Embed Size (px)
Citation preview

CONGRESSO FUNDACIONAL DE LA
SOCIEDAD ESPAŇOLA DEL ACCESO VASCULAR
SEDAV Madrid 7-8 Noviembre 2014
MICROCIRURGIA y HEMOSTASIA PREVENTIVA
Nicola Pirozzi
Roma
www.nefrologiainterventistica.com
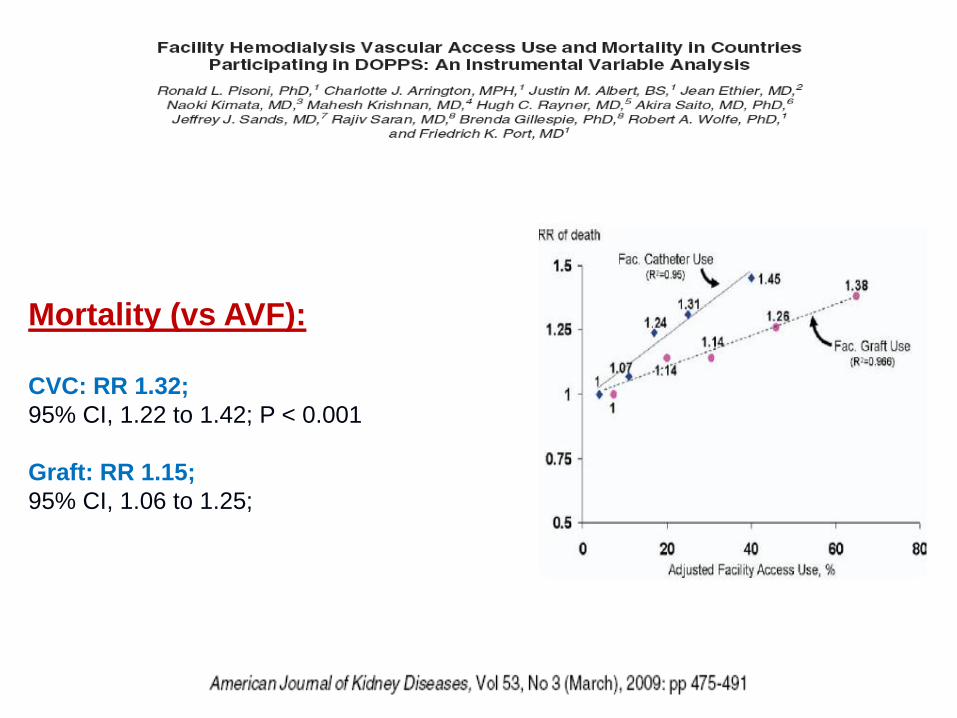
Mortality (vs AVF):
CVC: RR 1.32;
95% CI, 1.22 to 1.42; P < 0.001
Graft: RR 1.15;
95% CI, 1.06 to 1.25; P < 0.001
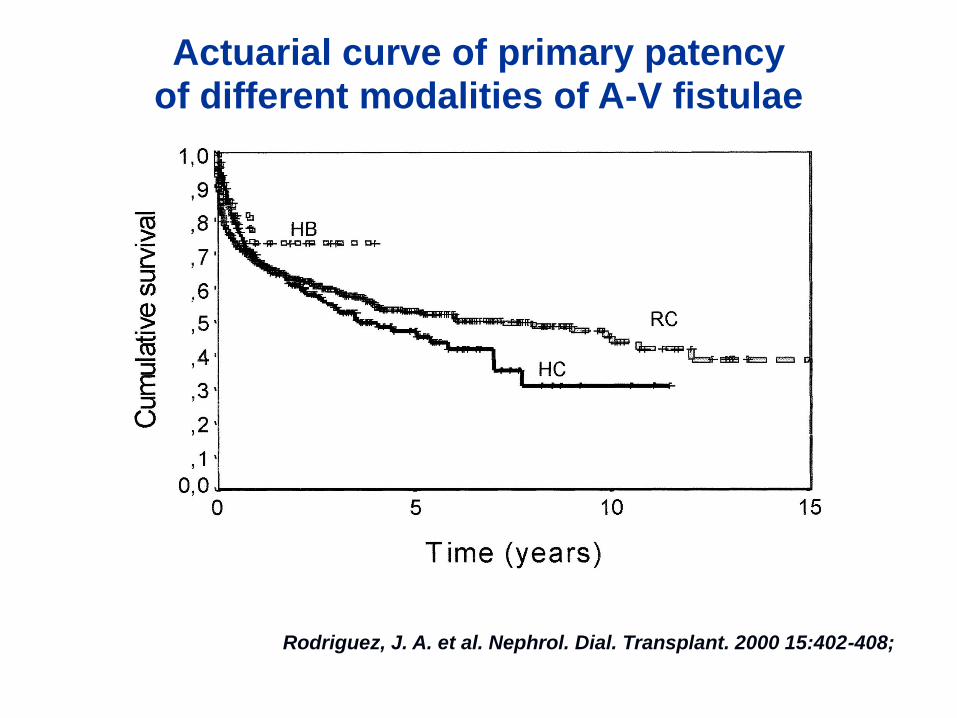
Rodriguez, J. A. et al. Nephrol. Dial. Transplant. 2000 15:402-408;
Actuarial curve of primary patency of different modalities of A-V fistulae

Modified from L.Turmel Rodrigues, Marseille 2012, http://www.sfav.org/Publication/SFAV2012/002.pdfModified from L.Turmel Rodrigues, Marseille 2012, http://www.sfav.org/Publication/SFAV2012/002.pdf
AUTOLOGOUS ARTERIO-VENOUS FISTULA (AVF)
78.5% OF PREVALENT PTS IN ITALY
Distal AVF 88%
Proximal AVF 12%
Elderly, diabetic and dialysis vintage >10y included
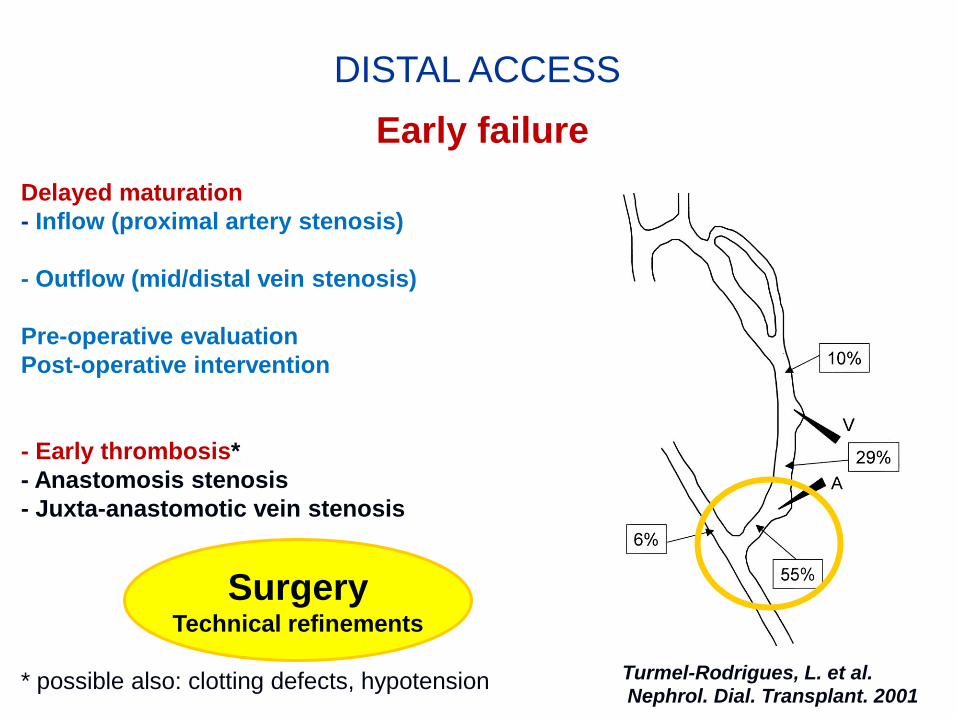
DISTAL ACCESS
Early failure
Delayed maturation
- Inflow (proximal artery stenosis)
- Outflow (mid/distal vein stenosis)
Pre-operative evaluation
Post-operative intervention
- Early thrombosis*
- Anastomosis stenosis
- Juxta-anastomotic vein stenosis
* possible also: clotting defects, hypotension Turmel-Rodrigues, L. et al. Nephrol. Dial. Transplant. 2001
Surgery Technical refinements
DISTAL ACCESS SURGERY
Microsurgery:
Magnification of images (loop glasses, operating microscope)
Dedicated instruments (pince, forcep, needelholder, clamp)
Sutures: poliamide – polipropilene (8-0, 9-0..12-0)
Preventive haemostasis
Pneumatic tourniquet
- Operative field visualisation
- Sharpness of procedures
- Reduced vascular traumatism
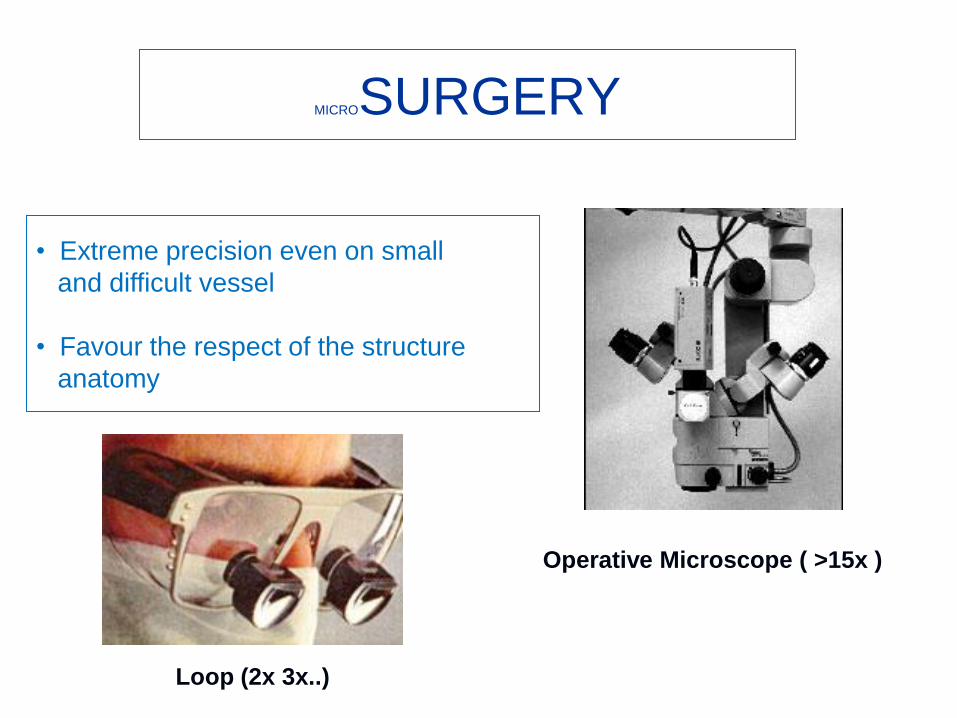
MICROSURGERY
• Extreme precision even on small
and difficult vessel
• Favour the respect of the structure
anatomy
Loop (2x 3x..)
Operative Microscope ( >15x )

MicroSurgery
- Intima respect
- Sharp artery /vein wall apposition
- Avoiding adventitial “infiltration”
- Valvulectomy
- Avoiding twisting, kinking, narrowing …
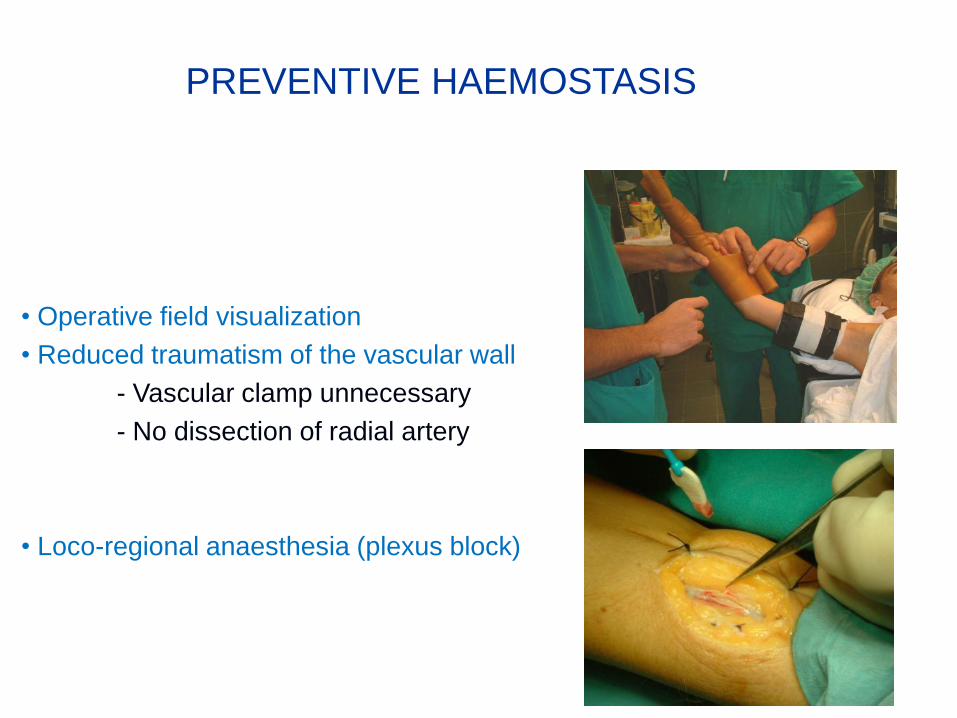
• Operative field visualization
• Reduced traumatism of the vascular wall
- Vascular clamp unnecessary
- No dissection of radial artery
• Loco-regional anaesthesia (plexus block)
PREVENTIVE HAEMOSTASIS
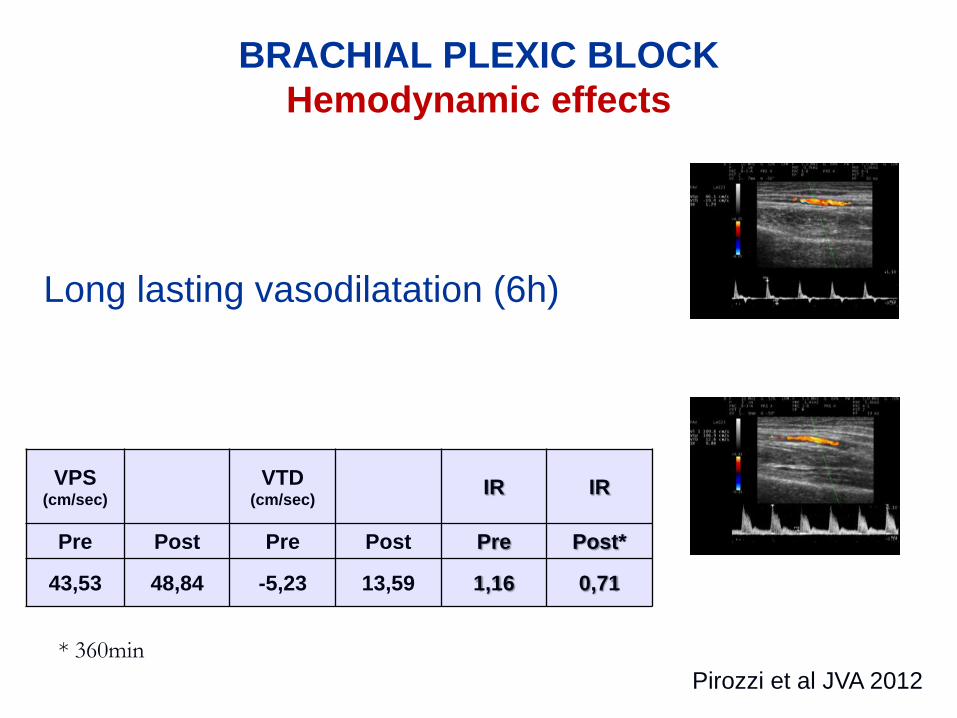
BRACHIAL PLEXIC BLOCK
Hemodynamic effects
VPS (cm/sec)
VTD (cm/sec)
IR IR
Pre Post Pre Post Pre Post*
43,53 48,84 -5,23 13,59 1,16 0,71
Pirozzi et al GIN 2010 (27) S51 Pirozzi et al JVA 2012
* 360min
Long lasting vasodilatation (6h)
evidence based medicine
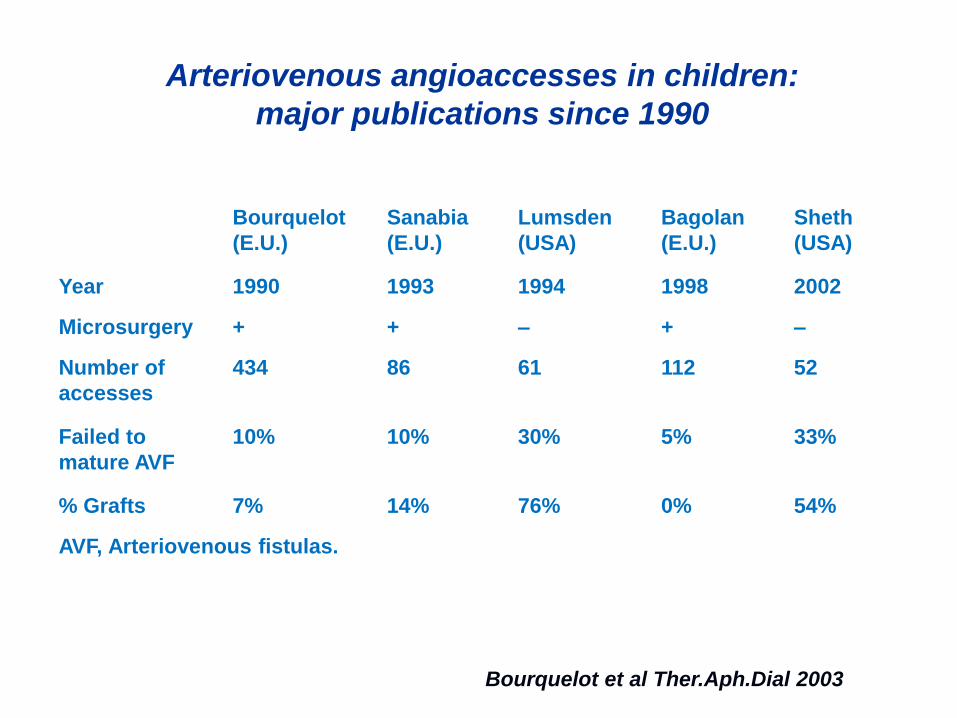
Arteriovenous angioaccesses in children:
major publications since 1990
Bourquelot
(E.U.)
Sanabia
(E.U.)
Lumsden
(USA)
Bagolan
(E.U.)
Sheth
(USA)
Year 1990 1993 1994 1998 2002
Microsurgery + + – + –
Number of
accesses
434 86 61 112 52
Failed to
mature AVF
10% 10% 30% 5% 33%
% Grafts 7% 14% 76% 0% 54%
AVF, Arteriovenous fistulas.
Bourquelot et al Ther.Aph.Dial 2003
MICROSURGERY
Adults: still an open debate
“…there are two different “schools of thinking”.
http://www.vascularaccesssociety.com
Guidelines: Create forearm A/V_fistula
RCT lack
EBPG KDOQI guide-lines: no mention about technique
Emerging evidence:..
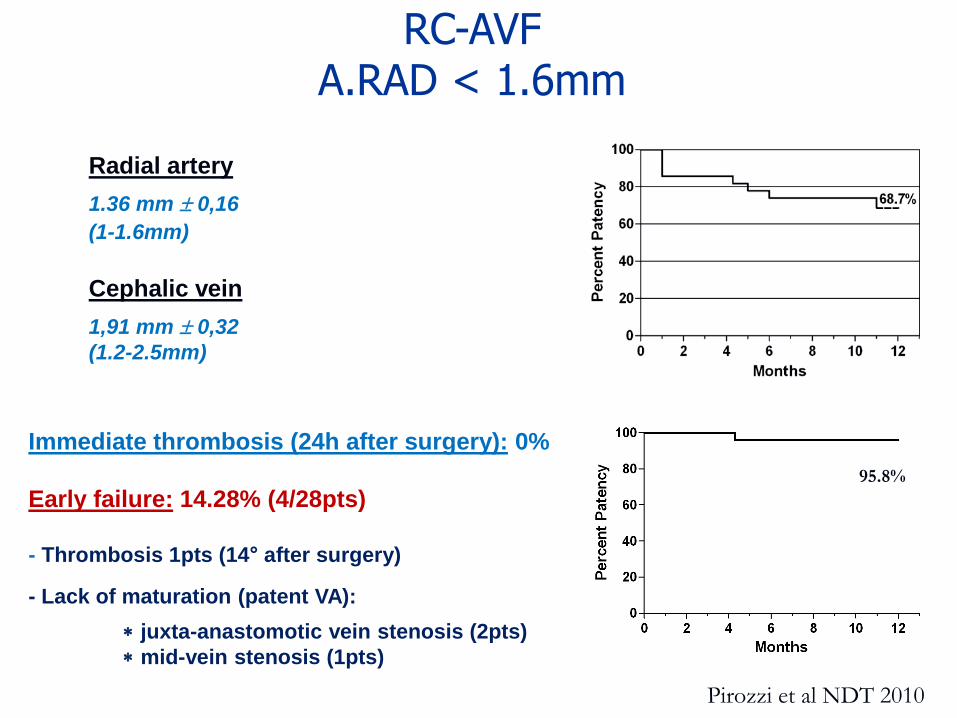
Immediate thrombosis (24h after surgery): 0%
Early failure: 14.28% (4/28pts)
- Thrombosis 1pts (14° after surgery)
- Lack of maturation (patent VA):
juxta-anastomotic vein stenosis (2pts)
mid-vein stenosis (1pts)
95.8%
Pirozzi et al NDT 2010
RC-AVF A.RAD < 1.6mm
Radial artery
1.36 mm 0,16
(1-1.6mm)
Cephalic vein
1,91 mm 0,32
(1.2-2.5mm)
Bourquelot et al JVS 2011
UB-AVF
70 pts (63 adult, 7 children)
Immediate success
94% (adults)
100% (children)
- In use access 60% after 80 days
- 1y PP 42%
- 1y SP 60%
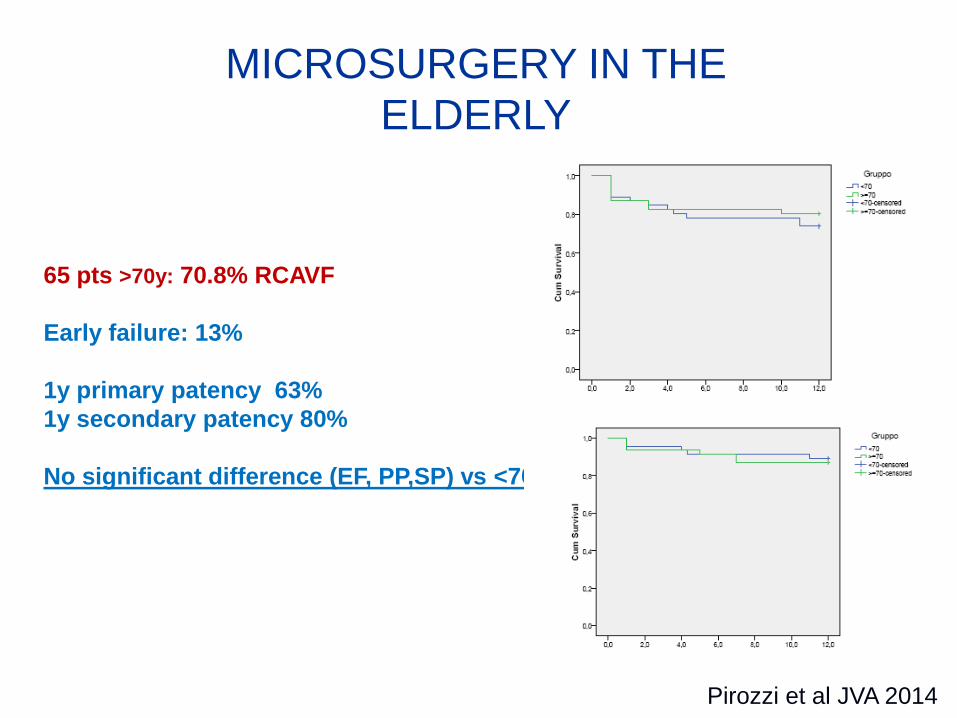
65 pts >70y: 70.8% RCAVF
Early failure: 13%
1y primary patency 63%
1y secondary patency 80%
No significant difference (EF, PP,SP) vs <70y pts
MICROSURGERY IN THE
ELDERLY
Pirozzi et al JVA 2014
MICROSURGERY = PATENT DISTAL ANASTOMOSIS
then
Multidisciplinary approach => help functional/patency
- OBESITY:
Lipectomy Bourquelot et al JVS 2009
- FOREARM ARTERY STENOSIS:
PTA Turmel Rodrigues NDT 2009 Raynaud et al JVS 2009
- IUXTA-ANASTOMOTIC VEIN STENOSIS:
Proximalisation / PTA Tessitore Clin J Am Soc Nephrol 2006, Long B et al JVS 2010
- MID-VEIN / OUTFLOW VEIN STENOSIS:
PTA +/- stenting Turmel Rodrigues et al NDT 2001, Nat Clin Pract Neph 2008
Multidisciplinary approach => help functional/patency
CONCLUSIONS
-The main challenge of distal anastomosis is the deal with small, thin,
fragile vessels.
Calcifications: sometimes impossible to create any anastomosis
- No definitive validation of any surgical procedure
- Microsurgery (and preventive haemostasis) seem to match
the needs of a correct surgical procedure able to lead to a patent
anastomosis
- Consistent results on children, emerging evidence on adults
CONCLUSIONS
- Cardiovascular and plastic reconstructive surgery moved to
microsurgical techniques long time ago (facing the same vessels)
- It is time to such a change in practice even for vascular access surgery?
- More evidence would be provided, stronger conclusion could be drawn

Muchas gracias
et SUERTE a la SEDAV!!
Nicola Pirozzi
[email protected] www.nefrologiainterventistica.com
Pirozzi et al GIN 2010 (27) S51
VIDEO 1
PREVENTIVE HAEMOSTASIS
CREATION: UB-AVF
Pirozzi et al GIN 2010 (27) S51
VIDEO 2
MICROSURGERY (Courtesy of Dr. Pierre Bourquelot)
Pirozzi et al GIN 2010 (27) S51
VIDEO 3
PREVENTIVE HAEMOSTASIS:
SUPERFICIALISATION BY LIPECTOMY