Embed Size (px)
Citation preview

j. max.-fac. Surg. 10 (1982) 229
J. max.-fac. Surg. 10 (1982) 229-235 © 1982 Georg Thieme Verlag Stuttgart • New York
Oral Leiomyomas Frans R. Praal, Charis A. Ioannides, Gert Jan van Beek, Fred van de Molengraft
Department of Oral and MaxiUofaciai Surgery (Head: Prof. C. A. Merkx, D.M.D., since 1-11-1979 Prof. Dr. H. P. M. Freihofer, M.D., D.M.D.) Department of Pathology (Head: Prof. Dr. P. H. M. Schillings, M.D. and Prof. Dr. G.P. Vooys, M.D.)
Summary
Three cases of oral leiomyoma and a review of the literature of oral leiomyomas are presented. Differenti- ation between leiomyoma, other spindle cell tumours and leiomyosarcoma is discussed. Emphasis is placed on the necessity to section the specimen completely.
Key-Words
Leiomyoma - Leiomyosarcoma - Spindle cell tumour
Introduction
Leiomyoma, a benign turnout of smooth muscle origin, usually develops in the uterus, gastrointestinal tract and skin. The tumour is not commonly found outside these regions and can be considered rare in the oral cavity. The first case of an oral leiomyoma was described by Blanc in 1884. Since then several reports have been made (Ta- ble 1). The aim of this paper is to present three case reports of leiomyomas from the files of the Department of Pathol- ogy, University of Nijmegen, and to correct and complete the review of the literature, presented by Ravindranathan and Heslop in 1979. The leiomyoma is a slow-growing, firm, elastic asymptoma- tic turnout. Its colour varies from bluish purple to grey- white, depending on the vascularity. The size varies from a few millimetres to three centimetres. Clinically it is difficult to differentiate the tumour from other mesenchymal tumours, such as fibroma, neurofibroma, lipoma, mucocoele or its malignant counterpart the leiomyosar- coma. The origin of this turnout in the oral cavity is unknown, but suggestions as to sources of smooth muscles are: 1 Tunica media of the blood vessel wall (Stout, 1938) 2 Papillae circumvallatae of the tongue (Garrett, 1909)
3 Ductus lingualis (Glas, 1905) 4 Heterotopic embryonic muscle tissue (Utz, 1965)
Review of the literature
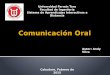
Seventy-two cases have been reported (Table 1). The most common sites of this lesion in the oral cavity are palate and tongue (Fig. 1). Two of the reported lesions of the cheek were supposed to have developed from epithelium of the hair follicle and were not primarily intra-oral.
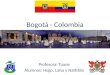
The leiomyomas are usually asymptomatic. However, three lesions of the tongue, reported by Blanc (1884), Bertelli (1965) and one of our cases, were painful. A few peculiar symptoms were: change of the patient's voice (Blanc, 1884), sore throat ( Glas, 1905; Stout, 1938) and limited opening of the mouth (Frenkel, 1965). The patient's ages varied from 31/2 to 85 years old, with an average of 42.7 years (Fig. 2). No sex predilection was observed. Recurrences after local excision are rarely seen: only three cases have been reported (Sehrt, 1907; Stout, 1938; Bur- ford et al., 1944), which were all of the vascular type.
TONGUE
CHEEK
PALATE ~- HARD PALATE . . . .
L SOFT PALATE
UVULA
FLOOR OF MOUTH
f LIP
LIPS UPPER LIP
LOWER LI P
ANT. MAND. MUCO-BUCCAL FOLD
GtNGIVA
PAROTID SALIVARY GLAND
LINGUAL POUCH (M3)
SUBMANDIBULAR SALIVARY GLAND . . . .
MAXILLARY TOOTH SOCKET
CENTRAL MANDIBULA
6 9
5 7
1 5 8
t
1
: 2 1
3
2 2 3
1 2 3
2 1
1
1
Fig. 1 Site and sex distribution for oral 1 2 3 4 5 6 7 8 9 1 0 1 1 1 2 1 3 1 4 1 5 leiomyomas: 72 cases

230 J. max.-fac. Surg. 10 (1982) F. R. Praal et al.
Table 1 Previously recorded leiomyomas (intra-oral localization). This table compared to that published by Ravindranathan and Heslop, 1978 adds five missed and ten new cases and omits one case, because of its extra-oral localization and corrects information concerning sex and site of the lesions. For further explanation see discussion and conclusion.
Author Year Age Sex Site
Blanc 1884 33 M Tongue Herzog 1898 45/50 M Cheek Fein 1905 26 F Palate Glas 1905 44 M Tongue Sehrt 1907 Child M Cheek Well 1914 69 M Uvula Peter 1937 40 F Floor of the mouth Stout 1938 50 M Tongue Stout 1938 29 M Tongue Burford et al. 1944 32 M Floor of the mouth Abulafia and Grinspan 1956 48 F Cheek Duhig and Ayer 1959 ? ? Lower lip Duhig and Ayer 1959 ? ? Lower lip Yannopoulos and Stout 1962 11 ? Buccal mucosa Yannopoulos and Stout 1962 41/2 F Tongue Kohn et al. 1963 ? ? Palate Watabe and Morishima 1963 Infant F Tongue Kist and Bhaskar 1964 58 M Palate Lucas 1964 12 M Gingiva Hagy et al. 1964 76 F Lip Bianchi 1964 48 F Cheek Bertelli 1965 43 M Tongue Utz 1965 29 F Gingiva Frenkel t965 13 M Cheek Merrill and Downs 1967 72 M Tongue Merrill and Downs 1967 76 M Cheek (2 x ) Collins and Elzay 1968 56 M Upper lip Manhold and Doyle 1968 70 M Cheek Pindborg 1968 50 M Hard palate MacDonald 1969 44 M Upper lip MacDonald 1969 11 F Tongue Garrett 1969 65 F Hard palate McGowan and Jones 1969 48 F Lower lip McGowan and Jones 1969 54 M Upper lip Colangelo and Benagiano 1969 ? ? Parotid salivary gland Weisinger et al. 1969 59 F Lingual gingiva Weisinger et al. 1969 61 M Tongue Costas and Curuchaga 1970 31 F Cheek Papadrianos 1971 55 F Tongue Brizuela et al. 1972 28 F Hard palate Cherrick et al. 1973 53 M Palate Cherrick et al. 1973 53 M Lower buccal sulcus Cherrick et al. 1973 56 M Palate Cherrick et al. 1973 47 M Palate Cherrick et al. 1973 28 F Palate Cherrick et al. 1973 24 M Lingual pouch Cherrick et al. 1973 24 M Lower labial sulcus Gutmann et al. 1974 73 M Hard palate Gutmann et al. 1974 ? F Lower lip Galili and Shteyer 1974 69 F Soft palate Farman 1975 6 F Tongue Farman 1975 52 M Tongue Farman 1975 ? M Lower lip Farman 1975 Adult M Lower lip Farman 1975 6 F Submand. salivary gland Rao and Venkateswarlu 1975 23 F Buccal gingiva M3 region Rhatigan and Kim 1976 71 F Maxillary tooth socket Gombos et al. 1976 ? F Floor of the mouth Kelly and Harrigan 1977 28 M Tongue Reichart and Reznik-Sch011er 1977 51 F Cheek Goldblatt and Edesess 1977 3~/2 F Central mandible Ravindranathan and Heslop 1978 85 M Cheek Nakamura et al. 1978 ? F Palate Nakamura et al. 1978 ? M Palate

Oral Leiomyomas J. max.-fac. Surg. 10 (1982) 231
Author Year Age Sex Site
Datum and Neville 1979 47 M Damm and Neville 1979 42 F Damm and Neville 1979 28 F Davis 1980 62 M Masuda et al. 1980 33 M Praal et al. 1982 72 M Praal et al. 1982 18 F Praal et ai. 1982 14 F
Ant. mand. muco-buccal fold Ant. mand. muco-buccal fold Ant. mand. muco-buccal fotd Hard palate Lower lip Cheek Cheek Tongue
age distrubution, by sex,of the oral leiomyomas (60 cases)
n u m b e r of cases
lO
8
6
L
• total
[ ] male
female
L 1-10 11-20 21-30 31-40 41-50 51-60 61-70 71-80 81-90
age
Fig. 2 Age distribution, by sex, of the oral leiomyomas (60 cases). (12 cases were left out, because the ages were unknown.)
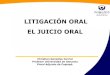
Fig. 3 Case 1. Nuclear palisading in a vascular leiomyoma. Cellu- larity is moderate. Capillaries are sparse. HE; x 130
Case Descriptions Case 1 An 18-year-old Caucasian woman presented with an eight- months-old painful, slow growing tumour of the cheek. The examination revealed a firm elastic mass with a diame- ter of 1.5 cm., painful on palpation. The overlying mucosa had a normal appearance. General medical examination revealed no pathology. The tumour was excised under local anaesthesia. The lesion was found to be well demarcated. Healing was uneventful. After a 2 year follow-up without recurrence the patient was lost to further routine examination. Histopathology - Macroscopic: Hazelnut-size with a cap- sule, pale on cross-section. Microscopic - Tumour, composed of cells with oval nuclei which showed a fine chromatin structure and differing in size. The cells were elongated and formed bundles with local signs of whorling. An orderly pattern could nowhere be recognised. No mitoses were seen (Fig. 3). Hardly any collagen was found with the Van Gieson staining technique. Collagen could be seen with the AZAN-stain. Conclusion: Vascular leiomyoma, well demarcated. No signs of malignancy.
Case 2 A 72-year-old man was sent by his general practitioner for examination of a swelling in the left cheek. The mass had been present for more than two years, increasing very slowly in size. Extraoral examination revealed no pathological signs. Intraorally there was a 2.5 by 1.5 cm. hard, sessile, mobile tumour in the left cheek (Fig. 4 a). The mucosa covering the swelling was whitish. The patient was edentulous and no other abnormalities could be seen. There was no regional lymphadenopathy and no disturbed sensation in the lower lip and cheek. The diagnosis of fibroma or a minor salivary gland tumour was considered. The lesion was excised under local anaesthesia. Clinically, it was surrounded by a thin capsule. The wound was closed in layers and the postoperative course was uneventful. The patient has been followed-up for 11/2 years. No recur- rence has been noted up to now. Histopathology - Macroscopic: A firm round mass, at one side covered with mucosa, 11/2 cm. in diameter. Microscopic - The tumour was well circumscribed and totally surrounded by a scant amount of fibrous connective tissue. The surface was covered with an intact stratified squamous epithelium, focally demonstrating orthokeratosis (Fig. 4 b). The lesion itself consisted of bundles of longitudi- nal and transverse intertwining cells.

232 J. max.-fac. Surg. 10 (1982) F. R. Praal et al.
Fig. 4 Case2
Fig. 4 a The tumour located in the left cheek. The whitish colour of the covering mucosa clearly visible.
Fig. 4 b The intact stratified squamous epithelium demonstrates focal orthokeratosis. The tumour is well circumscribed and sur- rounded by a scant amount of fibrous connective tissue, HE; x 150
Fig. 4 c Cell-rich region. The arrow indicates a mitosis. HE; × 480 Fig. 4 d The focally thick walled channels are diffusely arranged and sometimes irregularly shaped. HE; x 96

Oral Leiomyomas J. max.-fac. Surg. 10 (1982) 233
Fig. 5 Case 3. Moderate cell-rich vascular leiomyoma. Spindle cells are arranged in whorls. HE; x 130
Some collagen between these cells was seen. The generally fusiform nuclei had blunt ends. Mitoses were found espe- cially in the more cell-rich regions (Fig. 4c), where the nuclei sometimes showed slight hyperchromasia (average mitotic-rate: 1.5 per 10 HPF). The Elastica Van Gieson stain was positive for smooth muscle. Within this lesion several diffusely arranged, sometimes irregularly shaped and focally thick-walled vascular channels, also consisting of smooth muscle cells, were found (Fig. 4 d). Focally ery- throcytes were present in the vascular lumina, where the endothelial lining cells demonstrated no atypia. Conclusion: Vascular leiomyoma.
Case 3 A 14-year-old, white female was referred by her house physician, to the department of general surgery (Head Prof. Dr. W. Schmidt and Prof. Dr. H. de Boer) for examination of a swelling in the distal part of her tongue. The enlarge- ment was reported to have been present for one year. On examination, a slow growing tumour of the tongue was noted. Its size was 1.4 cm. by 1 cm. approximately. The lesion appeared well circumscribed, smooth-surfaced and firm-elastic in consistency. The tumour was not fixed to the deeper layers of the tongue and the overlying mucosa appeared normal. General medi- cal examination revealed no further pathology. The tumour was excised under local anaesthesia and the wound was closed. Healing was uneventful. One year postoperatively no recurrence was apparent. No further follow-up was possible since the patient did not return to our clinic, despite numerous attempts to contact her. Histopathology - Macroscopic: The specimen measured 1.4 cm. by 1 cm.
Microscopic - The tumour was a well circumscribed lesion, surrounded by loose, vascular fibrous connective tissue with striated muscle present in the base of the specimen. The tumour consisted of whorls of cells with pale-staining blunt-ended nucle~ and long cytoplasmic extensions. No mitotic figures were found (Fig. 5). The Van Gieson staining technique was positive for bundles of well differentiated smooth muscle elements. Conclusion: Vascular leiomyoma of the tip of the tongue. No signs of malignancy.
Discussion and Conclusion
Leiomyoma can be considered rare in the oral cavity. Farman and Kay (1977) found a percentage of 0.064% of oral leiomyomas in relation to leiomyomas of the whole body. In our study, oral leiomyomas constitute 0.42% of the benign tumours of the soft tissue of the oral cavity, col- lected in the same period. In contrast to this, the percentage of oral lipomas in relation to all benign oral soft tissue tumours from the study of De Visscher (1982) is 2.4%. We have updated the tabel of Ravindranathan and Heslop (1978). One of these cases is omitted because of its extra- oral situation (Pettini, 1965). We have added five cases which are not mentioned by Ravindranathan and Heslop (1978) and had been reported before 1978 (Pindborg, 1968; Weisinger et al., 1969; Brizuela et al., 1972; Rao and Venkateswarlu, 1975; Gombos et al., 1976). Since then, seven more cases have been reported and these are also added to the modified list. We have now presented three more cases. With this paper we increase the present number of published oral leiomyomas by 24%. Contrary to previous reviews, we conclude a predilection of oral leiomy- omas for women under 30 years of age and for men over 30 years old. The paucity of smooth muscle tumours found in the oral cavity may be due to the relatively small amount of smooth muscle in this cavity. The main sources of smooth muscle in the mouth are the blood vessel walls. Therefore it would seem logical to conclude, that the majority of oral leiomyo- mas will be vascular. Duhig and Ayer (1959) suggest, that the vascular leiomyo- ma is only one stage in a developing process of smooth muscle proliferation: Haemangioma, angioma, vascular leiomyoma and solid leiomyoma. If this were true, one would expect the mean age to be younger (Farman, 1975). Certain leiomyomas of the cheek may be derived from smooth muscle associated with hair follicles and are there- fore not primarily intraoral. Some authors suggest that the leiomyomas of the tongue arise from the muscle in circumvallate papillae or ectopic thyroglossal tissue. Shafer et al. (1974) stated, that smooth muscle tissue is an inconstant finding in the circumvallate papillae of the tongue. Kist and Bhaskar (1964) stated that the paucity of smooth muscle tissue in the oral cavity cannot be considered the only reason for the rarity of oral leiomyomas. The tissue of tongue, cheek, lip and soft palate consists for a considerable part of striated muscle. Yet the rhabdomyoma and rhab- domyosarcoma are tumours almost as rare as the leiomyoma. Intra-uterine leiomyomas are oestrogen dependent (Bells et al., 1979). However, the male-female ratio of 1 : 1 for

234 J. max.-fac. Surg. 10 (1982) F .R . Praaletal .
intra-oral le iomyomas indicates that there is no hormonal influence. According to the W.H.O. classification we have to deal with three types of leiomyomas: - Leiomyoma (solid) -Angiomyoma (vascular leiomyoma) -Epithelioid le iomyoma (leiomyoblastoma)
The reported cases from the oral cavity are solid and vascular. Only one case, reported by Hagye t al., (1964) is a leiomyoblastoma. Microscopical ly the solid le iomyoma is composed of bun- dles of intertwining spindle cells with a varying amount of collagen. The collagen can become so prominent , that the true nature of the lesion is obscured (Enzinger et al., 1969). The muscle nuclei are generally elongated, pale-staining and blunt-ended. The bundles of fibres usually form whorls, because of the fibres being cut in different planes. Intracytoplasmic myofibrils can be demonstrated. Mitoses are usually scarce. The vascular le iomyoma is composed of a tor tuous mass of thick-walled blood vessels in among intertwining bundles of smooth muscle. Stout (1938) could not identify the vessel as a vein or artery. Janssen (1952) detected a vessel containing a valve in the tumour. In our second case the walls of the vascular chan- nels were focally thickened. We could not identify any vessel containing valves. The le iomyoblas toma has rounded or polygonal cells rather than the elongated, blunt ended, differentiated leiomyoblast ; the cytoplasm is acidophilic. Smooth muscle fibres are rarely found. Sometimes it is difficult to differentiate a le iomyoma from a neurof ibroma or other spindle cell tumour, such as spindle cell p leomorphic carcinoma. The le iomyoma can have areas of acellular connective tissue and areas of palisading, and is easily confused with neuri lemmoma. Proper diagnosis is possible with the PTAH-staining ( = Mal lory ' s phosphotungst ic acid haematoxylin) , Masson ' s t r ichrome and Van Gieson's staining technique. In Masson ' s t r ichrome staining, the smooth muscle stains red and the collagen fibres stain green or blue. The Van Gieson's stain is recommended as a good screening stain for muscle tissue, but often gives a false positive reaction (Damm and Neville, 1979). In order to prove the existence of muscle, the PTAH-staining technique for myofibrils should be used. It is sometimes difficult to differentiate the le iomyoma from its malignant counterpar t , the le iomyosarcoma. The characteristic histological features are high mitotic activity, cellular p leomorphism, hyperchromatism, lack of pa l i sading of nuclei, bizarre cell forms and lack of myofib- rils. It is suggested, that the finding of mitoses is the most impor tant feature in recognizing a le iomyosarcoma (Kim- braugh, 1920; Stout, 1962). Mos t investigators state that, if less than two mitoses per ten high power fields are found, the prognosis is to be called good (Gorlin and Goldman, 1970; Batsakis, 1974; Reichart and Reznik-SchiilIer 1977). The counting of mitoses cannot always be taken as a reliable feature in differentiating between benign and malig- nant lesions. There are some reports of smooth muscle turnouts that did not show more than an average number of mitoses, but invaded locally or metastasized to lymph nodes
or bones (Stout and Hill, 1958; Miles and Waterhouse, 1962). Furthermore, 20% of the intra-oral smooth muscle tumours are mal ignant (Farman and Kay, 1977). This is a higher incidence of malignancy than for similar tumours in other sites of the body (Robinson and Wbyte, 1978). There- fore we emphasize the necessity of complete sectioning of the specimen, because sarcomatous changes may appear only in a certain par t of the tumour.
Addendum: Since the writing of this article one more case of oral leiomyoma has been reported. (Giles A. D., Gosney M. B. E.: Oral Angiomyoma, a case report. Br. J. Oral Surg. 20 (1982) 142).
Acknowledgement The authors are deeply grateful to Dr. M. P. van Beek, M. D. (Department of Pathology) and to Miss W. G. A. Karnphuis for their help and advice.
References Abulafia, J., D. Grinspan: Leiomiomas de la piel, con especial referen-
cia alas formas solitarias. Arch. Argent. Derm. 6 (1956) 1 Batsakis, J. G.: Tumours of the head and neck. Williams and Wilkins.
Baltimore 1974 Bells, J. A., G. I. Post, S. C. Rochman, D, F. Milam: Genitourinary
leiomyomas. Urology 13 (1979) 424 Bertelli, A. de P.: Uncommon tumours of the tongue. Oral Surg. Oral
Med. and Oral Path. 19 (1965) 771 Bianchi, H.: D'Etude d'un liomyome de la jour. Hospital Rio 66
(1964) 1319 Blanc, E.: Contribution ~t l'6tude des tumeurs fibreuses de la langue.
Gaz. Hebdomad. de M~d. et de Chir. 21 (1884) 611 Brizuela, A. F., L Lewin, T. Ferrario: Leiomioma bilateral en paladar
duro. Trib. Odont. (C. B. Aires) 56 (1972) 274 Burford, W. N., L. V. Ackerman, H. B. Robinson: Leiomyoma of the
tongue. Am. J. Orthod. (Oral Surg.) 30 (1944) 395 Cherrick, H. M., C. L. Dunlap, O. H. King: Leiomyomas of the oral
cavity J. Oral Surg. 35 (1973) 54 Colangelo, G., E. Benagiano: Su alcuni particolari aspetti
istopatologici dei tumori angiomatosi del caro orale. Ann. Stomat. (Roma) 18 (1969) 507
Collins, L. R., R. P. Ehay: Leiomyoma of the oral cavity: report of a case. J. Oral Surg. 26 (1968) 142
Costas, J, B., E. Curuchaga: Leiomyoma de la cavidad bucal. Ann. Esp. Odont. 29 (1970) 385
Datum, D. D., B. W. Neville: Oral leiomyomas. Oral Surg. 47 (1979) 343
Davis, G. B.: Angiomyoma of the palate. Int. J. Oral Surg. 9 (1980) 484
Duhig, J. T., J. P. Ayer: Vascular leiomyoma. Arch. Pathol. 68 (1959) 424
Enzinger,, F. M., R. Lattes, H. Torloni: Histological Typing of Soft Tissue Tumours. World Health Organisation, Geneva 1969 pp. 30
Farman, A. G.: Benign smooth muscle tumours. S. Afr. Med. J. 49 (1975) 13
Farman, A. G., S. Kay.: Oral leiomyosarcoma. Report of a case and review of the literature, pertaining to smooth muscle tumours of the oral cavity. Oral Surg. 43 (1977) 402
Fein, J.: Ein Leiomyom des Gaumens. Arch. Laryng. and Rhinol. 17 (1905) 533
Frenkel, G.: Auftreten eines Leiomyofibroangioms in Wangen- und Jochbogenbereich. Dt. Zahn~.rztl. Z. 20 (1965) 168
Galili, D., A. Shteyer: Leiomyoma of the oral cavity. J. Oral Med. 29 (1974) 69
Garrett, J. R.: Angiomyoma of the palate. Report of a case. Oral Surg. Oral Med. Oral Path. 27 (1969) 103

Oral Leiomyomas J. max.-fac. Surg. 10 (1982) 235
Glas, E.: Beitr~ige zur Pathologie der Zungengrundtumoren. Wiener Kiln. Wochenschrift 18 (1905) 747
Goldblatt, L. I., R. B. Edesess: Central leiomyoma of the mandible. Oral Surg. Oral Med. Oral Path. 43 (1977) 591
Gombos, F., Mazzarella, G., G. De Rosa: Su di un caso di leiomioma vascolare del pavimaento della bocca. Arch. Stomatol. (Napoli) 17 (1976) 205
Gorlin, R. J., H. M. Goldman: Oral Pathology. Mosby. St. Louis 1970 pp. 889
Gutmann, J., C. Cifuentes, M. A. Balzarini, V. Sobarzo, R. Vicuna: Angiomyoma of the oral cavity. Oral Surg. 38 (1974) 209
Hagy, D. M., V. Halparin, C. Wood: Leiomyoma of the oral cavity. Review of the literature and report of a case. Oral Surg. Oral Med. Oral Path. 17 (1964) 748
Herzog, M.: A case of myoma of the skin. J. of Cut. and Gen.Urin. Diseases. 18 (1898) 747
Janssen, L. H.: Leiomyoma curls. Acta. Derm. Vener. 32 (1952) 40 Kelly, D. E., W. F. Harrigan: Leiomyoma of the tongue. J. Oral Surg.
35 (1977) 316 Kimbraugh, R. A.: Malignant myomata and related tumours of the
uterus. Surg. Gyn. and Obstet. 30 (1920) 225 Kist, R. S., S. N. Bhaskar: Leiomyoma of the palate. J. Oral Surg. 22
(1964) 346 Kohn, E. M., D. C. Dahlin, J. B. Erich: Primary neoplasms of the hard
and soft palates and the uvula. Mayo Clinic Proceed. 38 (1963) 233 Lucas, Ro B.: Pathology of tumours of the oral tissues. Churchill,
London. 1 st Ed. 1964 MacDonald, D. G.: Smooth muscle turnouts of the mouth. Br. J. OraI
Surg. 6 (1969) 207 Manhold, J. D., J. L. Doyle: Leiomyoma of the oral cavity. Oral Surg.
Oral Med. Oral Path. 25 (1968) 729 Masuda, N., K. Kawai, M. Ishihura, L Takeyama: A case of leiom-
yoma of the lower lip and a discussion of statistical observations. Jibiinkoka Rinsho 52 (1980) 355
McGowan, D. A., J. H. Jones: Angiomyoma (vascular leiomyoma) of the oral cavity. Oral Surg. Oral Med. Oral Path. 27 (1969) 649
Merrill, R. G., J. R. Downs: Oral leiomyomas: report of two cases. Oral Surg. Oral Med. Oral Path. 23 (1967) 438
Miles, A. E. W., J. P. Waterhouse: Leiomyosarcoma of the oral cavity. J. Path. (Bact.) 83 (1962) 551
Nakamura, H., M. Kanai, M. Tokita, Y. Matsumoto, K. Seto, M. Niiyama, S. Sugawara: Two cases of angiomyoma of the palatal region. Tsurumi Shigaku 4 (1978) 123
Papadrianos, E.: Vascular leiomyoma of the oral cavity. J. Oral Med. 29 (1971) 69
Peter, K.: Epulis w~ihrend der Schwangerschaft. Dt. Zahn-, Mund- und Kieferheilk. 4 (1937) 412
Pettini, P.: Su un raro caso di leiomyoma della guancia. Ann. Stomat. (Roma) 14 (1965) 965
Pindborg, J. J.: Atlas of diseases of the oral mucosa. Munksgaard, Kopenhagen, 1968
Rao, Ch. B., M. J. Venkateswarlu: Leiomyoma of the palate. Ind. Dent. Assoc. 47 (1975) 115
Ravindranathan, N., I. H. Heslop: Oral leiomyoma. A case report and review of the literature. Br. J. Oral Surg. 16 (1978) 93
Reichart, P., H. Reznik-Schiiller: The ultrastructure of an oral angioma. J. of Oral Path. 6 (1977) 25
Rhatigan, R. M., Z. E. Kim: Leiomyoma arising adjacent to a maxil- lary tooth socket. S. Med. J. 69 (1976) 493
Robinson, E. C., A. M. Whyte: Leiomyosarcoma of the cheek. A case report. Br. J. of Oral Surg. 16 (1978) 100
Sehrt, E.: Subcutane Leiomyome der Wange und ihre Histogenese. Bruns Beitr. Klin. Chir. 54 (1907) 723
Sharer, W. G., N. K. Hine, B, N. Levy: Textbook of oral Path. 3 rd Ed. Saunders, Philadelphia - London 1974
Stout, A. P.: Leiomyoma of the oral cavity. Cancer 34 (1938) 31 Stout, A. P.: Bizarre smooth muscle tumour of the stomach. Cancer 15
(1962) 4O0 Stout, A. P., W. T. Hill: Leiomyosarcoma of the superficial soft tissues.
Cancer 11 (1958) 844 Utz, W.: Beitrfige zur Klinik und Pathologie des Leiomyoms in der
Mundh6hle. Stoma 18 (1965) 190 Visscher, J. G. A. M. de: Lipomas and fibrolipomas of the oral cavity.
J. Max.-Fac. Surg. 10 (1982) 177 Watabe, T., T. Morishima: A rare case of leiomyoma at the root of the
tongue. Otolaryng. Tokyo 35 (1963) 147 Well, I.: Ein Leiomyom der Uvula. Monatschr. fiir Ohrenheilk. 48
(1914) 1002 Weisinger, E., E. Doyle, M. J. Ladov: Leiomyoma of the oral cavity. J.
of the New Jersey Dental Society 40 (1969) 355 Yannopoulos, K., A. P. Stout: Smooth muscle tumours in children.
Cancer 15 (1962) 958
F. R. Praal, D.M.D. Department of Oral and Maxillofacial Surgery St. Radboud Hospital Geert Groote plein Zuid i4 Nijmegen Holland