal.
Using a tonicity
balance, the basis of hypernatremia was a positive balance of
250 mmol of Na+ (and
Cl ) and a deficit of 1 liter of water. Accordingly, the design
of therapy was to
create a negative balance for Na+ (250 mmol) while increasing
water balance by
1 liter. Moreover, the dangers in this setting could be
anticipated. Once the PNareturned to normal, one must maintain Na+
and water balances. Because the urine
Na+
concentration was high and the urine flow rate was also large,
intravenoussolutions should be given at the same rate as the urine
output while ensuring that
their overall Na+ concentration was equal to that of the urine
(Fig. 5).
Perhaps the simple take-home message is that a physiological
approach should
be the one used at the bedside in the ICU. There are two other
points that merit
emphasis. First, from a practical and safety perspective, it is
critical to monitor the
PNa closely during and after therapy to be sure the goals of
therapy are indeed
being achieved. Second, because hypernatremia developed so
acutely, it should
not be dangerous to return the PNa to normal over a period of
one day.
Illustrative case 2
Three problems prompted the transfer of a 70-kg male to the ICU
following a
recent bone marrow transplant. First, he was heavily
immunosuppressed and
developed an acute respiratory tract infection for which he was
treated with
antibiotics including gentamicin. Second, he became hypotensive
(blood pressure
nadir was 65/40 mm Hg) yet he developed non-oliguric acute renal
failure (plasma
creatinine rose from 0.9 to 4.6 mg/dl (100 to 412 mmol/l), BUN
rose from 14 to
213 mg/dl, urea 5 to 76 mmol/l). Third, his PNa
rose from 140 to 157 mmol/l over
several days in the ICU. Balance data were available for the day
his PNa rose from
147 to 155 mmol/l. They revealed a positive balance of both 1
liter of water and
378 mmol Na+ + K+ (7 liters of hypotonic saline (Na+ + K+ of 90
mmol/l) were
infused and he excreted 6 liters of urine (Na+ + K+
concentration of 42 mmol/l)
(Fig. 6). His urine osmolality was 524 mOsm/kg H2O.
At this point, we ask the reader to consider the following
questions. What
was the basis of the polyuria and hypernatremia? Why was the
urine Na+ +
K+ concentration so low?
What was the basis of the polyuria?
Physiology principle 4. Function of the thick ascending limb of
the loop of
Henle (TAL) is needed to concentrate the urine and for
conservation of Na+ and
Cl by the kidney. These cells have a calcium receptor on their
basolateral
aspect (facing the blood side, Fig. 7). When this receptor is
occupied by a
M.L. Halperin, D. Bohn / Crit Care Clin 18 (2002) 249272 259
-
8/4/2019 desordenes de NA
12/24
cationic ligand such as calcium or gentamicin, the kidney
behaves as if it were
under the influence of a loop diuretic because of an
intracellular signal trans-
duction cascade that leads to inhibition of K+ movement from
these cells into the
lumen. The net result is a renal concentrating defect and a high
rate of excretion
of Na+ (and Cl ).
Fig. 6. Tonicity balance in case 2. For details, see text and
the legend to Fig. 3.
Fig. 7. Physiology of the calcium receptor in the loop of Henle.
A cell in the thick ascending limb of
the loop of Henle (TAL) is depicted on the right portion of the
Figure. When the calcium receptor on
its basolateral aspect is occupied, its luminal ROM-K channel is
inhibited. When fewer K+ enter the
lumen, there is insufficient K+ for the luminal Na+ , K+ , 2 Cl
cotransporter and less positive luminal
voltage to drive the paracellular reabsorption of Na+ , Ca2+ and
Mg2+ .
M.L. Halperin, D. Bohn / Crit Care Clin 18 (2002) 249272260
-
8/4/2019 desordenes de NA
13/24
Return to the bedside. Using the physiological principles
illustrated in Table 1, it
is clear that the basis for the polyuria was an osmotic diuresis
(very high daily
osmole excretion rate, 6 liters 524 mOsm/liter = 3144 mosmoles
per day). Thebulk of these osmoles were non-electrolytes (2 (Na+ +
K+ ) = 84 mOsm/kg H2O).Only one solute (urea) was filtered in
sufficient quantity to cause this osmotic
diuresis. Hence the presumptive diagnosis was a urea-induced
osmotic diuresis
(confirmed later by direct analysis of urea). Notwithstanding,
two other features
contributed to this polyuria. First, there was a high daily rate
of excretion of Na+ +
K+ (6 liters 42 mmol/l = 252 mmol/day). Second, the
furosemide-like effectdue to gentamicin (Fig. 7) could have led to
a lower renal medullary interstitial
tonicity and thereby a lower than expected urine osmolality in
the face of
a calculated plasma osmolality of 390 mOsm/kg H2O (2 157 mmol
Na+
/l +76 mmol urea/l).
What was the basis of the hypernatremia?
A tonicity balance calculation (Fig. 6) revealed that the basis
for the hyper-
natremia was the positive balance of 378 mmol of Na+ + K+
because there was
also a positive balance of 1 liter of water. Thus his ECF volume
was expanded
(Na+ gain) rather than being contracted (a deficit of water will
cause hyper-
natremia with a contracted ECF volume).
Why was the urine Na+ + K+ concentration so low if vasopressin
is acting?
When there is a lesion that limits the rise in the urine
osmolality (furosemide-
like effect attributable to gentamicin, Fig. 7), a higher rate
of excretion of organic
solutes (urea in this case) obligates a lower concentration of
electrolytes in each
liter of urine (Fig. 8). At this point, we again ask the reader
to pause and consider,
What is the next threat to survival in this patient?
What is the next threat to survival in this patient?
Physiology principle 5. The catabolism of proteins leads to the
production of
urea, the major nitrogenous waste product [18] (Fig. 9). Because
lean body
mass has water as its main constituent (80% of weight), these
tissues contain
180 g of protein per kg. For every 100 g of protein oxidized, 16
g of nitrogen
is converted to urea (572 mmol of urea) [16]. Therefore the
appearance in the
urine of close to 1100 mmol of urea from endogenous sources
represents the
net catabolism of 1 kg of lean body mass. Because of its size,
muscle catab-
olism is the major contributor when there is a very high rate of
appearance of
urea. This can cause a problem because muscle function is needed
to clearrespiratory secretions.
Return to the bedside. On the day the tonicity balance was
carried out, the
patient excreted 6 liters of urine with a urea concentration of
close to 400 mmol/l.
Therefore 2400 mmol of urea were excreted, representing the net
catabolism of
close to 200 g of protein. On that day, he was given 60 g of
protein by nasogastric
M.L. Halperin, D. Bohn / Crit Care Clin 18 (2002) 249272 261
-
8/4/2019 desordenes de NA
14/24
tube so he catabolized approximately 140 g of endogenous
protein. This was
likely derived from almost 0.8 kg of lean body mass (Fig. 9).
Should this
Fig. 9. Catabolism of lean body mass to cause a urea-induced
osmotic diuresis. With low levels of
anabolic hormones and high levels of catabolic factors, there is
net breakdown of muscle protein and
release of amino acids. Amino acids are delivered to the liver
where their nitrogen is converted to urea
while carbon/hydrogen is converted to glucose by a common
pathway for the most part. The urea so-
formed becomes the principal urinary nitrogen waste. A
quantitative analysis is shown by the numbers
in parentheses. Control exerted at site 1.
Fig. 8. Exacerbation of polyuria by a renal medullary lesion.
The rectangle on the left represents 1 liter
of urine excreted per day when vasopressin acts, the medullary
interstitial osmolality is 900 mOsm/kg
H2O, and half of the urine solutes are urea (the other half are
electrolytes (lytes)). With a major
concentrating defect limiting the maximum urine osmolality to
300 mOsm/kg H2O as the only change,
the urine volume will now be 3 liters per day and the urine Na+
+ K+ concentration will be hypotonic
as shown to the right of the arrow.
M.L. Halperin, D. Bohn / Crit Care Clin 18 (2002) 249272262
-
8/4/2019 desordenes de NA
15/24
continue, he would ultimately undergo marked muscle wasting (and
he did).
Protein wasting could make his lung infection worse by
compromising efforts to
clear secretions from his respiratory tract as well as
diminishing his immuno-logical responses to infection [20].
Summary. Had the true basis for polyuria and hypernatremia been
recognized,
efforts would have been more vigorous at the nutritional level
in this patient. On
the one hand, more exogenous calories including protein could
have been given.
On the other hand, anabolic hormones such as high dose insulin
with glucose to
avoid hypoglycemia and/or provision of nutritional supplements
such as gluta-
mine [20] might have been tried to minimize protein catabolism.
One might also
have questioned the use of high doses of catabolic hormones such
as glucocorti-coids at this point because of his extreme degree of
catabolism.
Concluding remarks for case 2
Perhaps the simple message in Case 2 is to perform a balance of
all
major constituents of the urine. From the Na+ and water
perspective, a urea-
induced osmotic diuresis caused polyuria. Hypernatremia
developed because
isotonic saline was infused whereas the urine had a much lower
concen-
tration of Na+ + K+. More importantly, from an integrative
physiology point
of view, these salt and water issues were the clues to reveal
the very large
endogenous protein catabolism with its potential threats for
survival.
Hyponatremia
The first decision one must make when dealing with a patient
with hy-
ponatremia (PNa less than 136 mmol/l) is to determine whether it
represents an
acute condition (documented course is less than 48 hours). The
reason for this
emphasis is that the main danger in acute hyponatremia results
from brain cellswelling whereas the main danger with chronic
hyponatremia is the osmotic
demyelination syndrome (ODS) that occurs secondary to its
treatment [35]. In
fact, one usually begins with therapeutic considerations in
acute hyponatremia
and with diagnostic considerations in chronic hyponatremia. If
even mild
symptoms begin in a patient with acute hyponatremia, clinical
deterioration
may be very rapid so treatment must be prompt and vigorous.
Acute hyponatremia
Illustrative case 3
A 17-month-old infant weighing 10 kg had a 2-day history of
gastroenteritis.
Physical examination revealed a normal ECF volume, but one
observer said that he
was somewhat dry. There was a mild degree of hyponatremia
(PNa134 mmol/l)
M.L. Halperin, D. Bohn / Crit Care Clin 18 (2002) 249272 263
-
8/4/2019 desordenes de NA
16/24
and a urine osmolality of 320 mOsm/kg H2O; the urine volume was
not recorded
throughout his hospital course. Despite these minor
abnormalities, he was given
a bolus of isotonic saline (200 ml, 30 mmol Na+
) and a maintenance infusion of2/3 D5W and 1/3 isotonic saline
at 40 ml/h for the next 20 hours (total volume,
750 ml, 37.5 mmol Na+ ). He received an estimated 200 ml of
water as ice chips
because of a dry mouth. He improved initially, but 20 hours
after the start of
therapy, a seizure occurred. His PNa at this time was 121
mmol/l.
We ask the reader to consider: Why did acute hyponatremia
develop?
What would your therapy be bearing in mind that he has had a
seizure? To
prevent the development of hyponatremia, what should the initial
therapy be?
Are there specific risk factors for hyponatremia in certain
patients who receive
electrolyte-free water?
Why did acute hyponatremia develop?
Physiology principle 6. To develop hyponatremia, there must be
both a source
of electrolyte-free water and a means to decrease its rate of
excretion (Table 1);
the latter is due to renal actions of vasopressin [27]. The
quantity of Na+ in the
ECF compartment is close to 30 mmol/kg body weight (Table 1); a
10-kg normal
infant has 2 liters of ECF and 280 mmol of Na+.
Return to the bedside. Vasopressin could have been released in
response to a
number of non-osmotic stimuli including the underlying GI
disturbance (Table 3).
He had three source of electrolyte-free water. First, hypotonic
solutions were
infused. Second, electrolyte-free water was given orally in the
form of ice
chips. Third, electrolyte-free water was generated by the kidney
by a process
that we call desalination of infused isotonic saline (Fig. 10);
this process
requires a large natriuresis [34]. Because he was given close to
7 mmol of Na+
per kg, his ECF volume would be expanded by 20% providing a
stimulus for
Na+
excretion.
Table 3
High vasopressin levels in patients with hyponatremia
Readily reversible causes
Low effective circulating volume
Anxiety, stress pain, nausea
Drugs causing nausea (e.g., chemotherapeutic agents), the
central release of vasopressin (e.g.,
morphine) or enhancement of the renal effects of vasopressin
(e.g., certain oral hypoglycemics,
nonsteroidal anti-inflammatory drugs)
Endocrine causes (e.g., hypothyroidism, adrenal
insufficiency)
Exogenous DDAVP, oxytocin
Not easily reversible causes
Vasopressin-producing tumors
Central nervous system or lung lesions (may cause reset
osmostat)
Granulomas
Certain metabolic lesions (e.g., porphyria)
M.L. Halperin, D. Bohn / Crit Care Clin 18 (2002) 249272264
-
8/4/2019 desordenes de NA
17/24
What should your therapy be bearing in mind that he has had a
seizure?
Application of physiology principle 3. The ICF volume is
inversely propor-
tional to the PNa (Fig. 4). To lower the ICF volume, one must
give solutes such as
Na+ (and Cl ) or mannitol that are restricted to the ECF
compartment. To draw
water out of the skull by osmosis to reduce intracranial
pressure, the solute given
must not readily cross cerebral capillaries. Hypertonic Na
+
and mannitol causeosmotic shrinking of the brain because they do
not readily cross the blood-brain
barrier [26].
Return to the bedside. Treatment must be aggressive even if only
mild
symptoms were present. Hypertonic saline (3%) should be given
intravenously
to raise the PNa by 5 mmol/l in 1 2 hours; this should alleviate
significant
cerebral swelling and hopefully prevent irreversible damage. The
calculated
dose of NaCl depends upon body weight (10 kg) and in infants,
water is 70%
of body weight. Because total body water is approximately 7
liters, he wouldneed 35 mmol (5 mmol/l 7 liters) to raise his PNa
by 5 mmol/l. This isequivalent to close to 80 ml of 3% saline ($
500 mmol/l). A potential danger ofthis infusion is over-expansion
of his ECF volume, but this risk is minor.
Longer-term treatment would depend on the volume and tonicity of
the urine.
Having said all this, the emphasis should have been on correct
therapy when
the child was admitted.
Fig. 10. Generation of electrolyte-free water by the kidney. The
larger rectangle to the left of the
arrows represents the infusion of 2 liters of isotonic saline;
the content of Na + (300 mmol) is shown in
the oval inside that rectangle. A similar depiction is used for
the excretion of Na + and water and they
are shown to the right of the arrows. To have a concentration of
Na + in the urine that is 300 mmol/l,
vasopressin (VP) must act and there must be a reason to excrete
NaCl. The remaining 1 liter of
electrolyte-free water is retained in the body.
M.L. Halperin, D. Bohn / Crit Care Clin 18 (2002) 249272 265
-
8/4/2019 desordenes de NA
18/24
To prevent the development of hyponatremia, what should the
initial therapy be?
Application of physiology principles 1 and 3. The excretion of
Na+
is increasedwhen the ECF volume is expanded. If vasopressin is
present, the concentration of
Na+ + K+ in the urine can be very high, generating
electrolyte-free water that will
be retained in the body (Fig. 10).
Return to the bedside. Acute hyponatremia in hospitalized
patients should be a
problem of the past. Prevention depends upon limiting the access
to electrolyte-
free water in a patient likely to have vasopressin acting. The
administration of
hypotonic infusions is contraindicated in our patient because
his PNa is less than
138 mmol/l. Since electrolyte-free water can be generated by the
kidney as aresult of a large natriuresis when vasopressin acts
(Fig. 10), one should give only
as much isotonic saline as needed for hemodynamic purposes. It
is not advisable
to administer a large volume of isotonic saline to achieve a
good urine output
because the good urine output may really be a danger sign if the
urine tonicity
is high. If the urine were hypertonic, it should be replaced
with the same volume
and tonicity as was excreted or, alternatively, the composition
of this urine could
be changed to near-isotonic saline with a loop or osmotic
diuretic and again its
total volume replaced with isotonic saline (Fig. 5).
Are there specific risk factors for the development of acute
hyponatremia in
certain patients who receive electrolyte-free water?
Application of physiology principle 3. Close to 50% of body
water is in skeletal
muscles. The major constituent (80%) of the brain is water.
Approximately 2/3 of
this water is in cells and this volume increases with
hyponatremia. Therefore for a
given % swelling, the larger the brain cell/total volume in the
skull, the greater
the rise in intracranial pressure. On the other hand,
hyponatremia that is due to the
addition of an iso-osmotic mannitol solution will expand the ECF
volume but it
will not cause brain cell swelling (the plasma osmolality is not
appropriately low,
Table 4).
Return to the bedside. The following major risk factors can be
anticipated for
developing brain swelling with acute hyponatremia. First, even
less electrolyte-
free water is needed to cause a lower PNa in patients with a
small muscle mass.
Second, patients who have a larger brain cell mass (younger age)
are at greater
risk from a given volume of water retained in the body. Third,
patients given anacute bolus of saline intravenously will have an
expanded blood volume (higher
hydrostatic pressure) and a lower colloid osmotic pressure.
Hence they might
have a higher intracerebral ECF volume and develop symptoms from
increased
intracranial pressure with a smaller reduction in their PNa.
Fourth, patients with an
underlying brain lesion (seizure disorder) may be more prone to
develop seizures
with a smaller degree of hyponatremia.
M.L. Halperin, D. Bohn / Crit Care Clin 18 (2002) 249272266
-
8/4/2019 desordenes de NA
19/24
It is said that young women are less able to regulate brain cell
volume in
response to acute hyponatremia [1]. This ides has arisen because
of pooroutcomes in young women compared with men who develop
postoperative
hyponatremia. Nevertheless, this is not a closed issue for two
reasons. First,
postoperative hyponatremia in males most frequently occurs
during transuretheral
resection of the prostate (TURP). Males undergoing TURP are
typically older and
could have a smaller brain cell/total intracranial volume.
Second, the composition
of the fluid retained with the commonest surgery in females and
males is
different electrolyte-free intravenous water after gynecological
surgery and
lavage solutions during a TURP (Table 4). During a TURP, acute
hyponatremia
may be due to the absorption of isotonic or half-iso-osmotic
lavage solutionscontaining glycine, sorbitol, and/or mannitol [12].
Neurological manifestations in
this setting might be due to toxic metabolic products such as
ammonium (NH4+)
produced during the metabolism of glycine rather than to brain
cell swelling. It
follows that one should not use aggressive therapy for this type
of acute
hyponatremia if the measured plasma osmolality is reduced by
less than 10%.
On the other hand, if the plasma osmolality is less than 260
mOsm/kg H2O,
therapy reverts to that described above for a gain of
electrolyte-free water.
Chronic hyponatremia (time course >48 hours)
Illustrative case 4
The usual diet of a 78-year-old, 60 kg, cheerful lady was tea (a
large cup),
toast, and jam. A thiazide diuretic was prescribed because of
the recent discovery
Table 4
Acute hyponatremia due to lavage solutions
EFW Lavage solution
Unit Original Final Original Final
Before the excretion of the organic solute
ICF volume L 20 22 20 20
ECF volume L 10 11 10 13
PNa mmol/L 140 127 140 108
Plasma osmolality mOsm/L 290 264 290 290
After the excretion of the organic solute (as 3 L of isotonic
urine)
ICF volume L 22 20
ECF volume L 11 10
PNa mmol/L 127 140
Plasma osmolality mOsm/L 264 290
Each subject with 30L of total body water has a 3L positive
water balance. The patient who
received the isosmotic lavage solution also has a positive
balance of 900 mOsm of a solute with a
distribution restricted to the ECF compartment. The plasma
osmolality is not depressed in the patient
who retained the isotonic lavage solution, and the ICF volume is
normal, despite a PNaof 108 mmol/L.
When the lavage solution is excreted as an isotonic solution,
there is a large increase in the PNa and no
change in the ICF volume.
M.L. Halperin, D. Bohn / Crit Care Clin 18 (2002) 249272 267
-
8/4/2019 desordenes de NA
20/24
of high blood pressure (160/90 mm Hg). She became lethargic and
slower in
mentation over several weeks, but there were no focal neurologic
signs. Blood
pressure fell to 140/90 mm Hg suggesting that her ECF volume was
contracted.Laboratory investigations are shown in Table 5.
We ask the reader the following questions: If an emergency is
present, what
is it? What dangers to you anticipate with therapy? On a
quantitative
analysis, what changes occurred in the volumes and electrolyte
composition in
her ICF and ECF compartments? What is the chronic therapy for
hypona-
tremia due to SIADH?
If an emergency is present, what is it?
Other physiology principles. Cardiac arrhythmias are more common
if hypo-
kalemia is severe in degree and if there is underlying heart
disease.
If KCl is given to treat hypokalemia, think of it as a form of
NaCl for the ECF
compartment because when K+ enters cells, Na+ (and H + ) will
exit cells for the
most part.
Return to the bedside. The major emergency to anticipate is
hypokalemia if it is
accompanied by prolonged QT interval in the EKG recording. The
absolute value
for her PNa, while alarming, should not be considered an
emergency. Because ofabsence of an ominous EKG, KCl was given
slowly to raise her PK to the low
3 mmol/l range over 24 hours. The oral route was used because
bowel sounds
were present. One cannot accurately predict how much of K+ will
be needed over
the next 24 hours, but we anticipated that at least 100 mmol of
KCl would be
required changes in her PK dictate the actual dose given.
Glucose and
bicarbonate containing infusions should not be given for fear of
an unwanted
acute shift of K+ into cells. Notwithstanding, there is a danger
with KCl
therapy too rapid correction of her hyponatremia. This can occur
for two
reasons. First, giving hypertonic KCl will raise her PNa and
thereby could lead totoo rapid a rise in PNa. Second, because K
+ will enter the ICF compartment and
Na+ will move in the opposite direction, the ECF volume will
expand. This in
turn could suppress the release of vasopressin and lead to the
excretion of a large
volume of dilute urine.
Table 5
Laboratory values in case 4
Parameter Unit Plasma Urinea
Na+ mmol/L 107 10
K+ mmol/L 2.2 25
Cl mmol/L 67 10
Glucose mg/dL (mmol/L) 90(5) 0
Urea mg/dL (mmol/L) 11(4) 320
Osmolality mOsm/kg H2O 220 402
a Random sample.
M.L. Halperin, D. Bohn / Crit Care Clin 18 (2002) 249272268
-
8/4/2019 desordenes de NA
21/24
What dangers do you anticipate with therapy?
Application of physiology principle 3. The physical examination
to detect amild degree of ECF volume contraction is not reliable
[4,24].
Return to the bedside. As discussed above, in the short-term,
there is a danger
that hyponatremia may be corrected too rapidly because of
suppression of the
release of vasopressin. As a result, a large water diuresis
could lead to a rapid
increase in PNa and cause the ODS. Clues suggesting that her ECF
volume
was low are found in the history (low-salt diet and the thiazide
diuretic). The
laboratory data are often difficult to interpret with respect to
the ECF volume
status. For example, some laboratory data did suggest that her
ECF volume
was contracted (urine Na+ and Cl concentrations were both <
15 mmol/l),
but these data are not entirely convincing in someone on a
low-salt diet who
should have a low electrolyte excretion rate. Other laboratory
values that may
be of help in this regard are a frankly high plasma urea (may
not be high
because of her low-protein diet), high level of creatinine (not
present because
of low muscle mass), metabolic alkalosis with hypokalemia
(present in this
case), and/or a plasma anion gap that is higher than expected
even when
corrected for albumin level [19].
There was a danger sign with therapy in this patient her urine
output rose
dramatically with an infusion of saline. Because this was a
water diuresis,
vasopressin was given to reduce the urine output temporarily so
that the desired
slow rate of rise in the PNa could be achieved (4 mmol/l/24 hour
because of her
K+ deficit) [2,22].
The main threat is brain cell volume shrinkage and the
development of an
ODS following therapy that resulted in too rapid a rise in the
PNa [21,35]. The
danger of ODS is greater in patients with a deficit of K+ and
those whose
nutritional state is poor [2,22] probably because they are
unable to regenerate
brain ICF particles quickly enough to prevent their cell volume
from shrinking.
In attempts to correct PNa of patients in this high-risk group,
the correction rate
should be much less than our usual recommendation of 8 mmol/l
per 24 hours
[25]. The PNa should rise at a rate that is slow enough to avoid
the ODS in
every patient. The emphasis should be on magnitude of correction
of hypona-
tremia, remaining within our 4 mmol/liter/24 hours [25]. Raising
the PNa above
125 mmol/l is rarely necessary in the first few days.
What changes occurred in her ICF and ECF compartment volumes
and composition?With a body weight of 60 kg, her normal total
body water (TBW) is close to
30 liters (50% of body weight distributed as 20 liters ICF and
10 liters ECF). If
there was no change in the number of osmoles in her ICF
compartment, the
calculated ICF volume with a PNa of 107 mmol/l is 26 liters
((140 mmol/l/
107 mmol/l) 20 liters). If her ECF volume was close to 10 liters
on admission,there was a negative balance of 330 mmoles of Na+ in
her ECF compartment
M.L. Halperin, D. Bohn / Crit Care Clin 18 (2002) 249272 269
-
8/4/2019 desordenes de NA
22/24
(fall in PNa of 33 mmol/l 10 liters). Because her plasma K+
concentration was
so low (2.2 mmol/l), her ICF compartment probably gained a
cation (Na + or
H+
). It is not possible at present to assign quantitative values
to these changesin ICF ion composition.
What is the chronic therapy with hyponatremia due to SIADH?
If the patient has an on-going defect in the excretion of
electrolyte-free water,
there are two options for therapy to prevent a further decline
in PNa. Either less
water must be consumed (water restriction) or the urine must be
large in volume
and isotonic to the intake. To lower the urine Na+ + K+
concentration, one can
ingest urea [6]; a typical dose for urea is 1030 g per day. If
the urine Na + + K+
concentration is very high, administration of a loop diuretic
can reduce theseconcentrations an isotonic level [7,17]. We do not
recommend the use of drugs
such as vasopressin antagonists because of the possibility of
causing a large water
diuresis and an excessively rapid rise in PNa.
Summary
Our purpose was to illustrate the utility of an approach that
begins with simple
principles of physiology to patients who have a disturbance in
salt and water
balance (Table 1). At times, the physiology is restricted to the
kidney and body
fluid compartments. In these settings, the goals of therapy are
defined by
calculating a tonicity balance electrolyte-free water balances
simply do not
provide the needed information [3]. At other times, performing
balances of other
solutes such as urea reveal that another critically important
problem is present
(tissue catabolism). Thus the physiologic analysis becomes more
integrative,
extending beyond renal issues. Goals for therapy become clearer
once the
integrative physiology is known.
More modern contributions from molecular studies permit a
revised interpre-
tation of the physiology. An example presented was the possible
role of
gentamicin-like drugs as a cause of high output renal failure
that is basically a
persistent loop diuretic-like effect.
In the patient presenting with hyponatremia, the first step is
to determine if
the time course is less than 48-hours because emergency therapy
is different in
this setting. With acute hyponatremia, the objective is to
diminish brain cell
swelling especially if even mild symptoms are present. In
contrast, the objective
in the patient with chronic hyponatremia is to prevent ODS. An
even slower
rate of rise of the PNa is required in patients who are
malnourished and/or
K+ depleted.
References
[1] Arieff AI. Hyponatremia, convulsions, respiratory arrest,
and permanent brain damage after
elective surgery in healthy women. N Engl J Med
1986;314:152935.
M.L. Halperin, D. Bohn / Crit Care Clin 18 (2002) 249272270
-
8/4/2019 desordenes de NA
23/24
[2] Bahr M, Sommer N, Peterson D, Wietholter H, Dichgans J.
Central pontine myelinolysis
associated with low potassium levels in alcoholism. J Neurol
1990;237:275 6.
[3] Carlotti APCP, Bohn D, Mallie J-P, et al. Tonicity balance
and not electrolyte-free water calcu-
lations more accurately guides therapy for acute changes in
natremia. Intensive Care Med2001;27:9214.
[4] Chung HM, Kluge R, Schrier RW. Clinical assessment of
extracellular fluid volume in hypo-
natremia. Am J Med 1987;83:9058.
[5] Davids MR, Edoute Y, Halperin ML. Approach to a patient with
acute polyuria and hyper-
natremia: A need for the physiologic approach of McCance at the
bedside. Netherlands J Med
2001;58:10310.
[6] Decaux G, Brimioulle S, Genette F, et al. Treatment of the
syndrome of inappropriate secretion
of antidiuretic hormone by urea. Am J Med 1980;69:99106.
[7] Decaux G, Waterlot Y, Genette F, et al. Treatment of the
syndrome of inappropriate secretion of
antidiuretic hormone with furosemide. N Engl J Med
1981;304:32930.
[8] Edelman IS, Leibman J, OMeara MP, et al. Interrelations
between serum sodium concentration,
serum osmolarity and total exchangeable sodium, total
exchangeable potassium and total body
water. J Clin Invest 1958;37:123656.
[9] Gamble JL, McKhann CF, Butler AM, et al. An economy of water
in renal function referable to
urea. Am J Physiol 1934;109:13954.
[10] Goldberg M. Hyponatremia. Med Clin North Am 1981;65:251
69.
[11] Gowrishankar M, Lenga I, Cheung RY, et al. Minimum urine
flow rate during water deprivation:
importance of the permeability of urea in the inner medulla.
Kidney Int 1998;53:15966.
[12] Hahn RG. The transurethral resection syndrome. Acta
Anaesthesiol Scand 1991;35:557 67.
[13] Halperin ML. The ACID truth and BASIC facts with a Sweet
Touch, an enLYTEnment. In:
Stirling, ON, Canada: RossMark Medical Publishers; 1997.
[14] Halperin ML, Goguen JM, Scheich AM, et al. Clinical
consequences of hyperglycemia and its
correction. In: Seldin DW, Giebisch G, editors. Clinical
disturbances of water metabolism. New
York: Raven Press; 1993. p. 24972.
[15] Halperin M.L, Goldstein MB. Fluid, electrolyte and
acid-base physiology; a problem-based
approach. Philadelphia: W.B. Saunders; 1998.
[16] Halperin M.L, Rolleston FS. Clinical detective stories: a
problem-based approach to clinical
cases in energy and acid-base metabolism. In: London, England:
Portland Press; 1993. p. 2734.
[17] Hantman D, Rossier B, Zohlman R, et al. Rapid correction of
hyponatremia in the syndrome of
inappropriate secretion of antidiuretic hormone. Ann Int Med
1973;78:8705.
[18] Jungas RL, Halperin ML, Brosnan JT. Lessons learnt from a
quantitative analysis of amino acid
oxidation and related gluconeogenesis in man. Physiol Rev
1992;72:41948.[19] Kamel KS, Cheema-Dhadli S, Halperin FA, et al.
Anion gap: do the anions restricted to the
intravascular space have modifications in their valence? Nephron
1996;73:3829.
[20] Labow BI, Souba WW. Glutamine. World J Surg 2000;24:1503
13.
[21] Laureno R, Karp BI. Myelinolysis after correction of
hyponatremia. Ann Int Med 1997;126:57 62.
[22] Lohr JW. Osmotic demyelination syndrome following
correction of hyponatremia: association
with hypokalemia. Am J Med 1994;96:40813.
[23] Mallie J-P., Bichet DG, Halperin ML. Effective water
clearance and tonicity balance: the ex-
cretion of water revisited. Clin Invest Med 1997;20:1624.
[24] McCance RA. Medical problems in mineral metabolism. III.
Experimental human salt defi-
ciency. Lancet 1936;230:823 30.
[25] Oh MS, Kim HJ, Carroll HJ. Recommendations for treatment of
symptomatic hyponatremia.Nephron 1995;70:143 50.
[26] Porzio P, Halberthal M, Bohn D, et al. Design of a
treatment for acute symptomatic hypona-
tremia: ensuring the excretion of a predictable amount of
electrolyte-free water. Crit Care Med
2000;28:1905 10.
[27] Robertson GL. Vasopressin. In: Seldin DW, Giebisch G,
editors. The kidney: physiology &
pathophysiology. Philadelphia PA: Lippincott Williams &
Wilkins; 2000. p. 113352.
M.L. Halperin, D. Bohn / Crit Care Clin 18 (2002) 249272 271
-
8/4/2019 desordenes de NA
24/24
[28] Rose BD. New approach to disturbances in the plasma sodium
concentration. Am J Med 1986;
81:103340.
[29] Sands JM, Layton HE. Urine concentrating mechanism and its
regulation. In: Seldin DW,
Giebisch G, editors. The kidney: physiology &
pathophysiology. Philadelphia PA: LippincottWilliams & Wilkins;
2000. p. 1175216.
[30] Soroka SD, Chayaraks S, Cheema-Dhadli S, et al. Minimum
urine flow rate during water
deprivation: importance of the urea and non-urea osmole
concentration and excretion rate. J
Am Soc Nephrol 1997;8:8806.
[31] Soupart A, Decaux G. Therapeutic recommendations for
management of severe hyponatremia:
current concepts on pathogenesis and prevention of neurologic
complications. Clin Nephrol
1996;46:14969.
[32] Spira A, Gowrishankar M, Halperin ML. Factors contributing
to the degree of polyuria in a
patient with diabetes mellitus in poor control. Am J Kidney Dis
1997;30:82935.
[33] Spital A, Sterns RD. The paradox of sodiums volume of
distribution: Why an extracellular
solute appears to distribute over total body water. Arch Intern
Med 1989;149:12557.
[34] Steele A, Gowrishankar M, Abrahmson S, et al. Postoperative
hyponatremia despite isotonic
saline infusion: A phenomenon of desalination. Ann Int Med
1997;126:205.
[35] Sterns RH, Silver SM, Spital A. Hyponatremia. In: Seldin
DW, Giebisch G, editors. The
kidney: physiology & pathophysiology. Philadelphia PA:
Lippincott Williams & Wilkins;
2000. p. 121738.
[36] Welt LG, Seldin DW, Nelson WP, et al. Role of the central
nervous system in metabolism of
electrolytes and water. Arch Int Med 1952;90:35578.
M.L. Halperin, D. Bohn / Crit Care Clin 18 (2002) 249272272